
Abstract
Background:
The management of patients with differentiated thyroid carcinoma (DTC) showing low levels of serum thyroglobulin autoantibodies (TgAb) and undetectable Tg after thyroidectomy is unsettled. This study sought to elucidate the clinical significance of low levels of TgAb and to evaluate their interference with Tg measurement in vitro.
Methods:
Tg and TgAb levels were correlated with the post-thyroidectomy staging of 177 consecutive DTC patients undergoing 131I ablation after total thyroidectomy (clinical study). Tg was measured by an immunometric assay (functional sensitivity: 0.1 ng/mL), and TgAb were evaluated by six assays (functional sensitivities: 1.2–96 IU/mL; positive cutoffs: 4–150 IU/mL). The changes in Tg concentration (Tg recovery) of diluted specimens from DTC patients were also measured after incubation with 67 sera from DTC patients with undetectable Tg and low levels of TgAb (in vitro study). DTC sera containing Tg were diluted serially (from 330 to 0.1 ng/mL) and incubated with TgAb samples; Tg was then measured.
Results:
In the clinical study: all patients had residual thyroid tissue, and 10 had metastatic disease. Depending on the TgAb assay, median Tg values were 7.0–10.9, 0.0–5.3, and 0.0–0.0 ng/mL in patients with undetectable, borderline (between functional sensitivities and positive cutoffs), and positive TgAb, respectively (p < 0.001). An undetectable Tg value was associated with borderline levels of TgAb in five assays. Only two patients with metastatic disease had undetectable Tg; both were TgAb positive by three or more assays. Conversely, no patient with undetectable Tg and undetectable or borderline TgAb by sensitive assays had metastatic disease. In the in vitro study, TgAb interfered significantly with Tg recovery (p < 0.001), but low levels of TgAb did not abolish Tg recovery.
Conclusions:
While low levels of TgAb do not preclude Tg measurement in vitro, they can be associated with an undetectable Tg in DTC patients with residual thyroid tissue after thyroidectomy. However, the finding of low levels of TgAb by sensitive assays associated with an undetectable Tg rules out metastatic disease.
Introduction
T
Recently, the management of DTC patients showing low levels of TgAb after thyroidectomy has arisen as a critical issue. Some studies set the threshold for interference with Tg measurement below the positive cutoffs of TgAb assays, which are established in cohorts of patients with autoimmune thyroid disease (13 –15), and close to their analytical sensitivities (11). According to these findings, two different thresholds for TgAb can be defined: one for the effects on Tg measurement (“interfering” cutoff), and another for the diagnosis of autoimmune thyroid disease (“positive” cutoff). Thus, in addition to positive TgAb, borderline (i.e., between functional sensitivities and positive cutoffs) TgAb would render the results obtained by Tg IMAs unreliable, challenging the definition of the clinical status of a large number of DTC patients (11,16).
This study evaluated the relevance of low levels of TgAb in the diagnostic work-up of DTC patients. To this purpose, the in vivo interference was evaluated by correlating the results of serum Tg (measured by IMA) and TgAb with the staging of a large cohort of DTC patients bearing residual thyroid tissue and possible metastatic disease after total thyroidectomy. TgAb were measured by six different assays because of the well-known variability in TgAb assays (9,11,12,17,18). In addition, the in vitro interference of TgAb by Tg recovery studies was evaluated. In these experiments, the changes in Tg concentration observed in samples from DTC patients with detectable Tg (and undetectable TgAb) were calculated after incubation with sera from clinically free of disease DTC patients without evidence for disease but containing low levels of TgAb and undetectable Tg.
Patients and Methods
Study group
Cohort for determination of TgAb levels interfering with Tg measurement in vivo
Samples were obtained from 177 consecutive, unselected DTC patients (median age 47.0 years; interquartile range [IQR] 37.0–54.0 years; 135 females) referred to the Endocrinology Unit, University Hospital of Pisa, Italy, between 2007 and 2009. The tumor stage, established according to the 2002 TNM classification (19), was as follows: 80 patients T1, 31 patients T2, 64 patients T3, 2 patients T4; 117 patients Ta, 60 patients Tb; 152 patients N0, 25 patients N1; 174 patients M0, 3 patients M1. Sera were collected from patients before 131I thyroid remnant ablation, after thyroid hormone withdrawal, about three months after total thyroidectomy. All patients had a neck ultrasound and a 24 h 131I (activity: 50 μCi) uptake of thyroid bed. A whole-body scan (WBS) was performed after the administration of 131I activity of 30–100 mCi. Metastatic lymph nodes were diagnosed by ultrasound, fine-needle biopsy (for cytological evaluation and Tg measurement), and WBS. Distant metastases were diagnosed by WBS and computed tomography scan.
