
Abstract
Background:
The goal of eliminating iodine deficiency worldwide was successfully achieved in China after the implementation of a mandatory universal salt iodization program for the last 16 years. Thus, China has been assessed as a country with more than adequate iodine levels. This survey aimed to investigate the current iodine status in China and the effects of an increased iodine intake on the spectrum and prevalence of thyroid disorders.
Methods:
A total of 15,008 adult subjects from 10 cities in eastern and central China were investigated. Serum thyrotropin (TSH), thyroid peroxidase antibodies (TPOAb), thyroglobulin antibodies (TgAb), and urine iodine concentration (UIC) were measured, and an ultrasonography of the thyroid was performed in all subjects. Free thyroxine (fT4) and free triiodothyronine (fT3) levels were only measured if the serum TSH was outside the normal range.
Results:
The median UIC values were 197 μg/L in school-age children (SAC) and 205 μg/L in a cohort population. Six cities were classified as regions with adequate iodine intake (AII), and four cities as regions with more than adequate iodine intake (MTAII), according to median SAC UIC. The prevalence of clinical hypothyroidism, subclinical hypothyroidism, and positive thyroid antibodies was significantly higher in MTAII cities than it was in AII cities. Moreover, the prevalence of clinical hyperthyroidism (1.1% vs. 0.8%, p = 0.033) and Graves' disease (0.8% vs. 0.5%, p = 0.019) also significantly increased in MTAII cities. Compared with a five-year prospective study conducted in 1999, the prevalence of goiter significantly decreased (2.9% vs. 5.02%, p = 0.001), but there was a significant increase in thyroid nodules (12.8% vs. 2.78%, p = 0.001). The prevalence of subclinical hypothyroidism (16.7% vs. 3.22%), positive TPOAb (11.5% vs. 9.81%), and positive TgAb (12.6% vs. 9.09%) significantly increased, while no changes were seen in clinical hyperthyroidism, subclinical hyperthyroidism, or Graves' disease.
Conclusion:
The goal of eliminating iodine deficiency has been successfully achieved in China. However, the prevalence and spectrum of thyroid disorders has increased, reflecting possible adverse effects of increased iodine intake.
