
Abstract
Background:
Previous studies have examined the relationship between body mass index (BMI) and the behavior of papillary thyroid carcinomas (PTC). However, the results are inconsistent. The purpose of this study was to clarify the association between PTC behavior and anthropometric parameters including BMI and body surface area (BSA).
Methods:
This study retrospectively reviewed 5081 PTC patients who underwent total thyroidectomy with bilateral central neck dissection between January 2002 and June 2015. Because of sexual dimorphism in obesity, analyses were conducted separately for men and women. The World Health Organization BMI classification was used to classify patients as normal (18.5 ≤ BMI <25 kg/m2), overweight (25 ≤ BMI <30 kg/m2), or obese (BMI ≥30 kg/m2). Since no consensus for BSA categorization exists, enrolled patients were grouped into BSA quartiles by sex: women BSA1 (BSA <1.52 m2), BSA2 (1.52 ≤ BSA <1.59 m2), BSA3 (1.59 ≤ BSA <1.67 m2), and BSA4 (BSA ≥1.67 m2); and men BSA1 (BSA <1.77 m2), BSA2 (1.77 ≤ BSA <1.86 m2), BSA3 (1.86 ≤ BSA <1.96 m2), and BSA4 (BSA ≥1.96 m2).
Results:
In women, overweight (adjusted odds ratio [OR] = 1.187, p = 0.042) and obese (adjusted OR = 2.231, p < 0.001) were independent predictors for multiplicity. Furthermore, overweight (adjusted OR = 1.237, p = 0.012) and obese (adjusted OR = 1.789, p = 0.005) were independent predictors for extrathyroidal extension (ETE). However, higher BMI was not an independent predictor for bilaterality or central lymph node metastasis (CLNM). In addition, higher BSA—BSA3 (adjusted OR = 1.205, p = 0.049) and BSA4 (adjusted OR = 1.524, p < 0.001)—was an independent predictor for multiplicity. However, higher BSA was not a predictor for bilaterality, ETE, or CLNM. In men, higher BMI and BSA were not predictors for multiplicity, bilaterality, ETE, or CLNM.
Conclusions:
In women with PTC, higher BMI was an independent predictor for multiplicity and ETE. Furthermore, higher BSA was an independent predictor for multiplicity. However, BMI and BSA were not predictors for the PTC behavior in men.
Introduction
T
The prevalence of obesity is also increasing worldwide (4). A recent population-based cohort study of 5.24 million British adults found that body mass index (BMI) is associated with an increased risk of thyroid and 16 other cancers (5). Other studies have demonstrated that higher BMI is associated with poorer prognosis in several types of malignancies, including breast, prostate, and colon (6 –8).
Several studies have examined BMI and PTC behavior. However, their results are inconsistent. Paes et al. (9) suggested that higher BMI was significantly associated with decreased risk of tumor invasion and lymph node (LN) metastasis. In contrast, Kim et al. (10) found no significant association between BMI and PTC aggressiveness. Kim et al. (11), however, suggested that higher BMI was significantly associated with larger PTC tumor size, extrathyroidal extension (ETE), and advanced stage. Furthermore, Tresallet et al. (12) suggested that high BMI is an independent predictor of locoregional events in macrocarcinomas (tumor >1 cm).
Given these contradictory results, the purpose of this study was to clarify the association between PTC behavior and anthropometric parameters. Because of sexual dimorphism in obesity (13,14), analyses were conducted separately for men and women. Particularly since no study has examined the association between body surface area (BSA) and PTC, BMI and BSA were both assessed.
Materials and Methods
Patient selection
This study was approved by the Institutional Review Board at Samsung Medical Center. The medical records of 5081 patients with pathologically proven PTC who underwent total thyroidectomy with bilateral central neck dissection (CND) at the Thyroid Cancer Center of the Samsung Medical Center between January 2002 and June 2015 were retrospectively reviewed. Patients were excluded for any of the following factors: lack of BMI/BSA data, reoperation, age <18 years or >80 years, non-PTCs (follicular/medullary/anaplastic), mixed-type PTC, thyroid dysfunction (use of antithyroid drugs or thyroid hormones), abnormal serum thyrotropin (TSH) levels (<0.3 or >6.5 mIU/L) (11), presence of distant metastasis, history of lateral neck dissection, or follow-up duration less than six months (e.g., residual tumor or LN detected within six months of initial surgery, reoperation within six months, or loss to follow-up within six months).
