
Abstract
Background:
The incidence of differentiated thyroid cancer (DTC) is low in Cuba, and the contribution of dietary factors to DTC in this population has not been investigated so far. The aim of this study was to evaluate the relationship between dietary iodine intake and DTC with regard to the interaction with environmental factors or some common single nucleotide polymorphisms (SNPs), based on a case-control study carried out in Cuba.
Methods:
A total of 203 cases and 212 controls from the general population were interviewed face-to-face using the dietary intake questionnaire and the photo booklet from the E3N cohort. A specific food composition table was constructed for this study. For each parameter studied, the odds ratio (OR) was stratified on age group and sex, and further adjusted for dietary energy, smoking status, ethnic group, level of education, number of pregnancies, and body surface area.
Results:
The risk of DTC was significantly reduced with increasing consumption of fish (p = 0.04), but no association between total dietary iodine intake and DTC risk was evident (p = 0.7). This lack of significant association was true whatever the age, the smoking status, the dietary selenium intake, and the ethnicity (p > 0.05). DTC risk was positively and strongly associated with the number of copies in the minor allele (A) for SNP rs965513 near FOXE1 among people who consumed less iodine than the median (p = 0.005).
Conclusion:
Overall, the majority of the studied population had an optimal dietary iodine intake. DTC risk was inversely associated with high fish consumption. Furthermore, DTC risk was positively associated with the number of copies in the minor allele (A) of rs965513 among people who consumed less iodine than the median. Because these findings are based on post-diagnostic measures, studies with pre-diagnostic dietary iodine are needed for confirmation.
Introduction
I
The incidence of differentiated thyroid cancer (DTC) is lower in African populations and higher in island populations, particularly in volcanic regions of islands (8,9). Cuba is an island of 100,000 km2 where 35% of the population belong to the African ethnic group (10). Before colonization by Spain, Cuba was occupied by Native Americans who had migrated from the mainland of North, Central, and South America several centuries before (11). Although thyroid cancer is the sixth most common female cancer in Cuba, its incidence is quite low. Indeed, while in North America the world age-standardized rate (ASR) of DTC incidence was 10.0/100,000 in white females during the period 1998–2002 (12), the ASR of DTC incidence in Cuba was around 4.1/100,000 for females and was even sixfold less frequent in males in 2009 (13). For other Latin American countries such as Colombia, the ASR of DTC incidence was 9.4/100,000 in females during the period 1998–2002 (12). Why is DTC incidence low in Cuba? Is this situation related to dietary iodine intake or other dietary factors?
Up to now, no clear explanation for the low incidence of DTC in the Cuban population has been established. Globally, the only highlighted risk factors for developing thyroid cancer are radiation exposure, having a family history of thyroid cancer, residing in an iodine-deficient area, large body size, and a high number of pregnancies (14 –16). The effect of alcohol, green tea, coffee, and other food groups or nutrients on the risk of developing thyroid cancer has also been investigated, but no significant associations have been identified (6,17).
It has been established that in endemic goiter areas with insufficient iodine intake, the incidence of follicular thyroid cancer is higher than elsewhere (18). However, this has not been replicated in papillary cancer, which currently represents >80% of DTCs in most countries, and 93% of the cases in this study, although overall goiter prevalence by palpation and inspection was 17.6% in Cuba, which corresponds to a mild endemic goiter area. However, the median urinary iodine concentration (UIC) of Cuban schoolchildren 6–11 years of age was 176 μg/L in 2011 and 2012 (19), which reflects adequate iodine intake (20), attributable to successful salt iodization. Nevertheless, until now, there has been no evidence to prove that iodine supplementation or excess dietary iodine intake in general decrease papillary DTC risk. The debate, however, is complicated because iodine content in food is very variable and, for the same food, depends on soil, agricultural techniques, and meal preparation. In addition, iodine is very volatile, and its measurement is still a challenge (4). For example, iodine content in cabbage was estimated to be 0.000427 mg/100 g in Cuba (ANSES 2014 food composition table), but 0.0007 mg/100 g in France (CIQUAL 2013 table) (21), and between 0.00026 and 0.00037 mg/100 g in Cameroon, depending on the samples (22). These variations exist for all foods, even those rich in iodine such as shellfish. The iodine content ranged from 0.056 mg/100 g depending on the type of shellfish in France (CIQUAL 2013 table) (21) to 0.50 mg/100 g in the Marshall Islands (23). In addition, iodine deficiency may also occur from interaction with other factors such as foods that are rich in isothiocyanates (24).