Samples for determination of the in vitro interference of TgAb on Tg measurement
Sera were obtained from four patients with metastatic DTC, who had undetectable serum TgAb and Tg levels of 49,950 (Tg1), 719 (Tg2), 698 (Tg3), and 670 ng/mL (Tg4), respectively. Additional sera were collected between 2012 and 2013 from a cohort of 67 DTC patients, clinically free of disease, with undetectable Tg and borderline (i.e., between functional sensitivities and positive cutoffs) or slightly positive TgAb (by IMA1, see below). As a control, sera were pooled from subjects who were clinically free of disease and had undetectable Tg and undetectable TgAb (control sera-CS-pool).
Written informed consent to phlebotomy and for the use of serum samples was obtained from all subjects involved in the study. The Institutional Review Board of the Endocrinology Unit approved the study.
In vitro interference of TgAb on Tg measurement
Tg sera were diluted to Tg concentrations of 330, 100, 33, 10, 3.3, 1.0, 0.33, and 0.1 ng/mL (five specimens from Tg1, 24 from Tg2, 21 from Tg3, and 17 from Tg4 for a total of 67 specimens for each concentration). Each diluted sample was then randomly assigned to incubation (1:1) for 3 h at 37°C with one of the 67 DTC sera containing borderline (>8 and ≤30 IU/mL, n = 39) or slightly positive (n = 28) TgAb. The percent change of Tg levels after incubation with TgAb sera was calculated according to the formula:
Thyrotropin, Tg, and TgAb assays
Thyrotropin (TSH) was determined by Immulite 2000 (Euro/DPC, Gwynedd, United Kingdom; normal values 0.4–3.6 μIU/mL). Tg was measured by an IMA, the Access Thyroglobulin assay (Beckman Coulter, Inc., Fullerton, CA; functional sensitivity 0.1 ng/mL, analytical sensitivity 0.05 ng/mL). The intra-assay coefficient of variation of the Tg assay ranged from 2.2% (at Tg 100 ng/mL) to 7.7% (at Tg 0.1 ng/mL). TgAb were checked by three non-competitive IMAs: AIA-Pack 2000 TgAb (Tosoh Corporation, Tokyo, Japan; IMA 1), Immulite 2000 anti-Tg Ab (Siemens Medical Solutions Diagnostics, Los Angeles, CA; IMA 2), Access Thyroglobulin Antibody (Beckman Coulter Inc.; IMA 3); and three competitive radioimmunoassays (RIAs): SelCo anti-Tg (Medipan, GMBH, Berlin, Germany; RIA 1), BRAHMS anti-Tgn (BRAHMS, Hennigsdorf, Germany; RIA 2), and RADIM TgAb One Step CT (RADIM S.p.A, Rome, Italy; RIA 3). The analytical sensitivities, the functional sensitivities, and the positive cutoffs were 6.0, 8.0, and 30 IU/mL (IMA 1); 20, 20, and 40 (IMA 2); 0.9, 1.2, and 4 (IMA 3); 20, 96, and 150 (RIA 1); 20, 40, and 60 (RIA 2); and 20, 49, and 70 (RIA 3). TgAb values between functional sensitivities and positive cutoffs were considered as borderline (>8 and ≤30 for IMA1, >20 and ≤40 for IMA 2, >1.2 and ≤4 for IMA3, >96 and ≤150 for RIA1, >40 and ≤60 for RIA2, and >49 and ≤70 for RIA3).
Statistical analysis
The number of detectable Tg and TgAb levels were compared by the chi-square test. Tg concentrations were compared by the Kruskal–Wallis test. Receiver operating characteristic (ROC) curve analyses were performed to identify the best cutoff for each TgAb assay that better discriminated between undetectable and detectable Tg in terms of sensitivity and specificity (i.e., highest Youden index). Sensitivity was defined as the percentage of samples with undetectable Tg that had a TgAb level greater than the cutoff, while specificity was the percentage of samples with detectable Tg that had a TgAb level lower than the cutoff. Spearman's correlation (rho) was used to quantify the association between TgAb levels and Tg recovery in in vitro experiments. Post hoc comparisons were performed using the Bonferroni correction of significance.