Surgical strategy
Total thyroidectomy was performed for tumor size >1 cm, multifocality, bilaterality, ETE, or regional LN metastasis detected during preoperative or intraoperative examination, according to the American Thyroid Association (ATA) management guidelines (15). This study included both therapeutic and prophylactic CND. Therapeutic CND was performed when suspicious central LN metastasis (CLNM) was detected during preoperative or intraoperative examination. Prophylactic CND was performed on PTC patients with clinically uninvolved central neck LNs, in particular for advanced primary tumors (T3/T4) (15) or according to the surgeon's preference at the time of operation. CND was performed immediately after the completion of total thyroidectomy, and comprised removal of all nodes and fibro-fatty tissue extending vertically from the hyoid bone to the thoracic inlet and laterally from the medial border of the common carotid artery to the midline of the trachea. The recurrent laryngeal nerve was mobilized and skeletonized along the entire cervical course.
Measurement of anthropometric parameters
BMI (kg/m2) was defined as weight (kg) divided by height (m) squared. Enrolled PTC patients were categorized using standardized guidelines from the World Health Organization as normal (18.5 ≤ BMI <25 kg/m2), overweight (25 ≤ BMI <30 kg/m2), or obese (BMI ≥30 kg/m2). BSA was calculated using the formula developed by DuBois and DuBois (16): BSA (m2) = 0.007184 × W(kg)0.425 × H(cm)0.725. Since no consensus for BSA categorization exists, enrolled patients were grouped into BSA quartiles by sex: women (BSA1 [BSA <1.52 m2), BSA2 [1.52 ≤ BSA <1.59 m2], BSA3 [1.59 ≤ BSA <1.67 m2), and BSA4 [BSA ≥1.67 m2]) and men (BSA1 [BSA <1.77 m2], BSA2 [1.77 ≤ BSA <1.86 m2], BSA3 [1.86 ≤ BSA <1.96 m2], and BSA4 [BSA ≥1.96 m2]).
Histopathological examination
Surgical specimens were microscopically examined by two or more experienced pathologists. Assessed histopathologic factors were cell type of the main lesion, primary tumor size (measured as the longest diameter of the largest lesion), location, multiplicity, ETE, lymphovascular invasion, margin involvement, LN metastasis, and underlying thyroid conditions such as chronic lymphocytic thyroiditis (CLT). Multiplicity was defined as two or more PTC lesions in a single lobe, regardless of bilaterality.
Postoperative follow-up and management
After initial surgery, all patients underwent regular follow-up at 6- to 12-month intervals with clinical evaluations, including physical examinations, ultrasonography, computed tomography, iodine-131 (131I) scans, and serum thyroglobulin. After total thyroidectomy, TSH suppression therapy (serum TSH level <0.5 mIU/L) with levothyroxine with or without radioactive iodine (RAI) ablation was considered as an initial postoperative therapy. RAI ablation was performed with 131I after surgery according to ATA guidelines (17). RAI ablation was administered after thyroid hormone withdrawal or stimulation with recombinant TSH. Although RAI ablation was generally proposed for patients classified as having intermediate- to high-risk features for recurrence (e.g., older age, larger tumor size, ETE, LN metastasis, or individual histology predicting intermediate to high risk of recurrence), the final decision was made according to the physicians' or patients' preference. When RAI treatment was no longer needed, patients received regular follow-up. Loss to follow-up, withdrawal, and deaths were censored as of last date of follow-up. Suspicious lesions were confirmed by ultrasonography-guided fine-needle aspiration biopsy with or without measurement of washout thyroglobulin levels and/or a thyroid computed tomography or positron emission tomography/computed tomography. Since PTC has an extremely low mortality rate (18), the prognostic impact of BMI and BSA was assessed using locoregional recurrence defined as the presence of tumor or metastatic LN on cytology from aspiration biopsy or histopathology from reoperation, developing six months after initial surgery.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant. Continuous variables are presented as means ± standard deviations (SD), and comparisons between groups were analyzed using one-way analysis of variance. Categorical variables are represented as percentages and odds ratios (OR), and comparisons between groups were analyzed using linear-by-linear association. In multivariate analysis, multiple logistic regression was employed to determine whether BMI and BSA were independent predictors of multiplicity, bilaterality, ETE, and CLNM. Kaplan–Meier methods and the log-rank test were adopted for analysis of time-dependent variables.