Traditional Cuban food includes staple food such as potato, taro, yam, vegetable banana, rice, and spaghetti; meat such as chicken, pork, beef, and ham; eggs; vegetables such as watercress, lettuce, tomato, red bean, and cabbage; fruits such as guava, mango, papaya, and banana; and fish or seafood such as sardine, tuna (canned or fresh), lobster, crab, shrimp, and shellfish. However, it is not clear whether dietary factors contribute to thyroid cancer risk in the Cuban population.
Both NK2 homeobox 1 (NKX2-1, also called TTF1 for Thyroid Transcription Factor 1) and Forkhead factor E1 (FOXE1, also called TTF2 for Thyroid Transcription Factor 2) play a crucial role in the development of the thyroid gland, and their expression is modified in thyroid tumors (25 –28). The single nucleotide polymorphism (SNP) rs944289 of the NKX2-1 gene was reported to increase the risk of DTC (29, 30). The SNP rs965513, rs1867277, and rs71369530 near or within the FOXE1 gene were identified in previous genome-wide association studies (GWASs) as being associated with an increased risk of DTC (29 –33). This study thus sought to investigate the contribution of genetic variations at the NKX2-1 and FOXE1 loci to the risk of DTC in the Cuban population.
To the best of the authors' knowledge, this observational study is the first to investigate dietary factors in the Cuban population. The aims were to explore the role of specific food groups or items, especially in regard to iodine intake, in the risk of developing DTC, and to assess the possibility of interaction between environmental factors and some common SNPs previously associated with DTC in the Cuban population. It was hypothesized, first, that fish consumption may reduce the risk of DTC; second, that dietary iodine deficiency and excess dietary iodine could be associated with an increasing risk of DTC; and third, that dietary iodine deficiency may interact with FOXE1 due to its role in thyroid hormone pathways.
Materials and Methods
This population-based case-control study was carried out in Havana, Cuba. A detailed methodology and the results of the analysis of non-dietary risk factors have already been published (34).
Consent
The Clinical Research Ethics Committee of the National Institute of Oncology and Radiobiology (INOR; Havana, Cuba) revised and approved this study. Informed written consent was obtained from all the study participants.
Study participants
All patients aged between 17 and 60 years who were living in Havana and its surrounding areas and who were treated for DTC between 2003 and 2010 at INOR and at the Institute of Endocrinology, Havana, were eligible for the study. Potential cases were selected from the National Cancer Registry databases (C73 ICD-10) and were cross-referenced with the INOR Pathology Register. On average, around 25–30 patients corresponding to these criteria were identified for each year of the study period. Among the 240 eligible DTC cases, 37 (15%) individuals were not interviewed because they had an unknown address (n = 32) or refused to participate (n = 5). The final study population consisted of 203 cases.
A total of 229 controls were selected from the general population living in Havana city and its surroundings using consultation files from primary-care units (family doctors) and from workplaces with a general practitioner. Each control was frequency matched with each case by age (±5 years) and sex. Of the 229 potential controls, 17 refused and 212 agreed to be interviewed (Fig. 1).