Introduction
C
Materials and Methods
Cities
Ten cities were chosen according to their historical median UIC in SAC that was representative of AII and MAII status. They were located in the eastern and central parts of China, which have a collective total population of 60 million and include Shenyang (SY), Beijing (BJ), Jinan (JN), Xi'an (XA), Chengdu (CD), Nanjing (NJ), Shanghai (SH), Wuhan (WH), Guiyang (GY) and Guangzhou (GZ; Fig. 1).
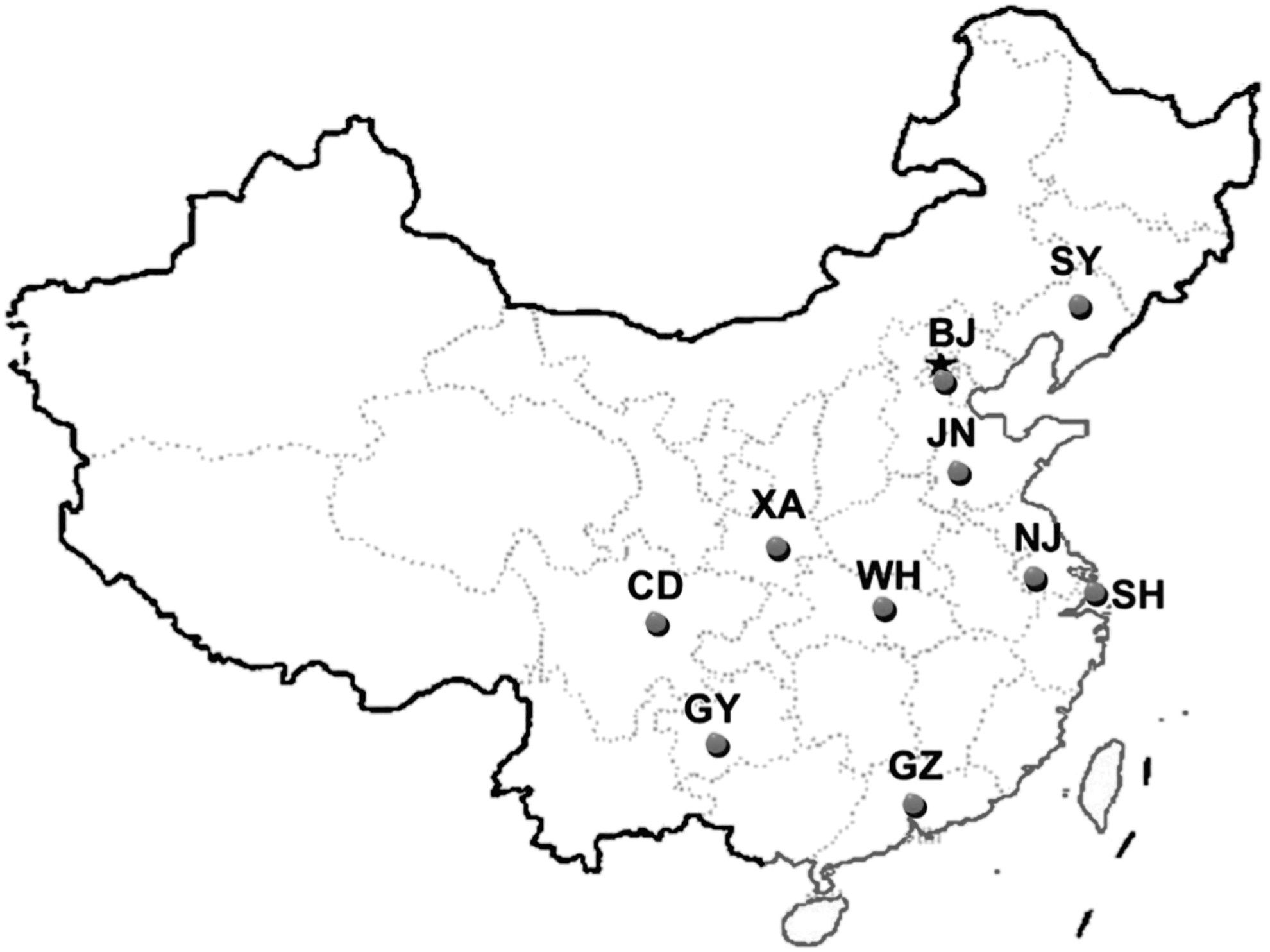
The distribution of 10 cities investigated in China.
Subjects
One or two communities were randomly chosen from each city. The designed cohort included 1500 individuals from each city, giving a total of 15,008 participants across the 10 cities. To avoid recruitment bias, the inhabitants in the community were screened according to their household registers. The participants were enrolled in the cohort in line with the designed age composition. The average participant age was 45.5 years (standard deviation [SD] = 14.9; range 15–92 years). The sample was stratified by age to reflect the age range of the Chinese population (National Bureau of Statistics in China in 2008). Thus, the age groups 15–29, 30–39, 40–49, 50–59, 60–69, and ≥70 comprised 17.1%, 22.3%, 22.4%, 19.6%, 10.3%, and 8.3% of the total study population, respectively. The ratio of men to women was 1:1.4, since fewer men lived at home.
The 10 city cohorts were similar in age and sex, but differed in iodine intake. Exclusion criteria included residing in the city for <10 years, age <15 years, pregnant or lactating, or any medical regimen affecting thyroid function such as antithyroid drugs, thyroid hormones, glucocorticoids, dopamine, or amiodarone. A reference population was selected according to Guideline 22 of the National Academy of Clinical Biochemistry, that is, without medications, detectable thyroid autoantibodies, a personal or family history of thyroid dysfunction, and goiter or nodules on thyroid ultrasonography (5). The 60 urine samples from SAC in each community were measured for UIC, and 10 samples of household salt and drinking water (tap water) in each community were measured for iodine concentration.