Data are reported as median and interquartile range (IQR) or mean values along with confidence intervals (CI). Statistical significance was assumed for p-values <0.05.
Results
Clinical features of the patients
Clinical features of the cohort of patients have been extensively reported previously (12). TSH values were 54.0 mIU/L (39.0–75.0 mIU/L) after thyroid hormone withdrawal. Neck ultrasound and 24 h uptake of 131I showed a remnant tissue in the thyroid bed in all patients; thyroid volume on ultrasound was 0.1 mL (0.0–0.5 mL), and neck uptake was 5.5% (2.0–10.1%). One patient had bone metastasis, one lung metastasis, one both lung and lymph node metastases, and seven lymph node metastases. Because of the persistence of thyroid tissue, Tg was expected to be detectable in all patients.
Tg values and TgAb levels
Tg was undetectable in 49 and detectable in 128 patients. Figure 1 shows the number of patients with undetectable, borderline, and positive TgAb by the six assays, in relation to Tg results. Of the 49 patients with undetectable Tg, 7 (by IMA1 and IMA2) to 30 (by RIA2) had undetectable TgAb and 15 (by RIA2) to 31 (by IMA1) had positive TgAb. Four to 12 patients (8.2–24.5%) with undetectable Tg and 0–39 patients (0.0–30.5%) with detectable Tg had borderline TgAb.

Thyroglobulin autoantibodies (TgAb) in patients with undetectable and detectable Tg. Percent and number of patients with undetectable, borderline and positive TgAb by six assays in 49 patients with undetectable Tg (
Tg values were significantly different in patients with undetectable, borderline, or positive TgAb according to the results of the six assays (p < 0.001; Table 1). Compared with patients with undetectable TgAb, Tg values were lower in patients with borderline TgAb and (according to the results of the three IMAs, but not the three RIAs) even lower in those with positive TgAb.
Median and interquartile range of Tg values are reported.
p < 0.001.
≤8 IU/mL. c>8 and ≤30 IU/mL. d>30 IU/mL.
≤20 IU/mL. f>20 and ≤40 IU/mL. g>40 IU/mL.
≤1.2 IU/mL. i>1.2 and ≤4 IU/mL. l>4 IU/mL.
≤96 IU/mL. n>96 and ≤150 IU/mL. o>150 IU/mL.
≤40 IU/mL. q>40 and ≤60 IU/mL. r>60 IU/mL.
≤49 IU/mL. t>49 and ≤70 IU/mL. u>70 IU/mL.
Tg, thyroglobulin; TgAb, thyroglobulin autoantibodies; IMA, immunometric assay; RIA, radioimmunoassay.
Correlation between TgAb levels and undetectable Tg value in vivo
For each TgAb assay, the value that correlated with an undetectable Tg (in vivo “interfering cutoff”) was established by ROC curve analysis (Fig. 2 and Table 2). They were lower than the positive cutoffs in all TgAb assays, with the exception of IMA2 (41 vs. 40 IU/mL). The interfering cutoff of RIA1 was below the functional sensitivity of the assay, while those of RIA2 and RIA3 were 0.0 IU/mL. Compared to positive cutoffs, the interfering cutoffs showed a higher sensitivity and a lower specificity (Table 2).

Receiver operating characteristic curve analysis of TgAb levels correlated with undetectable Tg. TgAb results by six assays were correlated with undetectable Tg in 177 differentiated thyroid carcinoma patients at the time of thyroid remnant ablation. , positive cutoff;  , interfering cutoff.
, interfering cutoff.
p < 0.0001.
Below the functional sensitivity of the assay.
TgAb value for the diagnosis of autoimmune thyroid diseases, according to manufacturers.
TgAb value that better discriminated between undetectable and detectable Tg according to sensitivity and specificity by receiver operating characteristic curve analysis.
Values are means with confidence intervals.
Tg values, TgAb levels, and postoperative clinical staging
Out of 10 patients with metastatic disease, Tg was detectable in eight (range 2.5–106 ng/mL) and undetectable in two, one with distant metastasis and one with metastatic lymph nodes (Table 3). The first patient had positive TgAb by the three IMAs, below the analytical sensitivity of the assays by RIA1 and RIA2 and undetectable by RIA3; the second patient had positive TgAb by all six TgAb methods. Conversely, among patients with undetectable Tg, those with undetectable TgAb (7 by IMA1, 7 by IMA2, and 12 by IMA3) or borderline TgAb (11 by IMA1, 12 by IMA2, and 9 by IMA3) by the three more sensitive assays (Fig. 1A) showed all residual thyroid tissue.