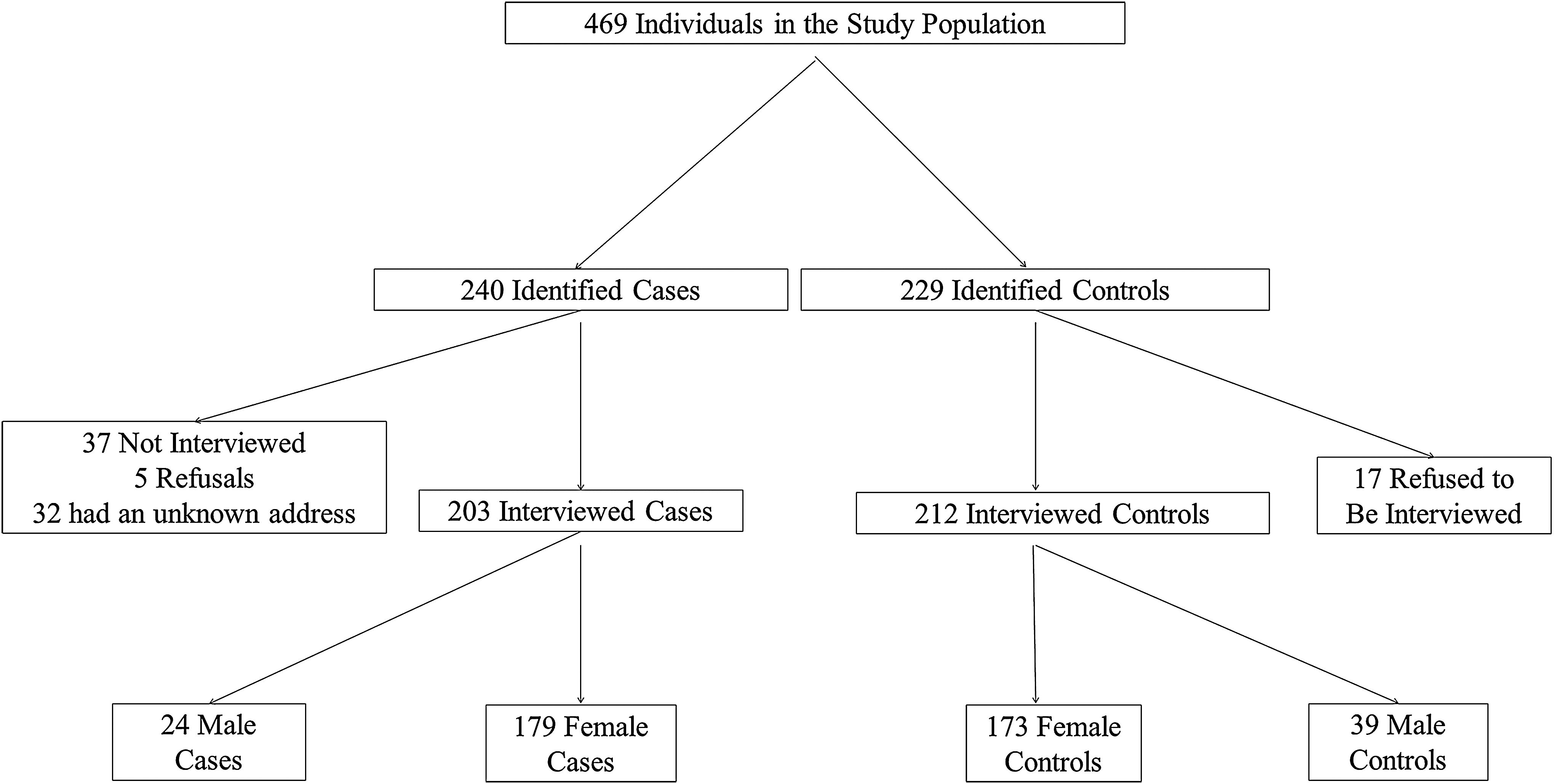
Participant flow chart of inclusion criteria, Cuba, 2009–2012.
Between July 2009 and January 2012, both cases and controls were interviewed face-to-face by trained professionals (nursing and medical staff) using a structured questionnaire. A standardized questionnaire was used to collect data on demographic characteristics (age, sex, place of residence, occupation), blood group and rhesus factor, anthropometric parameters, reproductive and hormonal history, lifestyle (smoking habits, alcohol consumption), exposure to radiation or chemicals, personal medical history and family medical history, and dietary intake in first-degree relatives. The dietary intake questionnaire is divided into two parts. The first part focuses on the general dietary intake, and the second part addresses the typical Cuban dietary intake more specifically. This questionnaire quantifies consumption by frequency and portion sizes per food group or food item. In addition, the photo booklet from the E3N cohort was used, which provides more detailed qualitative information on separate items within one food group (35). A saliva sample was also collected from the study participants.