Survey protocols
Participants were visited at home, and an oral questionnaire was administered as previously described (4), which collected personal information and data on the economic status of the family, eating habits, type of salt used, smoking status, and personal or family history of thyroid disease. Fasting blood and urine samples were collected between 8:00am and 10:00am. All samples were stored at −20°C and transferred within one month of collection to the laboratory in the project center for centralized measurements. Physicians who had received centralized training performed all thyroid ultrasonography evaluations using a portable instrument (LOGIQ a50, 7.5 MHz; GE Healthcare). Table 1 shows the diagnostic criteria for thyroid disorders used in this study.
Reference ranges were taken from the manufacturer. Method: electrochemiluminescence performed on a Cobas 601 analyzer (Roche Diagnostics).
TSH, thyrotropin; fT4, free thyroxine; TPOAb, thyroid peroxidase antibodies; fT3, free triiodothyronine; TgAb, thyroglobulin antibodies.
Laboratory methods
Serum thyrotropin (TSH), thyroid peroxidase antibodies (TPOAb), and thyroglobulin antibodies (TgAb) were measured in all participants. Free thyroxin (fT4) and free triiodothyronine (fT3) levels were only measured if TSH was outside the reference range. The laboratory reference ranges provided by the manufacturer were used in this study: TSH 0.27–4.2 mIU/L, fT4 12–22 pmol/L, fT3 3.1–6.8 pmol/L, TPOAb 0–34 IU/L, and TgAb 0–115 IU/L. Measurements were done using electrochemiluminescence immunoassays on a Cobas 601 analyzer (Roche Diagnostics). The functional sensitivity of serum TSH was 0.002 mIU/L. The intra-assay coefficients of variation (CV) of serum TSH, fT4, fT3, TPOAb, and TgAb were 1.1–6.3%, and the inter-assay CV values were 1.9–9.5%. UIC was determined in all participants by the ammonium persulfate method based on the Sandell–Kolthoff reaction (6). The reference range of the certified reference material (GBW09109) from the Center for Disease Control (CDC) in China was 138 ± 10 μg/L, and the result measured by the central laboratory was 134.3 ± 6.2 μg/L. The intra- and inter-assay coefficients of variation for UIC were 3–4% and 4–6% at 66 μg/L and 2–5% and 3–6% at 230 μg/L.
Statistical analysis
All statistical analyses were performed using SPSS Statistics for Windows v17.0 (SPSS, Inc.), and values of p < 0.05 were considered significant. The data were tested for normality using the Kolmogorov–Smirnov test. UIC was not normally distributed, therefore the median and interquartile ranges are reported. The chi-square test was used to compare the prevalence of thyroid disorders between different regions and years.
Medical ethics
The research protocols were approved by the medical ethics committee of China Medical University (serial number: IRB[2008]34). All subjects provided written informed consent.
Results
As shown in Table 2, the median UIC values were 197 μg/L in SAC and 205 μg/L in the total cohort population. According to the median UIC of SAC, six cities (SY, BJ, JN, CD, SH, and GZ) were classified as AII regions (median UIC 172.8 μg/L in SAC), and four cities (GY, NJ, WH, and XA) as MTAII regions (median UIC 239.5 μg/L in SAC). The average iodine concentrations in the drinking water were 6.55 μg/L in AII and 3.18 μg/L in MTAII. The average iodine concentration in household salt was 29.1 mg/kg in AII and 28.4 mg/kg in MTAII.
MUI, median UIC.
