
Abstract
Background:
Whether the addition of immunosuppressive drugs to standard antithyroid drugs reduces the relapse risk in Graves' disease remains uncertain.
Purpose:
The aim of this study was to investigate the effects of immunosuppressive drugs on the relapse rate after a first episode of hyperthyroidism due to Graves' disease.
Methods:
Based on a pre-specified protocol, PubMed (1946–July 2015), EMBASE (1947–July 2015), and Cochrane (1992–July 2015) databases were searched. The search was for (randomized) controlled trials comparing immunosuppressive drugs with a control group. PRISMA and SIGN statements were used for assessing data quality. Two reviewers extracted data, with any disagreement being resolved by consensus. Data were pooled using a random-effects model.
Results:
The primary endpoint was relapse of disease until follow-up. Secondary endpoints included reduction of thyroid volume and decrease in thyrotropin-receptor antibody (TRAb) levels. Seven trials with 862 participants were included. Most trials were small with a moderate to high risk of bias. There were 113 relapses in 481 (23.5%) patients receiving immunosuppressive drugs compared with 225 relapses in 381 (59.1%) control patients (risk ratio for recurrence 0.55; [confidence interval (CI) 0.41–0.75]). Subgroup analyses showed similar effects for randomized trials and controlled trials (I 2 0%), and for trials using corticosteroid and non-corticosteroid immunosuppressive drugs (I 2 0%). Use of immunosuppressive drugs also resulted in significant reductions in thyroid volume (−10.72 mL [CI −15.59 to −5.85]) and TRAb levels (−17.01 IU/L [CI −33.31 to −0.72]). Immunosuppressive drug-related adverse effects were not systematically reported, and thus were not included in the quantitative analysis.
Conclusions:
Current evidence suggests a possible relevant reduction in relapse risk when immunosuppressive drugs are added to standard treatment of Graves' disease. The small number of trials with high heterogeneity in regard to treatment modalities and the lack of systematic reporting of adverse effects calls for larger, conclusive trials.
Introduction
G
Standard treatment for Graves' disease includes use of antithyroid drugs (ATD) for a total duration of 12–18 months to treat the overproduction of thyroid hormones. In addition, ATD may also have immuno-modulating effects and thus a positive impact on the course of Graves' disease (4). This approach is generally well accepted by patients and physicians, as it offers the possibility of disease resolution without the need for livelong substitution with thyroid hormone (5). Yet, the risk of relapse is high (around 50%), and patients may suffer from medication side effects, especially if treated with higher doses, such as exanthema, pruritus, urticaria, hepatitis, and agranulocytosis. Due to the high risk of relapse, an alternative first-line treatment used mostly in the United States is radioactive iodine (RAI) ablation, a definitive treatment that typically results in hypothyroidism (3,6).
Because of the autoimmune nature of Graves' disease, additional use of immunosuppressive drugs in combination with ATD has been suggested to impact the clinical outcomes positively. Yet, whether the addition of immunosuppressive drugs to standard ATD treatment reduces the risk of relapse in Graves' disease is not well understood. Herein, a systematic review and meta-analysis was performed to study the effects of immunosuppressive drugs in addition to standard treatment compared to standard treatment alone on relapse rates and treatment effects of patients with hyperthyroidism due to Graves' disease.
Methods
Objectives
The objective of this systematic review and meta-analysis was to study the effects of immunosuppressive drugs compared to standard treatment on clinical outcomes in patients with hyperthyroidism due to Graves' disease.
Protocol and eligibility criteria
This review adheres to PRISMA guidelines (7). First, a review protocol was generated (see Supplementary Appendix; Supplementary Data are available online at
Observational studies and trials with a follow-up of <12 months, as well as case reports, reviews, and trials not reporting relapse, our primary endpoint of interest, were excluded.
Outcomes
The primary outcome was the rate of relapse (recurrence of hyperthyroidism) within a follow-up of at least 12 months after cessation of treatment. Secondary outcomes were serum levels of TRAb reduction after initiation of treatment, changes in thyroid volume, and adverse effects of treatment. Timing of outcome measurement was at least one year after withdrawal of ATDs.
Search strategy and study selection
The electronic databases PubMed/Medline, EMBASE, and the Cochrane CENTRAL Library were searched (all until end of July 2015). The references of leading articles were also hand-searched to identify further articles.
The search strategy included following terms: Graves' disease, steroids, immunosuppression, goiter, hyperthyroidism, and Basedow (see Supplementary Appendix for further details). The articles found were transferred into EndNote Version X7 (Thomson Reuters, Philadelphia, PA) and then screened by title and abstract. Full articles were retrieved for further assessment if the information given indicated that the study included patients receiving immunosuppressive treatment for Graves' disease, had a control group (receiving standard therapy), and had well-defined criteria for the diagnosis of Graves' disease and relapse. If there was any doubt about the relevance of the article from the information given in the title and abstract, the full article was consulted for clarification. All articles were reviewed by two independent authors (L.G. and T.S.). In case of disagreements, a solution was obtained by consensus and, if no agreement was reached, by a third reviewer (P.S.; see Fig. 1).