Results
Association between clinicopathologic characteristics of women with PTC and anthropometric parameters at diagnosis
In women with PTC, a higher BMI was significantly associated with older age (p < 0.001), BRAF positivity (p < 0.001), large tumors (p < 0.001), multiplicity (p < 0.001), bilaterality (p < 0.001), ETE (p < 0.001), and a decreasing occurrence of CLT (p = 0.008; Table 1). However, a higher BMI was not significantly associated with TSH (p = 0.941) or CLNM (p = 0.555). A higher BSA was significantly associated with younger age (p < 0.001), large tumors (p = 0.036), multiplicity (p < 0.001), and bilaterality (p = 0.003; Table 2). However, a higher BSA was not significantly associated with BRAF positivity (p = 0.704), TSH (p = 0.558), ETE (p = 0.151), CLT (p = 0.849), or CLNM (p = 0.774). After adjusting for clinicopathologic characteristics in multiple logistic regression analysis (Table 3), a higher BMI was an independent predictor for multiplicity (overweight: adjusted OR = 1.187, p = 0.042; obese: adjusted OR = 2.231, p < 0.001) and for ETE (overweight: adjusted OR = 1.237, p = 0.012; obese: adjusted OR = 1.789, p = 0.005). However, a higher BMI was not an independent predictor for bilaterality or CLNM. A higher BSA was an independent predictor for multiplicity (specifically BSA3: adjusted OR = 1.205, p = 0.049; and BSA4: adjusted OR = 1.524, p < 0.001). However, a higher BSA was not a predictor for bilaterality, ETE, or CLNM.
Categorized by World Health Organization classification.
BRAF mutation analysis was started in 2008, and it was performed in 1525 women with PTC.
PTC, papillary thyroid carcinoma; BMI, body mass index; ETE, extrathyroidal extension; CLT, chronic lymphocytic thyroiditis; CLNM, central lymph node metastasis; NA, not available; SD, standard deviation.
Categorized by quartiles.
BRAF mutation analysis was started in 2008, and it was performed in 1525 women with PTC.
BSA, body surface area.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), bilaterality, ETE, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, ETE, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, bilaterality, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, bilaterality, ETE, and CLT.
Categorized by World Health Organization classification.
Categorized by quartiles.
OR, odds ratio; CI, confidence interval; Ref, reference.
Association between clinicopathologic characteristics of men with PTC and anthropometric parameters at diagnosis
In men with PTC, a higher BMI was significantly associated with older age (p = 0.003) and large tumors (p = 0.002; Table 4). However, a higher BMI was not significantly associated with BRAF positivity (p = 0.124), TSH (p = 0.559), multiplicity (p = 0.092), bilaterality (p = 0.720), ETE (p = 0.089), CLT (p = 0.433), or CLNM (p = 0.074). A higher BSA was significantly associated with older age (p < 0.001) and CLNM (p < 0.001; Table 5). However, a higher BSA was not significantly associated with BRAF positivity (p = 0.288), TSH (p = 0.263), large size tumor (p = 0.064), multiplicity (p = 0.443), bilaterality (p = 0.663), ETE (p = 0.929), or CLT (p = 0.615). After adjusting for clinicopathologic characteristics in multiple logistic regression analysis (Table 6), a higher BMI and higher BSA were not predictors for multiplicity, bilaterality, ETE, or CLNM.
Categorized by World Health Organization classification.
BRAF mutation analysis was started in 2008, and it was performed in 491 men with PTC.
Categorized by quartiles.
BRAF mutation analysis was started in 2008, and it was performed in 491 men with PTC.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), bilaterality, ETE, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, ETE, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, bilaterality, CLT, and CLNM.
Adjusted for sex, age (per 10 years), tumor size (per 0.1 cm), multiplicity, bilaterality, ETE, and CLT.
Categorized by World Health Organization classification.
Categorized by quartiles.
