
Abstract
Background:
It is now recognized that noninvasive follicular variant of papillary thyroid carcinoma (NFVPTC) is a distinct subset of FVPTC with an exceedingly indolent clinical course. The Afirma gene-expression classifier (GEC) helps guide clinicians in the management of thyroid nodules with indeterminate fine-needle aspiration (FNA) results. Thyroid surgery is recommended for nodules with a suspicious Afirma result, whereas observation is deemed reasonable for most nodules with a benign result. The aim of this study was to confirm that the Afirma test detects NFVPTCs and to determine how many carcinomas detected by the Afirma GEC represent NFVPTCs.
Methods:
From a database of 249 FNAs sent for Afirma testing between January 2012 and October 2014, a search was conducted for cases with a preceding FNA diagnosis of atypia/follicular lesion of undetermined significance (AUS/FLUS) or suspicious for a follicular neoplasm (SFN), a suspicious Afirma result, and a corresponding resection specimen reviewed at Brigham and Women's Hospital. The diagnoses of the prior FNAs and subsequent resection specimens were recorded. Slides for all resection specimens with a diagnosis of FVPTC were reviewed to identify NFVPTCs.
Results:
Sixty-three cases met the inclusion criteria. The preceding FNA diagnosis was AUS/FLUS in 34 (54%) cases and SFN in 29 (46%) cases. The surgical resection specimen demonstrated 16 (25%) FVPTCs, five (8%) follicular thyroid carcinomas, one (2%) classical type PTC, and 41 (65%) benign tumors/nodules. Of the 16 FVPTCs, 14 (88%) were NFVPTCs. Thus, NFVPTCs accounted for 64% of the carcinomas in the cohort.
Conclusion:
These results indicate that the Afirma GEC detects NFVPTCs and that many of the carcinomas detected by Afirma are NFVPTCs. While all care should be individualized and include clinical and sonographic assessment, these results suggest lobectomy as opposed to total thyroidectomy should be considered for nodules with a preceding AUS/FLUS or SFN on cytology and a suspicious Afirma result.
Introduction
T
In the past decade, it has been shown that the follicular variant of papillary thyroid carcinoma (FVPTC) can be further subclassified based on growth pattern. FVPTCs that demonstrate infiltrative growth have a significant rate of lymph node metastases, a potential to recur, and a BRAFV600E mutation frequency of roughly 25% (7 –9). In contrast, encapsulated, partially-encapsulated, and well-circumscribed FVPTCs without capsular penetration or lymphovascular invasion (i.e., noninvasive tumors) have very little, if any, metastatic potential or recurrence risk (7 –11). Additionally, most groups have shown that the noninvasive follicular variant of papillary thyroid carcinoma (NFVPTC) harbors RAS and PAX8/PPARγ mutations but lacks the BRAFV600E mutation that is often associated with high-risk histopathologic features (8,12 –14). The indolent nature of NFVPTCs, along with a molecular profile that is more in keeping with follicular adenomas and follicular thyroid carcinomas (FTCs; i.e., tumors in which invasive growth is a requisite for malignancy), prompted endocrine pathologists to question whether NFVPTCs warrant a designation of carcinoma.
At the 2015 United States and Canadian Academy of Pathology (USCAP) meeting, it was proposed that NFVPTCs should no longer be termed carcinoma. Conservative management (i.e., lobectomy only) was advised for these tumors. Lobectomy is warranted for two main reasons. First, NFVPTC may be a precursor to a more aggressive thyroid tumor. Second, histologic evaluation of the tumor is required to assess for infiltrative or invasive growth, which cannot be discerned by cytologic review of the FNA. Tumors with any area of infiltrative growth would be designated as an infiltrative FVPTC—a diagnosis, as noted above, that is associated with frequent lymph node metastases and a risk of recurrence. Tumors with either capsular penetration or lymphovascular invasion would be designated as an encapsulated FVPTC with invasion. Approximately one third of encapsulated FVPTC are invasive (7 –9,11,15). Encapsulated FVPTCs with invasion metastasize in a manner similar to FTC with distant metastases as opposed to lymph node metastases (8,15,16). Although rare, these patients can die of their disease (8,15). Hence, it is important that the tumors be resected and evaluated histologically.
The validation of the GEC did not assess the identification of FVPTC subtypes, since the concept of NFVPTC and infiltrative FVPTC was still developing. The aim of this study was to evaluate if the Afirma test detects NFVPTCs and to determine how many carcinomas detected by the Afirma GEC would be categorized as NFVPTCs.