Values below the functional sensitivity of the assays are reported in italics.
At whole-body scan.
At neck ultrasound and fine-needle aspiration biopsy.
Skull metastasis.
Lung metastases.
In vitro interference of TgAb on Tg measurement
Tg recovery after incubation of diluted samples from Tg1, Tg2, Tg3, and Tg4 sera with the 39 sera with borderline (>8 and ≤30 IU/mL) TgAb and the 28 with slightly positive TgAb (by IMA1) are reported in Figure 3. A significant inverse correlation between TgAb levels and percent of Tg recovery was observed at all Tg concentrations (rho values from −0.69 to −0.47; p < 0.001). This correlation became non-significant when the analysis was restricted to sera with borderline TgAb (rho values from −0.28 to 0.15; p = 0.09–0.99). The number of samples showing interference (Tg recovery exceeding the intra-assay coefficient of variation) ranged from 50 (at Tg concentration of 330.0 ng/mL) to 62 (at Tg concentrations of 0.1 and 0.33 ng/mL). An underestimation of Tg values was observed in the majority of cases, while a few samples showed an overestimation of Tg values, in particular for lower TgAb levels. Tg was detectable in all samples, with the exception of one sample with a Tg concentration of 0.33 ng/mL and 29 with a Tg concentration of 0.1 ng/mL, which showed an undetectable Tg. Recovery was similar for Tg1, Tg2, Tg3, and Tg4 samples.
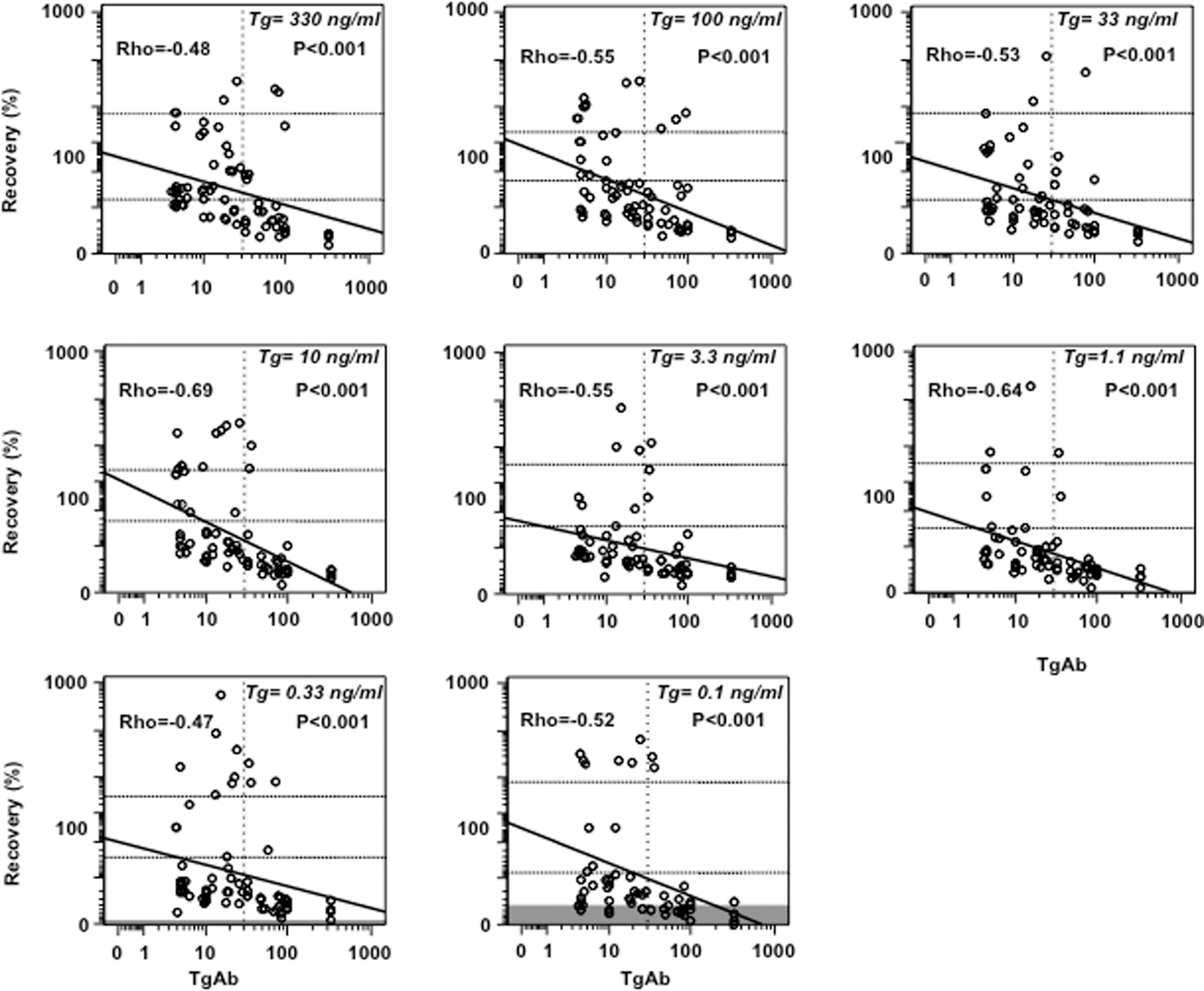
Correlation between TgAb levels by immunometric assay 1 (IMA1) and Tg recovery at different Tg concentrations. x-Axis, TgAb levels; y-axis, % recovery according to the formula:
Discussion
Tg is the specific marker for the presence of thyroid tissue, being produced by normal follicular cells as well as follicular cell-derived DTC. Follow-up evaluations of DTC patients consist in serial measurements of stimulated Tg (after levothyroxine withdrawal or recombinant human TSH administration) along with neck ultrasound (4,5). In DTC patients treated with total thyroid ablation (thyroidectomy followed by 131I thyroid remnant ablation), the finding of an undetectable Tg associated with a negative neck ultrasound indicates remission of DTC (4,5,20,21). According to recent studies, measurement of basal (unstimulated) Tg by second-generation IMAs, which have a functional sensitivity of 0.05–0.1 ng/mL, seems as effective as the measurement of a stimulated Tg after total thyroid ablation (22 –25). For patients with low-risk DTC, who form the majority of patients with thyroid cancer, the recent guidelines recommend a more conservative approach (less then total thyroidectomy or total thyroidectomy without 131I thyroid remnant ablation) (5). Preliminary data suggest that changes in unstimulated Tg levels over time are as reliable in these patients as they are in patients who underwent remnant ablation (6,7).