Table 3 shows the proportion of UIC in the cohort population. The percentages of the populations with UIC <50 μg/L and <100 μg/L were 3.23% and 16.04% in AII and 1.49% and 8.26% in MTAII, respectively. In the whole cohort, the percentages of the populations with UIC <50 μg/L and <100 μg/L were 2.78% and 12.23%, respectively. In women of child-bearing age (20–45 years), median UIC was 215.43 μg/L, with 2.78% UIC <50 μg/L and 24.55% UIC <150 μg/L.
Table 4 shows the significantly higher prevalence of thyroid disorders in MTAII cities than in AII cities, including overt hyperthyroidism (1.1% vs. 0.8%, p = 0.33), overt hypothyroidism (1.3% vs. 1.0%, p = 0.033), subclinical hypothyroidism (22.6% vs. 12.7%, p < 0.001), Graves' disease (0.8% vs. 0.5%, p = 0.019), positive TPOAb (12.4% vs. 10.9%, p = 0.004), and positive TgAb (13.4% vs. 12.0%, p = 0.04), except for subclinical hyperthyroidism (0.8% vs. 0.8%, p = 0.095). However, the prevalence of goiter was significantly lower (1.0% vs. 4.3%, p < 0.001) and the prevalence of thyroid nodules was significantly higher (14.5 vs. 10.4%, p < 0.001) in MTAIII cities than it was in AII cities.
Comparison of the prevalence of thyroid disorders between the cities with adequate iodine intake and the cities with more than adequate iodine intake.
A remarkable change was found in the prevalence of subclinical hypothyroidism (TSH >4.2 mIU/L), which was unexpectedly higher in both regions (12.7% in AII and 22.6% in MTAII). Of the individuals with subclinical hypothyroidism, 20.6% were TPOAb positive and 21.2% were TgAb positive. On the contrary, the prevalence of subclinical hypothyroidism in individuals with TPOAb positivity was 36%, while that of TgAb positivity was 33.8%. The prevalence of TPOAb and TgAb positivity in the whole cohort population was 11.5% and 12.0%, respectively, with a higher prevalence in women than in men (14.8% vs. 7.0%, p < 0.001; TgAb 18.1% vs. 5.1%, p < 0.001).
Table 5 shows the prevalence of thyroid disorders found in this study compared with the results reported in 1999 (5). As reported by most studies, the prevalence of the hyperthyroidism and Graves' disease decreased significantly (0.89% vs. 1.68%, p = 0.001 for hyperthyroidism; 0.61% vs. 1.25%, p = 0.001 for Graves' disease). An increased prevalence was found in subclinical hypothyroidism (16.7% vs. 3.22%, p = 0.001) without a change in clinical hypothyroidism (1.03% vs. 1.11%, p = 0.69). The prevalence of TPOAb and TgAb positivity also increased significantly (11.5% vs. 9.81%, p = 0.003 for TPOAb; 12.6% vs. 9.09%, p = 0.001 for TgAb). The prevalence of goiter in this study decreased significantly (2.9% vs. 5.02%, p = 0.001), but the prevalence of thyroid nodules increased (12.8% vs. 2.78%, p = 0.001).
Chemiluminescence immunoassays were used and the kits were provided by the Diagnostic Products Corporation. Reference intervals were: TSH 0.3–4.8 mIU/L, fT4 10.3–24.5 pmol/L, fT3 2.3–6.3 pmol/L, TPOAb 7.0–50 IU/L, TgAb 10–40 IU/L.
Comparison of the prevalence of thyroid disorders in the total population between 1999 and 2011.