Materials and Methods
Study population and data acquisition
Approval from the Brigham and Women's Hospital (BWH) investigation review board was obtained. From a database of 249 FNAs sent for Afirma GEC testing between January 2012 and October 2014, nodules were retrospectively identified that were ≥1 cm on imaging, had a suspicious Afirma result, an AUS/FLUS or SFN diagnosis on FNA, and a corresponding resection specimen reviewed at BWH. One hundred eighty-six FNAs sent for testing did not meet the inclusion criteria for the following reasons: 136 cases had a benign Afirma result, 16 cases had insufficient RNA for Afirma testing, 11 cases had prior FNA diagnoses other than AUS/FLUS or SFN, in 22 cases surgery was not performed at BWH, and in one case the nodule tested was <1 cm on ultrasound (FNA was performed due to the clinical history). For each case that met the inclusion criteria, the cytology and surgical pathology reports were reviewed, and the diagnoses of the prior FNAs and subsequent resection specimens were recorded. Additionally noted were demographic and clinical information (age, sex, sonographic size, location of the thyroid nodule sent for Afirma testing, presence of multiple nodules, presence of hypothyroidism, and type of surgery performed) and histopathologic characteristics (size, margin status, presence of lymphovascular invasion or extrathyroidal extension, and lymph node status).
All FNAs sent for Afirma testing were performed at BWH. FNAs were performed using a 25-gauge needle by an endocrinologist under ultrasound guidance (typically three or four passes). The specimen was collected immediately in CytoLyt (Hologic, Marlborough, MA), and a single Papanicolaou-stained ThinPrep slide was prepared using the ThinPrep 2000 (Hologic). The FNA diagnoses were recorded from the pathology reports generated by staff cytopathologists using the Bethesda System for Reporting of Thyroid Cytopathology (17). If multiple FNAs were performed on the same nodule, the FNA diagnosis associated with the highest risk of malignancy was used in the categorization of the case (17). At the time of the FNA, two additional samples were obtained for Afirma genomic analysis and shipped frozen. Description of the microarray assay and an annotation of genes used by the classifier are detailed in prior reports (5,18).
All tumor slides for cases diagnosed as FVPTC on resection were reviewed by K.W. and J.A.B. to identify tumors that would be categorized as NFVPTCs. Tumors diagnosed as FVPTC had an entirely or nearly entirely follicular architecture (<1% papillae) and nuclear features of PTC. NFVPTCs included encapsulated tumors that had a complete fibrous capsule separating the tumor from the surrounding benign parenchyma and partially-encapsulated/well-circumscribed tumors that had a partial capsule or entirely lacked a capsule yet had a sharp interface between the tumor and benign parenchyma. Tumors with any indication of an infiltrative edge were categorized as infiltrative FVPTC, and those with capsular penetration or lymphovascular invasion were categorized as encapsulated FVPTC with invasion. An example of an NFVPTC is shown in Figure 1.