A major drawback associated with the measurement of Tg is the possibility of assay interference by coexistent TgAb (4,5,12,26,27). Indeed, all series evaluating Tg in DTC are restricted to cohorts of patients with negative or undetectable TgAb (6,7,25,28,29). Positive TgAb are suggestive of autoimmune thyroid disease (13 –15,30,31). They are encountered in 7.5–25% of DTC patients (8 –10) as expression of associated autoimmune thyroid disease or an immune reaction to thyroid carcinoma (32). TgAb can be used as a surrogate marker for Tg measurement, as they reflect the persistence of thyroid tissue. Indeed, changes in TgAb levels correlate with the clinical status of DTC patients (33,34) and their disappearance with the absence of residual thyroid tissue (10). However, the reliability of TgAb measurement is greatly hampered by the high variability of results yielded by different TgAb assays (9,11,17,18). Among DTC patients showing undetectable Tg despite harboring residual thyroid tissue after total thyroidectomy, the proportion of patients with positive TgAb ranged from 30.6% to 63.3%, according to the results obtained with six commercial assays (12).
Because of the effect of TgAb on Tg IMAs, it has been proposed to use either RIA or tandem mass spectrometry for the measurement of Tg if TgAb are present (11,12), methods that are supposedly resistant to TgAb (16). In addition, recent data highlight that TgAb thresholds for interference with the measurement of Tg are significantly lower than the corresponding positive cutoffs (11), which are established in cohorts of patients with autoimmune thyroid disease (13,14,27). Accordingly, the Tg levels of a large number of DTC patients should be measured with Tg RIAs or Tg mass spectrometry rather than with Tg IMAs. However, the functional sensitivities of Tg RIAs and Tg mass spectrometry are higher (0.5–1.0 ng/mL) compared with ultrasensitive Tg IMAs. Furthermore, Tg RIA can yield falsely positive results in the presence of TgAb (35), and mass spectrometry for Tg is expensive, limited to a few centers, and has yet to be clinically validated (16,36).