Assuming a prevalence of exposure close to 30%, the size of this study (about 200 cases and 200 controls) allowed us to reach a power of 80% for identifying the role of a risk factor associated with an odds ratio (OR) of 1.8 when accepting a type I error of 5%.
Measures of iodine and selenium in food
The composition of 20 (28%) traditional Cuban food items was measured by the French Agency for Food, Environmental and Occupational Health & Safety (ANSES). It is noteworthy that the ANSES uses an innovative technology for determining total iodine (4). This technology is based on a European standard (36) that involves alkaline extraction using tetramethylammonium hydroxide (TMAH), optimized with an additional enzymatic treatment for samples containing starch, and followed by inductively coupled plasma mass spectrometry (ICP-MS) analysis. A complete single-laboratory validation was performed according to the accuracy profile approach (37,38) based on tolerance intervals to select the best calibration function and to determine the validated concentration ranges. This method was used to determine the iodine and selenium content in the main foods consumed by Cubans (Supplementary Figs. S1 and S2; Supplementary Data are available online at
The composition of the remaining 51 (72%) food items of other general food consumed by cases and controls, and included in the diet questionnaire, was estimated using the CIQUAL 2013 table (21).
For each food item in the diet questionnaire, total intake of iodine and selenium consumption were estimated by multiplying the daily consumption of each food by the iodine or selenium content in this food based on ANSES 2014 (Supplementary Table S1) or CIQUAL 2013 food composition tables (21) (if iodine or selenium content were measured from several similar foods in the composition tables, the mean of the iodine or selenium content in these similar foods was taken).
An item for quantifying iodized salt intake in the questionnaire was not included. In fact, since 2005, Cuba has established compulsory iodization of salt for human consumption for the whole Cuban population because a global strategy at the national level is the best solution for a cost-effective prevention and control of iodine deficiency (5). A fixed value of 10 g of iodized salt per person per day was included. This value was estimated to be the average consumption of iodized salt per inhabitant per day by the Center for Nutrition and Food Hygiene, the National Institute of Hygiene, Epidemiology, and Microbiology (Inhem) of Cuba.
Analyzed parameters
For quantitative factors, such as fish, shellfish, and total seafood consumption, the study participants were categorized into tertiles according to the consumption value distribution in controls.
Overall, the study participants were classified into three categories according to the Iodine Global Network (IGN) (39): mild iodine deficiency (75–149 μg/day), optimal iodine intake (150–299 μg/day), and more than adequate or excess iodine intake (≥300 μg/day). Furthermore, the study participants were regrouped into quartiles according to the dietary iodine intake in controls.
The possible interaction between dietary iodine intake and the following polymorphisms was investigated: rs944289 (near NKX2-1), rs965513 (near FOXE1), rs1867277 (5′ UTR of FOXE1), and rs71369530 (polyalanine length polymorphism in FOXE1), which were significantly associated with the risk of developing DTC in the same Cuban case-control study (40). For this purpose, the values of dietary iodine intake were classified into two categories: either less or more than the median (186 μg/day) value observed in controls.
Statistical analysis
Nineteen strata were defined on the basis of age and sex: seven for men and twelve for women. For each parameter studied, the OR stratified on age group and sex, and adjusted for dietary energy, smoking status, ethnic group, level of education, number of pregnancies, and body surface area (BSA), was estimated using conditional logistic regression with SAS v9.3 (SAS Institute, Inc., Cary, NC). Linear trend tests were performed by creating a variable that assigned the median value for each category of the studied variable consumption, and this variable was then modeled as a continuous variable. Likelihood ratio tests comparing models with and without multiplicative interaction terms were performed to assess the significance of interactions. Sensitivity analyses were performed by excluding individuals diagnosed more than five years before the interviews.
Results
The majority of the population in this Cuban case-control study were females (88%) with DTC diagnosed between 2000 and 2011. The mean age at diagnosis was 38 years (range 17–60 years). Almost all (93.1%) DTCs were papillary carcinomas (Table 1). The risk of DTC reduced significantly with increasing consumption of fish (p = 0.04; Table 2).