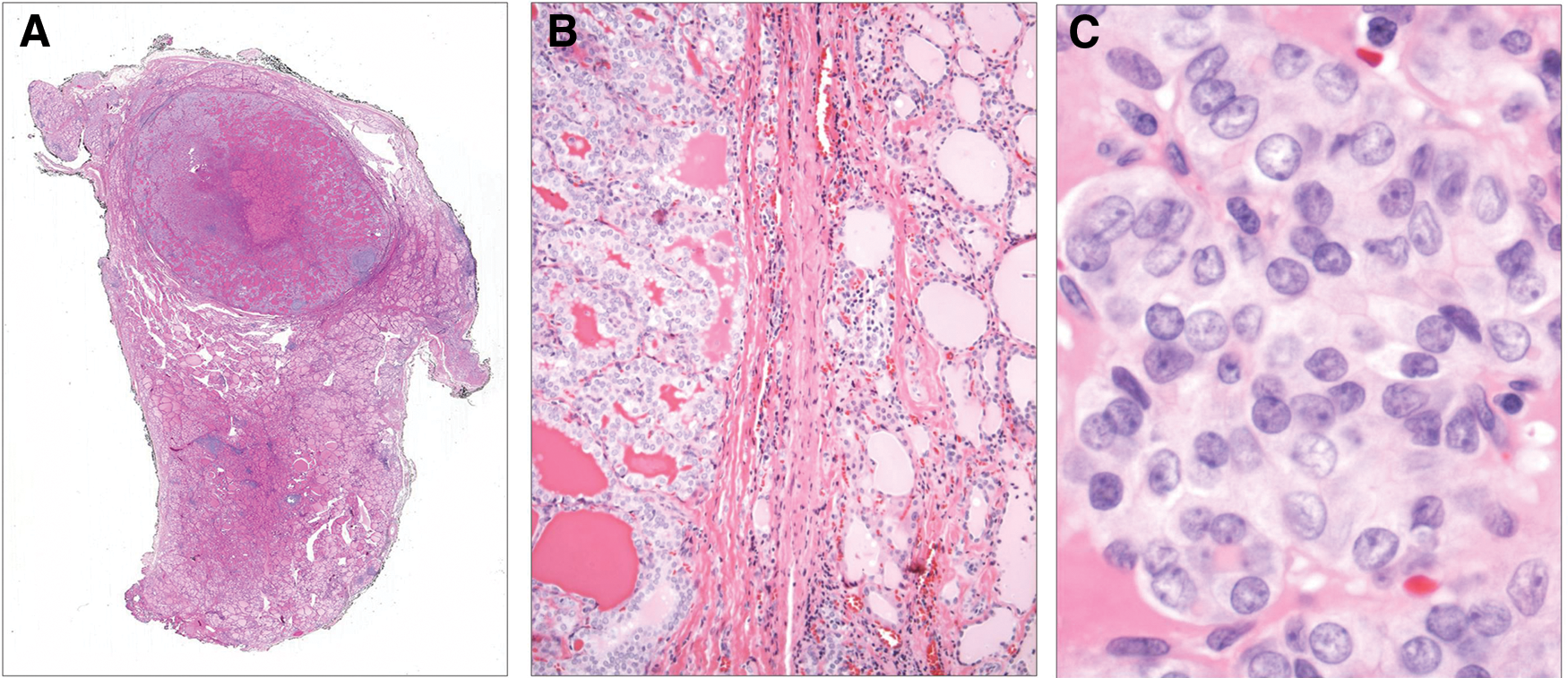
Architectural and cytologic features of noninvasive follicular variant of papillary thyroid carcinoma (NFVPTC). (
One case that was initially diagnosed as a follicular tumor of uncertain malignant potential was also re-reviewed. It was an oncocytic follicular neoplasm with significant capsular irregularity, but no definitive complete capsular penetration. Based on this re-review, this case was categorized as benign.
Results
A total of 63 cases met the inclusion criteria (a nodule of ≥1 cm on imaging with an AUS/FLUS or SFN cytology, a suspicious Afirma GEC result, and a subsequent surgical resection reviewed at BWH). The nodules were from 61 patients of whom 48 (79%) were women and 13 (21%) men with a mean age of 53 years at the time of resection (range 22–79 years). The FNA diagnosis was AUS in 34 (54%) cases and SFN in 29 (46%). Thirty-two (53%) patients underwent initial lobectomy/hemi-thyroidectomy, while the remaining 29 (48%) underwent initial total or near-total thyroidectomy. In the majority of cases in which an upfront total thyroidectomy was performed, the decision to pursue a total thyroidectomy as the initial surgical resection was based on multiple factors. These included the presence of bilateral nodules, a desire to avoid a second surgery should malignancy be found in the hemi-thyroidectomy specimen, and a diagnosis of hypothyroidism already requiring hormone supplementation.
Twenty-two (35%) of the nodules were malignant on surgical resection, and 41 (65%) were benign tumors/nodules. Of the malignant cases, 16 (73%) were FVPTC, five (23%) were FTC, and one (5%) was a classical type PTC. On pathologic examination, the mean size of malignant tumors was 1.9 cm (range 0.8–5.0 cm). The two tumors that were <1 cm in size appeared >1 cm on ultrasound but were smaller on pathologic examination. Two (9%) of the carcinomas had associated lymphovascular invasion (FTCs), and one (5%) had extrathyroidal extension (an FTC). The resection margins were negative in all cases. Lymph nodes were sampled in eight (36%) of the malignant cases; none demonstrated nodal metastasis. Of the 16 FVPTCs, 14 (88%) were classified as NFVPTCs. Thus, overall, NFVPTCs accounted for 64% of the carcinomas in the cohort. The mean size of NFVPTCs was 1.7 cm (range 0.8–2.7 cm). The preceding FNA diagnosis for NFVPTCs was AUS in 12 (86%) cases and SFN in two (14%) cases.
Discussion
The Afirma GEC was developed to risk stratify nodules with indeterminate cytology in order to reduce the number of diagnostic surgeries performed (5). The aim of this study was to confirm that the GEC detects NFVPTCs and to determine how many carcinomas detected by the GEC represent NFVPTCs.