Association between locoregional recurrence and anthropometric parameters in women with PTC
Median follow-up in women with PTC was 52.3 months (range 6.0–147.8 months). Survival analysis was not performed because cause-specific death was reported in only a single patient. Locoregional recurrence was observed in 136 women with PTC (3.4%). Of these, 127 (93.4%) occurred in regional LNs, and the remaining nine (6.6%) in the operation bed. Regarding BMI (Fig. 1A), the recurrence-free survival (RFS) rates at 5 and 10 years were 95.7% and 92.7% in the normal group, 96.6% and 96.3% in the overweight group, and 97.7% and 97.7% in the obese group, respectively. There was no statistically significant difference in the log-rank test (p = 0.184). Regarding BSA (Fig. 1B), the RFS rates at 5 and 10 years were 95.6% and 94.8% in the BSA1 group, 96.4% and 93.4% in the BSA2 group, 95.5% and 92.6% in the BSA3 group, and 96.6% and 95.0% in the BSA4 group, respectively. There was no statistically significant difference in the log-rank test (p = 0.359).
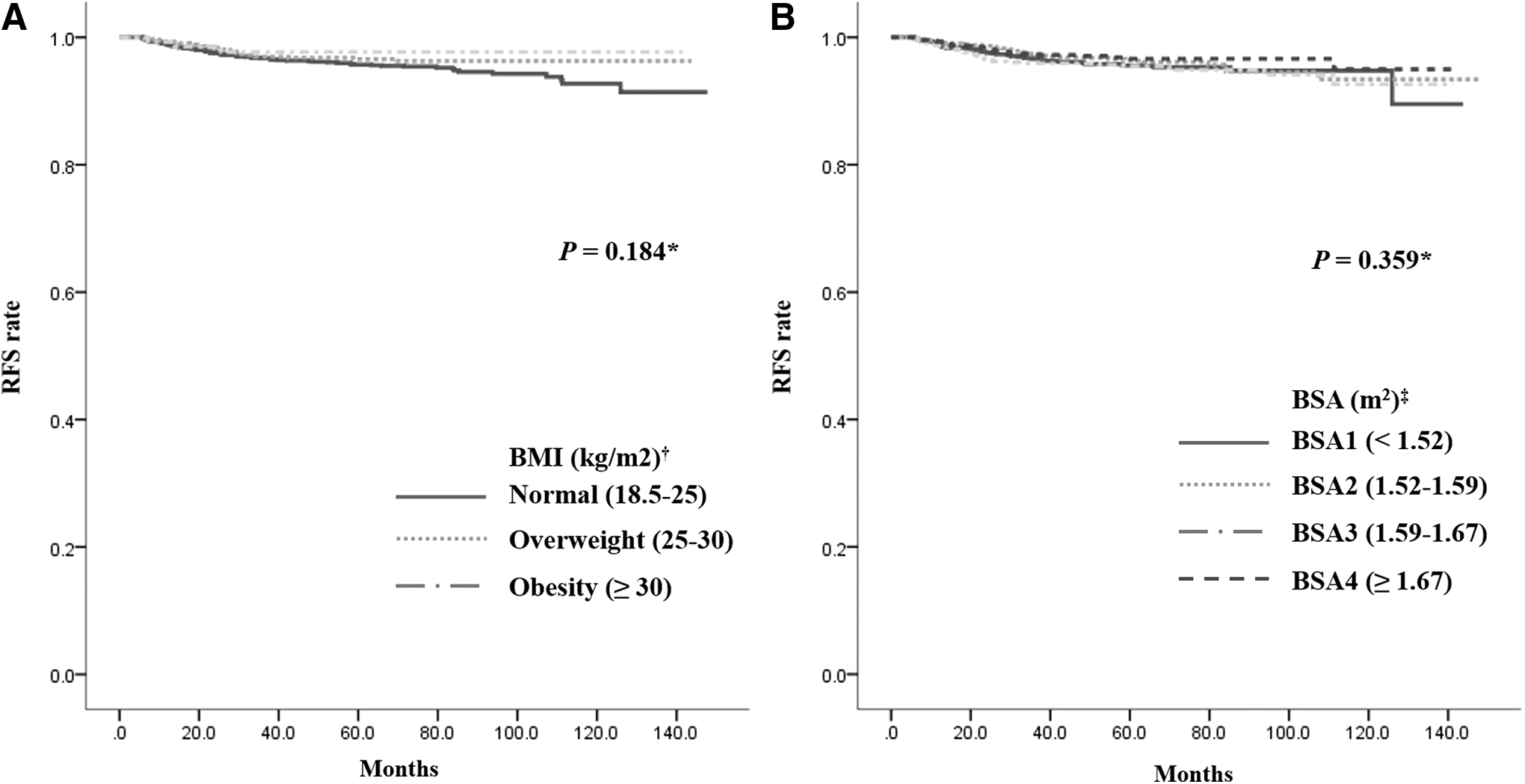
RFS according to anthropometric parameters in women with PTC.