DTC, differentiated thyroid cancer.
Mantel–Haenszel chi-square test stratified on age group and sex.
Multivariate logistic regression stratified on age group and sex, and adjusted for dietary energy, smoking status, ethnic group, level of education, number of pregnancies, body surface area, and, for trend test, calculated by assigning the median value to each category and treating this variable as a continuous variable.
Reference category.
OR, odds ratio; CI, confidence interval.
It was observed that only 15% of the studied population samples were estimated as having mild iodine deficiency, and the majority (78%) of the studied population had an optimal dietary iodine intake according to the IGN classification. No significant association was identified between dietary iodine intake, when classified according to the IGN classification, and DTC risk in the entire Cuban sample (p = 0.5; Table 3). This association was still not significant (p = 0.7) when the population sample was regrouped by quartiles of dietary iodine intake in controls (Supplementary Table S2). Furthermore, this non-significant association was not modified by age, smoking status, dietary selenium intake, or ethnicity (p > 0.05; Supplementary Table S2).
Calculated using the Wald test for dietary iodine intake modeled as a continuous variable (per classification).
Reference category.
Crude p-trend.
Stratified on age group and sex, and adjusted for dietary energy, smoking status, ethnic group, level of education, number of pregnancies, and body surface area.
Adjusted p-trend.
No interaction was found between dietary iodine intake and the polymorphisms rs944289, rs1867277, and rs71369530 in the risk of developing DTC. Conversely, a strong interaction (p = 0.005) was identified between dietary iodine intake and rs965513, near the FOXE1 gene on chromosome 9q22.33 (Table 4). A strong increased DTC risk was observed with the number of copies in the minor allele (A) of rs965513 among people who consumed less iodine than the median (<186 μg/day). The risk of DTC was 3.4 times higher (p = 0.0005 [confidence interval (CI) 1.7–6.5]) for subjects carrying one copy of the A allele, and 6.7 times higher (p = 0.0005 [CI 1.6–27.3]) for subjects carrying two copies of the A allele when compared with the reference group of subjects with no copies in the minor allele (A). This dose effect with regard to the DTC risk with the increasing number of copies in the A allele was not observed in subjects consuming more iodine than the median (>186 μg/day). Independent of the number of copies in the minor allele (A), the risk of DTC was around three times higher than that of the reference group whose subjects were not carrying any A allele and had a dietary iodine intake below the median (Table 4).
Missing data: two cases and four controls with dietary iodine intake <median, and four cases and three controls with dietary iodine intake >median due to low quality of samples for genotyping.
p-Value between the number of A allele in FOXE1 and dietary iodine intake (+ or – median), crude = 0.007, stratified = 0.003, multivariate = 0.005.
Reference category.
Mantel–Haenszel chi-square test.
Mantel–Haenszel chi-square test stratified on age group and sex.
Multivariate logistic regression stratified on age group and sex, and adjusted for dietary energy, smoking status, ethnic group, level of education, number of pregnancies, body surface area, and for trend test, calculated by assigning the number of A allele in FOXE1.
An interaction that was close to significance was identified between dietary iodine intake and body mass index (BMI; p = 0.08). Among people whose BMI was ≥25 kg/m2, the risk of DTC was 2.47 times higher (multivariate odds ratio [OR] = 2.47 [CI 0.89–6.85]) in people who were in the lowest quartile of dietary iodine intake compared with those who were in the highest quartile, although this difference was not significant (p = 0.1). This increase of DTC risk when decreasing iodine intake was not observed in people with a BMI <25 kg/m2 (Supplementary Table S2).
Discussion
It was observed that the risk of DTC significantly decreased with increasing consumption of fish in the Cuban population. In addition, a strong increase in DTC risk was found with the number of copies in the minor allele (A) of rs965513 near FOXE1 on chromosome 9q22.33 among people who consumed less than the median value of iodine in controls. Furthermore, the risk of DTC tended to be higher among people whose BMI ≥25 kg/m2 and who were in the lowest quartile of dietary iodine intake.