The cohort included 63 cases with a preceding FNA diagnosis of AUS/FLUS or SFN and a suspicious Afirma result. The surgical resection specimen demonstrated 16 (25%) FVPTCs, five (8%) FTCs, one (2%) classical type PTC, and 41 (65%) benign tumors/nodules. Of the 16 FVPTCs, 14 (88%) were NFVPTCs. While the study demonstrates that the GEC recognizes NFVPTCs as suspicious, it is unable to show with certainty that all NFVPTCs are categorized as suspicious by the GEC, since tumors with an AUS/FLUS or SFN diagnosis on FNA and a benign Afirma were not resected. However, in the initial Afirma validation study, all NFVPTCs would have been characterized as carcinoma (5). Therefore, the sensitivity ascribed to the GEC in the initial validation study should still be valid with respect to NFVPTCs.
NFVPTCs accounted for 64% of the carcinomas in the cohort. In the initial Afirma validation study, 22% of the malignancies identified by the GEC were FVPTCs (5). This apparently disparate result may be explained in part by the fact that the initial validation study included nodules with a preceding FNA diagnosis of SUS. Classical type PTCs have more developed nuclear features of PTC compared with FVPTCs. Thus, more classical type PTCs are present in the SUS category than in the AUS/FLUS or SFN categories (19 –23). Our findings are consistent with those reported by Lastra et al. who found that of the malignant tumors resected at their institution with a suspicious Afirma result and a preceding AUS/FLUS or SFN diagnosis, 73% were FVPTCs (the FVPTCs were not further subclassified in this study), 14% were classical PTCs, and 14% were FTCs (24). Moreover, the finding that many of the carcinomas detected by the GEC are NFVPTCs is a direct reflection of the fact that the Bethesda categorization of a nodule is associated with tumor type, stage, and prognosis (22,25). In other words, carcinomas resected in the setting of an AUS/FLUS or SFN FNA diagnosis are usually FVPTCs without associated extrathyroidal extension or lymph node metastases (22,25). Specifically, Vanderlaan et al. found that FVPTCs accounted for 85% and 73% of the PTCs associated with an AUS/FLUS and SFN FNA diagnosis, respectively (22), and Liu et al. showed AUS, SUS, and malignant FNA diagnoses were progressively associated with an increasing risk of extrathyroidal extension (p < 0.001) and local lymph node metastases (p < 0.001) (25). Thus, it is not surprising that most of the carcinomas resected on the basis of a suspicious Afirma result are indolent FVPTCs, since Afirma testing is being performed on nodules associated with an AUS/FLUS or SFN diagnosis on FNA. For this same reason, many of the carcinomas resected in the setting of a preceding indeterminate FNA and a mutation detected by Thyroseq are RAS mutation-positive FVPTCs (26,27).
The extent of initial surgery that should be performed for a nodule with an AUS/FLUS or SFN cytologic diagnosis and a suspicious Afirma result has not been established. In a recent publication by the American Thyroid Association (ATA) on the application of molecular profiling of thyroid nodules on perioperative decision making, the authors state that a nodule with a suspicious GEC result along with either an AUS/FLUS or SFN diagnosis on FNA should be managed by at least a diagnostic lobectomy (6). Additionally, they indicate that the extent of initial surgery should be based on a thorough discussion with the patient, endocrinologist, and surgeon that takes into account all clinical characteristics specific to that patient. Although, clinical and ultrasonographic characteristics still need to be factored into the decision regarding extent of surgery, the present findings suggest that a lobectomy should be considered for most nodules with an AUS/FLUS or SFN diagnosis and a suspicious Afirma result. Interestingly, nearly half of the patients in our study underwent an initial total or near-total thyroidectomy. While some of these patients had other clinical and ultrasonographic findings that influenced that decision, the results suggest that heightened recognition of the indolent nature of many of the carcinomas resected in the setting of an AUS/FLUS or SFN FNA diagnosis and a suspicious Afirma result may significantly alter decision making regarding the extent of initial surgery. It is also worth noting that a more conservative management of low-risk thyroid carcinomas is in line with the new ATA management guidelines for adult patients with differentiated thyroid carcinoma (1). Finally, a shift in terminology for NFVPTC away from carcinoma would result in a decrease in the positive predictive value of the GEC. In other words, with a shift in terminology, there would be a decrease in the number of nodules resected with a preceding suspicious Afirma result that are subsequently designated as “carcinoma” on resection. However, because resection is the appropriate management for these tumors, binary endpoints in the context of NFVPTC have limitations, and it is appropriate that the GEC categorizes these tumors as suspicious, regardless of terminology.
In summary, the Afirma GEC detects NFVPTCs, and many of the carcinomas detected by Afirma are NFVPTCs. While all care should be individualized and include clinical and sonographic assessment, these results suggest lobectomy as opposed to total thyroidectomy should be considered for nodules with a preceding AUS/FLUS or SFN on cytology and a suspicious Afirma result.
Footnotes
Author Disclosure Statement
Dr. Erik Alexander is a consultant for Veracyte.