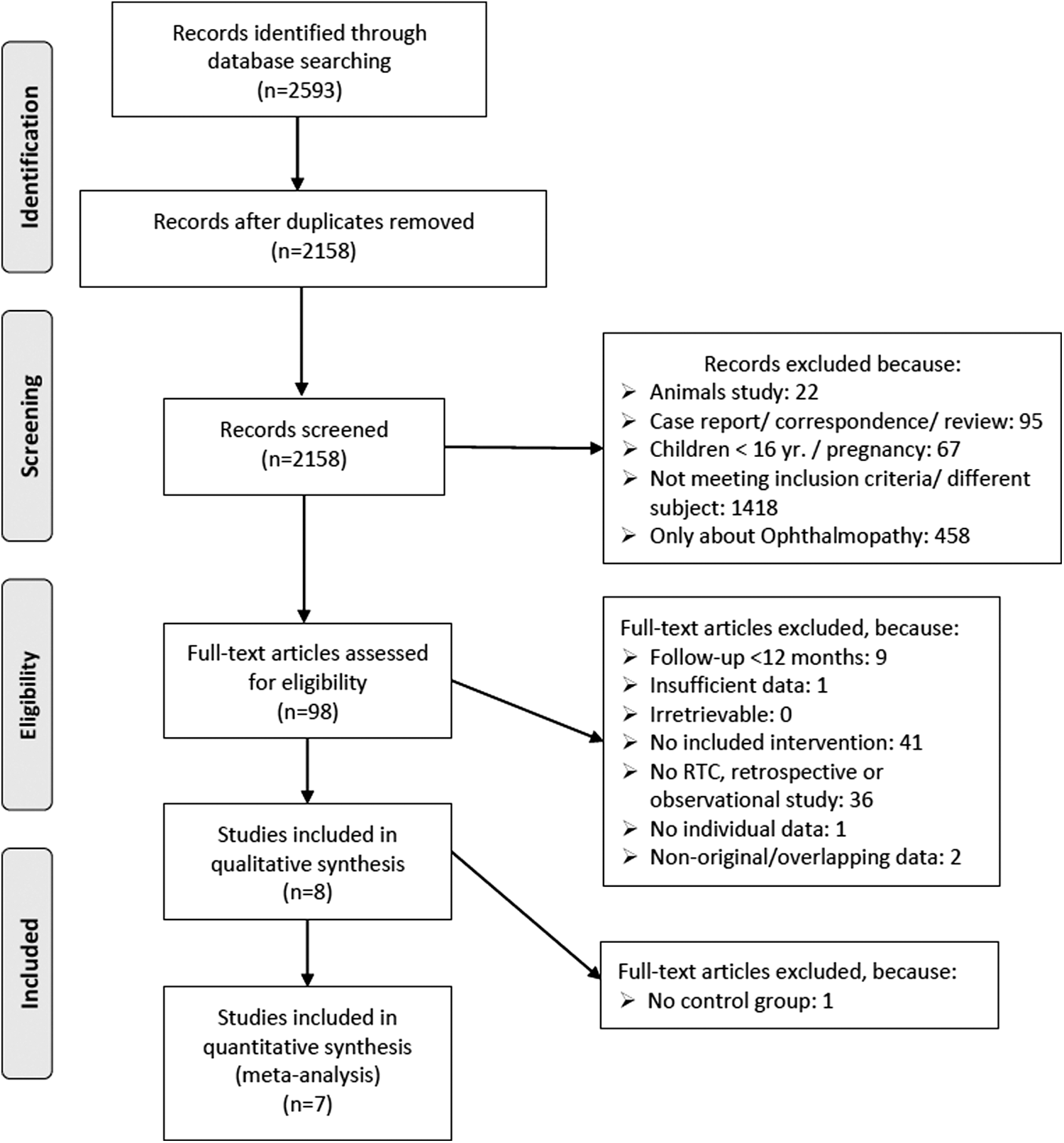
Study flow diagram.
Data collection
For all included studies, a data extraction table was generated based upon the Cochrane Handbook for Systematic Reviews of Interventions (8). It was tested on two pilot studies and refined afterwards. Data were extracted by one author (L.G.) and cross-checked by another researcher (T.S.). Two review authors independently assessed trial quality (L.G. and T.S.). In case of disagreements, a solution was again obtained by consensus and, if no agreement was reached, by a third reviewer (P.S.). Duplicate publications were suspected if the same authors published multiple studies on the same subject within two years. Two trial authors (D. El Fassi (9–11) and K.A. Heemstra (12)) were contacted for a suspected double publication of data and for missing data, respectively. Because final answers had not been received by the end of October 2015, the trial data were used only once.