Association between locoregional recurrence and anthropometric parameters in men with PTC
The median follow-up in men with PTC was 42.7 months (range 6.0–140.2 months). Survival analysis was not performed because cause-specific death was reported in only two patients. Locoregional recurrence was observed in 74 men with PTC (6.7%). Of these, 72 (97.3%) occurred in regional LNs, and the remaining two (2.7%) in the operation bed. Regarding BMI (Fig. 2A), the RFS rates at 5 and 10 years were 90.3% and 88.8% in the normal group, 93.9% and 91.5% in the overweight group, and 89.3% and 89.3% in the obese group, respectively. There was no statistically significant difference in the log-rank test (p = 0.184). Regarding BSA (Fig. 2B), the RFS rates at 5 and 10 years were 91.9% and 89.0% in the BSA1 group, 89.0% and 84.7% in the BSA2 group, 91.9% and 91.9% in the BSA3 group, and 94.8% and 94.8% in the BSA4 group, respectively. There was no statistically significant difference in the log-rank test (p = 0.061).
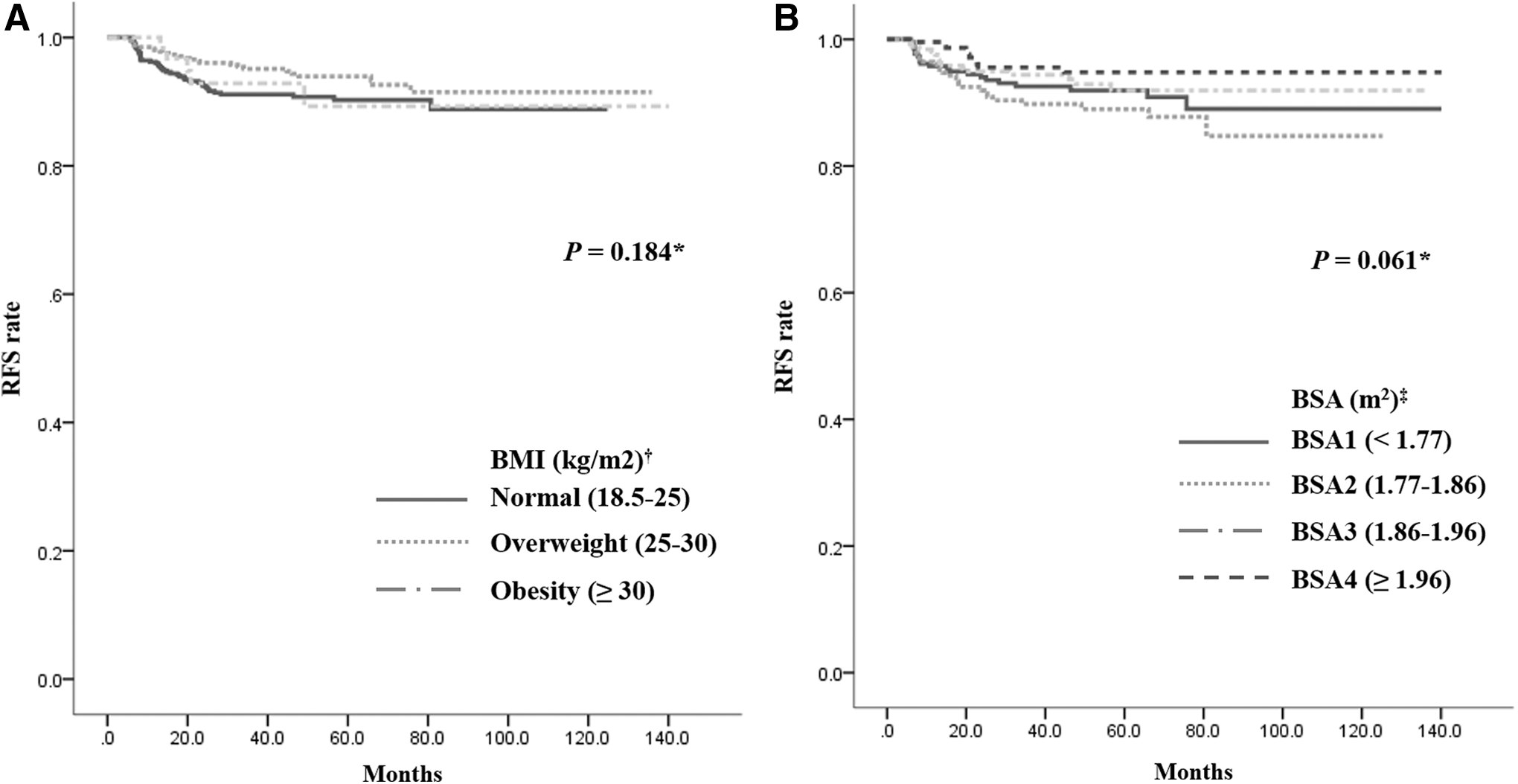
RFS according to anthropometric parameters in men with PTC.