The increasing number of eligible DTC cases in this study from the first six years (n = 50) to the last three years (n = 89) was not related to technical developments in thyroid cancer diagnosis (e.g., fine-needle aspiration). For cases diagnosed closer to the year of their interview (between July 2009 and January 2012), the reason was that their clinical and personal dossiers were more easily obtained. Furthermore, the charts contained more precise information, and therefore these cases were more likely to fulfill the inclusion criteria.
The present study is the first case-control study to focus on the risk factors of DTC in the Cuban population. The food photo booklet from the E3N cohort (35) was used in this study in order to estimate the portions of food and drink daily consumption by the participants, which complemented the quantificational questionnaire and gave us normative, accurate, and qualitative information on which to build the database. Another noteworthy point is that a special food composition table was constructed to measure the quantity of iodine in typical Cuban food for this study. However, only 28% of the food items in the questionnaire of this study were measured using this special and innovative table.
As with any case-control study, this study has some limitations. Self-reported food consumption is associated with imprecise measures and recall bias. Another limitation is that for a large part of the Cuban diet, iodine content was estimated from the CIQUAL 2013 food composition table, which had been established for French food, and may not be applicable to Cuban food. Moreover, because cases usually take more care of their health and are more motivated to participate in research studies than controls, the cases may have reported more precise information than the controls did, and this could have introduced a differential bias in the final results and overestimated the risk of DTC. Nevertheless, this potential bias cannot explain the significant relation between the number of copies in the minor allele (A) of rs965513 and the risk of DTC among people who consumed less iodine than the median. Indeed, it is very unlikely that the finding regarding an interaction between SNP rs965513 and iodine intake was due to chance because it remained present when correcting the p-value for the number of SNPs tested, which was four SNPs in the analyses (41). Additionally, this result was almost exactly identical when adjusting or not for other DTC risk factors and stratifying or not for age groups and sex. Lastly, recall bias was probably reduced by the fact that food import and export limitations exist in Cuba, which keeps the typical Cuban food more stable and less diversified than Western food.
The French CIQUAL 2013 food composition table was used in this study in order to evaluate the iodine content in fish and shellfish. This could introduce some uncertainties. Nevertheless, the iodine content in fish is highly variable even in one country (42). It depends strongly on the species and the places of capture, and most of the sea fish consumed in Cuba are from areas far away from Cuban coasts. Given the low number of fish captured by Cuban boats and low fish consumption in Cuba, the difficulty in measuring the iodine content in fish, and the cost-effectiveness of this study, the iodine content was not measured in either Cuban fish or shellfish. This study shows that in the Cuban population, the risk of DTC significantly decreased with the increasing consumption of fish at the time of the interview (Table 2). This important finding is in line with another case-control study, which was carried out in French Polynesia (43). A meta-analysis of 19 observational studies on dietary factors and thyroid cancer risk summarized the ORs for each risk factor. Based on the highest level of total consumption versus the lowest level, the aggregate OR [CI] of thyroid cancer was 0.79 [0.66–0.94] for fish consumption. Subgroup analysis showed that fish (OR = 0.74 [CI 0.59–0.92]) and shellfish (OR = 0.46 [CI 0.27–0.75]) consumption has a protective effect in iodine-deficient areas (44). Another related review showed that iodine-rich food such as fish and shellfish may provide a protective role in populations with insufficient daily iodine intake (6). In contrast, a Japanese cohort where subjects were followed up for a mean of 14.5 years showed that a high intake of seaweed was positively associated with thyroid cancer risk, although this result was not statistically significant. In addition, a high intake of seaweed was positively associated with papillary thyroid cancer risk in postmenopausal women (especially for papillary carcinoma, the hazard ratio [HR] for almost daily consumption compared with ≤2 days/week was 3.81 [CI 1.67–8.68]; p < 0.01) (45).