Discussion
It has been 25 years since the United Nations World Summit for Children established the goal of eliminating iodine deficiency worldwide in 1990 (3). Substantial progress has also been made in China as a participating country in this regard. There have been four stages in the implementation of USI in China (2). First, a non-mandatory salt iodization program conducted only in the iodine-deficient regions between 1954 and 1995 increased the national median UIC to 164.8 μg/L. Second, mandatory USI implemented throughout China in 1996 led to a status of excessive iodine intake between 1997 and 2001, as documented for example in 1997 (median UIC 330.2 μg/L) and in 1999 (median UIC 306 μg/L) in the general population. Third, the national mandate for salt iodization was revised by the central government in 2002, and decreased iodine intake to more than adequate levels of 241.2 μg/L in 2002 and 246.3 μg/L in 2005. Finally, a new national decree (GB-26878-2011) for salt iodization was launched in 2012 in which the concentration of iodine in salt was decreased to 20–30 mg/kg at the household level, while the provincial governments were authorized to set the local iodine concentration in salt to within ±30% of the recommended level to account for the natural background iodine level (7).
This cross-sectional study is the largest scale survey (n = 15,008) to date on the correlation of iodine status with thyroid disorders in China. It has the following advantages. First, it was conducted after the implementation of persistent and mandatory iodine iodization in China for 16 years and the effect of increased iodine intake on the prevalence of thyroid disorders had become evident and stable. Second, the cohorts were derived from 10 cities that were classified as AII and MTAII regions and located in the eastern and middle part of China. Third, the age composition of the cohorts was set according to the data of a national population report at the same period. Fourth, all urine and serum samples were measured in the central laboratory using the same kits and instruments.
The current iodine status in China is reported in this study. As shown in Tables 3 and 4, the median UIC was 197 μg/L in SAC and 205 μg/L in the cohort population. The proportion of median UIC <100 μg/L was 12.63%, with a 2.4% goiter prevalence in the cohort population. These results are consistent with the survey recently reported by the Institute of Iodine Deficiency Disorders, Center for Endemic Disease Control, and Chinese Center for Disease Control and Prevention from the same period (2011), which showed a national median UIC of 238.6 μg/L in SAC (2). Across China, 14 provinces had adequate iodine intake, 13 had more than adequate iodine intake, and four had excessive iodine intake. The coverage rate of iodized salt was 98%, with 95.3% of qualified iodine concentration in iodized salt (2). All of the above results demonstrate that the goal of eliminating iodine deficiency in China has been successfully achieved, and China has been assessed as a country of more than adequate iodine intake by the World Health Organization (3).
It is widely accepted that iodine intake has a dual effect on the thyroid. Insufficient iodine intake can cause iodine-deficient disorders, while too much iodine intake also results in thyroid disorders. In 1999, a baseline study was conducted that compared cohorts with a different iodine intake (median UIC 84 μg/L, 243 μg/L, and 651 μg/L). The prevalences were 0.3%, 0.9%, and 2.0% for overt hypothyroidism and 0.9%, 2.9%, and 6.1% for subclinical hypothyroidism, respectively, which showed a significantly increased prevalence with an increasing iodine intake. The same trend also occurred in the prevalence of autoimmune thyroiditis of 0.5%, 1.7%, and 2.8%, respectively (4). The adverse effects of an increased iodine intake were confirmed again in the present study. The prevalences of clinical hypothyroidism, subclinical hypothyroidism, and positive thyroid antibodies were significantly higher in MTAII cities than they were in AII cities, although the difference in median UIC was only 51 μg/L (235 μg/L vs. 184 μg/L, respectively). Moreover, the prevalences of clinical hyperthyroidism (1.1% vs. 0.8%, p = 0.033) and Graves' disease (0.8% vs. 0.5%, p = 0.019) were also significantly higher in MTAII cities than they were in AII cities, a finding that was not seen in our previous study (4). The same results were also reported by the CDC study in China. Liu et al. found an increased prevalence in EII and AII regions compared with iodine-deficient regions (20.09%, 10.41%, and 2.25% for subclinical hypothyroidism; 8.15%, 6.09%, and 2.55% for autoimmune thyroiditis, respectively) though in a small sample size (n = 861) (2).