Discussion
The association between obesity and cancer aggressiveness has several explanations. A major component of tumor stroma consists of surrounding adipocytes. Adipose tissue actively contributes to tumor growth and metastasis by functioning as an endocrine organ. Adipose tissue secretes signaling molecules and acts as an energy reservoir for embedded cancer cells (19 –21). In breast and colon carcinomas, elevated circulating insulin levels are associated with poor prognosis (22 –24). Elevated circulating leptin levels are associated with disease progression and poor prognosis in ovarian, breast, stomach, and kidney carcinomas (25 –28). In contrast, the circulating adiponectin level is negatively correlated with BMI (29). In obese patients, decreased serum adiponectin levels are associated with the progression of several malignancies (30 –33). Furthermore, hypertrophic expansion of adipose tissue may induce hypoxia, which triggers compensatory angiogenesis or makes patients resistant to chemotherapy (34 –36).
Similarly, in PTC, several hypotheses explain the association between obesity and tumor behavior. Cheng et al. demonstrated that leptin and its receptor are expressed in PTC. This expression is associated with tumor aggressiveness (37). An in vitro analysis from Uddin et al. (38) suggests that leptin stimulates cell proliferation and inhibits apoptosis via activation of the PI3K/AKT signaling pathway in PTC. However, overexpression of the leptin receptor is not an independent predictor for PTC recurrence. In addition, because physical examination is often limited in obese patients, delayed detection of PTC may explain the increased risk of tumor aggressiveness (39).
Although previous clinical studies have examined the association between obesity and PTC behavior (9 –12), the present study has unique factors. First, this is a large study with >5000 cases, limited to PTC patients who underwent total thyroidectomy and bilateral CND. Second, rigorous exclusion and inclusion criteria were used for clear and accurate analyses. Third, analyses were conducted separately for men and women because of sexual dimorphism in obesity (13,14). Finally, anthropometric parameters of BMI and BSA were assessed.
This study shows sexual dimorphism in the association between PTC behavior and anthropometric parameters. A high BMI was an independent predictor of multiplicity and ETE only in women. Higher BSA was also an independent predictor of multiplicity only in women (Table 5). In men, no significant association was seen between PTC behavior and anthropometric parameters (Table 6). These differences between men and women might first be explained by the fact that women have more body fat than men have, even when they have the same relative BMI (40). Second, women tend to store fat subcutaneously and men accumulate fat predominately in the abdominal region (13,14). Furthermore, a previous study showed that in women, lipoprotein lipase activity is higher in subcutaneous than abdominal fat; in men, lipoprotein lipase activity is higher in abdominal than subcutaneous fat (41). However, because fewer men with PTC were included in this study (3978 women vs. 1103 men), the results in men with PTC might not be statistically significant.
Although a high BMI and BSA were independent predictors of aggressive PTC behavior in female patients (Table 3), no significant difference was seen in locoregional recurrence in relation to BMI or BSA (Fig. 1). A similar result was seen in a study by Kim et al. (11), suggesting that higher BMI was significantly associated with larger tumors, ETE, and advanced PTC stage, but not with recurrence. These findings may be explained by the scarcity of adipose tissue in the thyroid gland. The amount of adipose tissue is substantially lower in the thyroid than in other organs or tissues such as the breast. Therefore, the impact of adipose tissue might be locally limited to the thyroid gland capsule, a contact area with the surrounding adipose tissue, causing the development of thyroid cancer near the capsule with a high incidence of ETE. In contrast, abundant adipose tissue within breast tissue may facilitate dissemination of breast cancer cells along the ducts.