First-degree relatives of DTC patients have an increased risk for developing thyroid cancer, and a positive family history is reported in approximately 5% of cases (46 –49). These observations strongly suggest the contribution of genetic factors to the susceptibility to the disease. Six potential regions for harboring a high-risk DTC gene have been identified through family-based linkage studies in the early 2000s: MNG1 (14q32) (50), TCO (19p13.2) (51,52), fPTC/PRN (1q21) (53), NMTC1 (2q21) (54), FTEN (8p23.1-p22) (55), and the telomere–telomerase complex (56). More recently, population-based studies, particularly GWASs, have identified and replicated susceptibility loci at 9q22, 14q13, 2q35, and 8p12 (57). In a previous study, in the same sample of the Cuban population, the association was validated between DTC risk and variants of genes localized at 9q22.33 (FOXE1) and 14q13.3 (NKX2-1) (40). The FOXE1 locus is the most widely replicated susceptibility locus associated with DTC risk in a number of population-based studies of various ethnic origins, especially associated with sporadic and radiation-related papillary thyroid cancer and also with familial nonmedullary thyroid carcinoma (58,59).
This case-control study has for the first time identified a strong increase in DTC risk associated with the number of copies in the minor allele (A) of SNP rs965513, near FOXE1 at 9q22.33, among people who consumed less iodine than the median, but no variation in people who consumed more (p = 0.005). To the best of the authors' knowledge, gene–environment interactions in DTC have only been investigated in relation to radiation exposure in a candidate gene approach, but no convincing association has been reported so far. In particular, no gene–environment interaction study has investigated an association with FOXE1 (at 9q22.33) and dietary iodine intake.
According to the IGN classification, an optimal iodine intake corresponds to 150–299 μg/day (39). The quartiles of the dietary iodine intake in the controls in this study were: <164.9, 164.9–186.5, 186.5–237.5, and ≥237.5 μg/day. The last three quartiles cover the optimal iodine intake, as well as more than adequate or excess iodine intake. However, a case-control study using a food frequency questionnaire is not an adequate way to estimate iodine status (because a case-control study without iodine measurement in urine is not designed to estimate the iodine status of a population, but to perform comparisons between the cases and the controls). Nevertheless, the majority of the studied population had an optimal dietary iodine intake. If this result was confirmed by other studies, it would emphasize the effectiveness of the compulsory public health policy by using iodized salt in urban, rural, and mountainous areas of Cuba. A cross-sectional study to assess the effectiveness of this program through determination of UIC and goiter prevalence has been previously completed in Cuban schoolchildren aged 6–11 years in 2011–2012. The results of this study by Terry-Berro et al. showed that the median UIC was 176.3 μg/L (19). Only 7.6% of the children showed iodine deficiency (2.2% had severe deficiency <50 μg/L) and 15.3% had an UIC >300 μg/L. The prevalence of optimal iodine nutrition was 43.5% (52.5% in mountain areas). The overall goiter prevalence was 17.6%, which reflects mild endemic goiter. However, in mountain areas, the prevalence of goiter was 32.6% (severe endemic goiter). The authors concluded that iodine deficiency is no longer a public health problem in urban and rural areas of Cuba, which is attributable to successful salt iodization. Nevertheless, high goiter rates are still observed in mountain areas.
In a comprehensive synthesis of animal and human studies (7), Zimmermann et al. concluded that iodine deficiency increases DTC risk. However, the present study does not have enough participants in the moderate iodine deficiency group to verify this conclusion with sufficient statistical power.
In conclusion, the majority of the studied population had an optimal dietary iodine intake. Although DTC risk was not found to be linked to dietary iodine intake in this study, DTC risk significantly decreased with high fish consumption. Additionally, DTC risk significantly increased with an increasing number of copies in the minor allele (A) of rs965513 near FOXE1 among people who consumed less iodine than the median. Because these findings are based on post-diagnostic measures, studies with pre-diagnostic dietary iodine are needed for confirmation.
Footnotes
Acknowledgments
We sincerely acknowledge the Ligue Nationale Contre le Cancer (LNCC), the Région Ile de France, and the Institut National du Cancer (INCA) for funding this research project. We extend special gratitude to Fondation de France for funding the first author, Yan Ren, for her PhD study, and we sincerely thank the Région Ile de France for the grant to Constance Xhaard.
Author Disclosure Statement
The authors state that no competing financial interests exist.