An increased prevalence of thyroid disorders has been found in the study presented here after mandatory USI for 16 years in China (Table 5). Compared with the five-year prospective study, the prevalence of subclinical hypothyroidism (16.7% vs. 3.22%), positive TPOAb (11.5% vs. 9.81%), positive TgAb (12.6% vs. 9.09%), and thyroid nodule (12.8% vs. 2.73%) significantly increased, while a decreased prevalence was seen in clinical hyperthyroidism, subclinical hyperthyroidism, goiter, and Graves' disease (4). These findings indicate the effects of long-term mandatory salt iodization on thyroid disorders. Lombardi et al. determined the effects of 15-year iodine prophylaxis on the prevalence of thyroid disorders in a small rural area (Pescopagno) in Italy (8). Compared with results before prophylaxis, a significant increase in the prevalences of overt hypothyroidism (2.8% vs. 5.0%), subclinical hypothyroidism (0% vs. 8.4%), and Hashimoto thyroiditis (3.5% vs. 14.5%) were found, but the prevalence of goiter decreased from 46.5% to 25.8% (8). In the DanThyr study, the incidence of spontaneous hypothyroidism was significantly higher in Copenhagen than it was in Aalborg (40.6/100,000 vs. 29.0/100,000), with a minor difference in median UIC (61 μg/L vs. 45 μg/L) (9). Miranda et al. reported a significant decrease in the prevalence of autoimmune thyroiditis (11.7% vs. 5.3%) in school children in Brazil when their median UIC decreased from 459.6 μg/L (2003) to 165 μg/L (2015) (10). Pedersen et al. reported the effect of iodine fortification on thyroid antibodies, which increased the median UIC of one cohort from 61 μg/L to 101 μg/L. The prevalence of TPOAb positivity increased from 14.3% to 23.8%, while that of TgAb positivity increased from 13.7% to 19.9% (11). Zolis et al. showed a significantly higher prevalence of autoimmune thyroiditis (9.6% vs. 3.3%) in children in Greece when their median UIC increased from 84 μg/L to 202 μg/L (12).
A remarkable change was found in the prevalence of subclinical hypothyroidism compared with the five-year prospective study (16.7% vs. 3.22%, respectively) (4). However, the individuals with subclinical hypothyroidism had only a 20.6% TPOAb positivity rate and a 21.2% TgAb positivity rate, which indicates that most of the subclinical hypothyroidism did not result from thyroid autoimmunity. This may be attributable to increased serum TSH levels. In an animal model, it has previously been shown that high levels of iodine may inhibit iodothyronine deiodinase activity in the hypothalamus and/or pituitary, decreasing the conversion of T4 to T3 and disrupting the negative feedback regulation, thereby increasing TSH secretion (13).
This study has some limitation. First, this cross-sectional study does not permit changes in the prevalence of thyroid disorders over time in the study's subjects to be assessed. Second, the comparative data in 1999 and in 2011 are based on two different cohorts, although the thyroid parameters were measured using the same method.
In conclusion, the iodine nutrition status in China has greatly improved, and the aim of eliminating iodine deficiency has been successfully achieved. However, the prevalence and spectrum of thyroid disorders has increased, reflecting possible adverse effects of increased iodine intake. Therefore, the importance of ongoing monitoring of the population iodine status and keeping the iodine intake at an optimal and safe level must be emphasized.
Footnotes
Acknowledgments
This work was supported by the International Cooperation Foundation of the Ministry of Health of the People's Republic of China (2009); the Guanghua Science and Technology Foundation of China (Grant 2007-02); the Research Foundation of Innovative Team in Advanced Educational Institute (Grant LT201215); the Foundation of Science and Technology for Universities in Liaoning Province; and the Foundation for The Key Laboratory in Liaoning Province (2010).
Author Disclosure Statement
The authors hereby confirm that no part of this manuscript has been published or is under consideration for publication elsewhere. The authors have no potential conflicts of interest to declare.