This study focused on the association between BSA and PTC behavior. In women with PTC, a higher BMI was an independent predictor for multiplicity and ETE. However, a higher BSA was an independent predictor only of multiplicity (Table 3). BSA is less affected than BMI by abnormal adipose mass, making BSA a better indicator of metabolic mass than BMI. Therefore, BSA has been widely used as the biometric unit for normalizing physiologic parameters and determining appropriate drug doses (42 –44). Given the relatively weak relationship between BSA and PTC behavior (although a stronger relationship was seen between BMI and PTC behavior), it is hypothesized that adipose tissue mass may be involved in tumor aggressiveness. PTC is a slow-growing tumor. Therefore, the effect of adipose tissue on initiation and progression of PTC may be prolonged. To investigate this hypothesis, examining body adipose mass during childhood or adolescence, before diagnosis, will be valuable.
BRAF mutation analysis started in 2008 in the authors' institution, and it was performed in 2016 PTC patients in the present study. The overall prevalence of BRAF mutation positivity was 82.2%, and it was significantly and linearly associated with higher BMI in women with PTC (Table 1). Fernandez et al. (45) and Lee et al. (46) found a positive association between BMI and BRAF mutation positivity. Prior studies demonstrated a strong association between BRAF mutation positivity and aggressive clinicopathologic characteristics of PTC, including advanced stage, ETE, LN metastasis, and tumor recurrence (47). These results might suggest an association between PTC behavior, BRAF mutation positivity, and obesity. Further investigations are required to clarify this association.
TSH may influence the growth and differentiation of thyroid cells (48). TSH levels are higher in patients with thyroid cancer than in patients with benign nodular disease (49). Furthermore, in obese patients, TSH levels contribute to increasing PTC aggressiveness (50). However, in this study and others (12,46), TSH levels were not significantly associated with BMI or BSA, regardless of sex (Tables 1, 2, 4, and 5).
This study has several limitations. It is a nonrandomized retrospective cohort study. The patient data may be incomplete. The possibility of residual confounding variables of measured or unmeasured factors cannot be ruled out. Second, this study included PTC patients who underwent total thyroidectomy with bilateral CND. Total thyroidectomy was performed according to ATA management guidelines (15) when the primary tumor was >1 cm, and/or if multifocality, bilaterality, ETE, or abnormal lymphadenopathy was detected during preoperative or intraoperative examination. Furthermore, therapeutic CND was performed when abnormal lymphadenopathy was detected during preoperative or intraoperative examination, and prophylactic CND was performed on PTC patients with clinically uninvolved central neck LNs, in particular for advanced primary tumors (T3/T4). Therefore, case selection in this study was possibly biased toward a high-risk group. Third, higher BMI is a risk for thyroid cancer (5), and ultrasonography resolution can be diminished in obese patients by thick subcutaneous fat (51). Therefore, the occurrence and detection of PTC may differ by body size. Fourth, although BMI and BSA are most commonly used as a measurement of body mass and fat, other measurements such as waist circumference, neck circumference, waist-to-hip ratio, or skinfold thickness were not available for this study. Fifth, follow-up duration was relatively short for PTC, and cause-specific mortality was extremely low. Therefore, cause-specific mortality could not be analyzed, only locoregional recurrence. Finally, another potential limitation is the possible genetic and environmental differences between the study population and those of others. For example, two previous studies on obesity and PTC aggressiveness in Caucasian (9) and Korean (11) patients arrived at different conclusions. Therefore, the present results may not be generalizable to other patient populations. The high prevalence of the BRAF mutation in this study population (82.2%) could also be explained by geographic bias (52 –54).
In conclusion, in women with PTC, a higher BMI was an independent predictor for multiplicity and ETE. Furthermore, a higher BSA was an independent predictor for multiplicity. However, BMI and BSA were not predictors for PTC behavior in men. Further studies on the relationship between obesity and the clinicopathologic characteristics of PTC, particularly molecular markers such as BRAF mutation positivity, may provide additional information on development and management of PTC patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.