In this context, the clinical significance of low levels of TgAb in DTC patients after thyroidectomy was elucidated. The authors have recently reported Tg concentrations (by IMA) and TgAb levels (by three IMAs and three RIAs) in these patients (12). Although ultrasound and/or WBS showed residual thyroid tissue in all 177 patients, Tg was undetectable in 49 of them (12). The proportion of undetectable Tg was higher in patients with positive TgAb than in those with negative TgAb, thus confirming the interference of TgAb with Tg measurements when measured by IMA. Among patients with undetectable Tg, TgAb were more frequently positive by the three IMAs than the three RIAs (37,38).
The present study sought to determine the clinical significance of low levels of TgAb in this cohort of patients. Among the 49 patients with undetectable Tg (as measured by ultrasensitive IMA), 4–12 (according to the six assays) had borderline (between functional sensitivities and positive cutoffs) TgAb. Tg values in patients with borderline TgAb were lower than in those with undetectable TgAb. All assays showed in vivo interfering cutoffs lower than positive cutoffs with the exception of IMA2, in which they were close to each other. The interfering cutoffs of RIA1, RIA2, and RIA3 were below their functional sensitivities, in keeping with their low sensitivity in picking up TgAb interfering with Tg measurement (12). These findings confirm that the degree of correlation of TgAb assays is low and that the conversion of results of different methods is unreliable. Therefore, TgAb should be measured by the same assay during the follow-up of DTC patients (27). In addition, IMAs seem to be more sensitive than RIAs in detecting TgAb interfering with Tg measurement (12).
When Tg and TgAb results were correlated with the postoperative staging, it was observed that of 10 patients with metastatic disease, Tg was detectable in eight, while in the two patients showing undetectable Tg, TgAb were positive by the three IMAs. On the other hand, patients with undetectable Tg and undetectable or borderline TgAb by the three IMAs (18 by IMA1, 19 by IMA2, and 21 by IMA3) had residual thyroid tissue only. These observations highlight that although in vivo interfering cutoffs are usually lower than positive cutoffs, low levels of TgAb (by sensitive assays) associated with undetectable Tg after thyroidectomy rule out metastatic disease. This conclusion adds to the well-known notion that Tg levels correlate with postoperative DTC staging and that undetectable Tg rules out metastatic disease (4,5,39).
In the second part of this study, the in vitro interference of TgAb on Tg measurement was investigated. To this end, the changes in Tg concentration observed in samples from DTC patients with detectable Tg (and undetectable TgAb) after incubation was calculated with sera from DTC patients who were clinically disease-free and who had an undetectable Tg and borderline or slightly positive TgAb. Tg recovery correlated directly with Tg concentrations and inversely with TgAb levels. Interference became non-significant for borderline TgAb. The finding of an excessive Tg recovery in some samples with borderline TgAb was somehow surprising but in keeping with previous observations by Spencer et al. (11) These results provide further evidence to discourage the use of a Tg recovery test (26), which is still employed by some commercial Tg assays.
Borderline TgAb (by sensitive assays) were associated with an undetectable Tg in 18–24% of patients in vivo, and in a few samples in vitro, at the lowest Tg concentration (0.1 ng/mL), which is close to the analytical sensitivity of the assay. The most likely reason for this discrepancy is the enhanced clearance of circulating Tg that can occur in vivo after the formation of Tg–TgAb complexes. This effect has been shown in animals (40), and probably takes place in humans as well (41). The Tg/TgAb ratio is the key factor in the clearance of Tg from circulation: while high levels of TgAb can clear a large amount of serum Tg, low levels of TgAb cannot remove a significant quantity of Tg. Therefore, low levels of TgAb (by sensitive assays) do not preclude the detection of Tg when it is produced in a considerable amount, as in patients with metastatic DTC, and do not significantly influence Tg results by IMA in vivo. These results support the reliability of Tg measurement by IMA in DTC patients showing low TgAb levels (when measured by sensitive assays). These patients do not require Tg measurement by other methodologies. This is relevant because of the huge increase in the incidence of patients with low risk DTC (3), not requiring 131I thyroid remnant ablation.
In conclusion, while low TgAb levels (by sensitive assays) interfere with but do not preclude Tg measurement in vitro, they can cause an undetectable Tg in patients with residual thyroid tissue. However, the finding of low TgAb levels associated with undetectable Tg rules out metastatic disease.
Footnotes
Acknowledgments
These studies were supported by the grant “Rientro dei cervelli” n. 311 from MIUR and University of Pisa to Francesco Latrofa.
Author Disclosure Statement
The authors have nothing to disclose.