Data items
From all included trials, the following data were extracted: (i) general information—first author, year of publication, country; (ii) trial characteristics—design, if eligibility criteria are reported, duration, mode of randomization, blinding (assessors, patients), intention to treat analysis; (iii) interventions—basis intervention with ATD (days and dose), comparison with immunosuppressive treatment (mode of application, duration, dose, sort of immunosuppression); (iv) patients—number of patients included, sex, age; and (v) outcomes—primary outcome, secondary outcome, effect size.
Risk assessment of bias in individual studies
All included studies were assessed by two reviewers according to the Scottish Intercollegiate Guidelines Network (SIGN; see Supplementary Appendix) (13). Assessment was done by using the appropriate checklist accordingly, and the risk of bias was judged to be “unacceptable,” “high,” or “low.” The following aspects of internal and external validity were assessed and reported: (i) whether any eligibility criteria were reported; (ii) mode of randomization (e.g., random number permutation table); (iii) participants blinding; (iv) assessor blinding; (v) intention to treat analysis; (vi) outcome well defined and complete; (vii) mean follow-up in months; and (viii) percentage of lost to follow-up.
Summary measures, planned methods of analysis, and risk of bias across studies
For dichotomous data, risks ratios with confidence intervals (CI) were calculated by a fixed- (14) and a random-effects model (15). For continuous data, the raw mean difference was computed as effect size, as all measurements used the same scale. The missing standard deviations were imputed as suggested (16). An analysis of side effects was not possible, as data were not systematically reported.
As a test of heterogeneity, the variation in risk ratio (RR) across studies attributable to heterogeneity (I 2) was computed (17). As there was significant heterogeneity across studies (I 2 > 75%), data of the fixed-effect model was omitted due to overestimation of effect size.
For each trial, the effect was plotted by the inverse of its standard error (18). The symmetry of these “funnel plots” were assessed both visually and statistically with Egger's test to see if the effect decreased with increasing sample size.
The statistical analysis was conducted using RevMan software v5.3 (Cochrane Collaboration) and in part with Stata software v12.1 (Stata Corp., College Station, TX). All significance tests were two-sided, and p-value of <0.05 was considered to be statistically significant.
Results
Study selection and study characteristics
A total of 2593 articles published in seven languages were evaluated by members of the study group with appropriate skills (see Fig. 1), according to suggestions of the PRISMA group (7). Of these, 97 full-text articles were assessed for eligibility and seven trials were included in the final data analysis (9,19,20 –24). There were three randomized controlled and four controlled trials, with a total of 862 participants for quantitative meta-analysis (see Supplementary Appendix Tables 1 and 2). One trial was only evaluated qualitatively, as there was no control group (12). Trials were published between 1988 and 2012. Four studies used corticosteroids as the main immunosuppressive agent, two used rituximab, and one used azathioprine. One used a combination of dexamethasone, cyclophosphamide, and octreotide. As there was no systematic reporting, adverse effects were only assessed qualitatively (see Supplementary Appendix Table 2). They included leucopenia, rash, minor infections, chills, and fever during infusion of rituximab. There were no reports of serious adverse effects.
Risk of bias within studies
Trials were mostly small with a moderate to high risk of bias (see Supplementary Appendix Table 3). There was no blinding of participants in any of the trials, and no trial was judged as “low risk of bias.” As there were not enough high-quality studies, studies with a higher risk of bias had to be included.
Results of individual studies and synthesis of results
There were 113 relapses in 481 patients receiving immunosuppressive drugs compared with 225 relapses in 381 patients (RR 0.55 [CI 0.41–0.75]). Results were similar in the subgroup of trials using corticosteroids alone (RR 0.58 [CI 0.40–0.83]) and trials using other immunosuppressants (RR 0.42 [CI 0.15–1.17], I 2 = 0%, see Fig. 2). There were also similar effects in randomized trials compared to controlled trials (RR 0.49 [CI 0.38–0.62] vs. RR 0.62 [CI 0.31–1.2]; see Table 1). In regard to secondary endpoints, two trials (19,22) were found that reported thyroid volume and TRAb levels. The pooled analysis showed a significant reduction of thyroid volume (−10.72 mL [CI −15.59 to −5.85]) and TRAb levels (−17.01 IU/L [CI −33.31 to −0.72]) in patients receiving immunosuppressive therapies compared with controls (see Supplementary Appendix Table 1 and Figures).
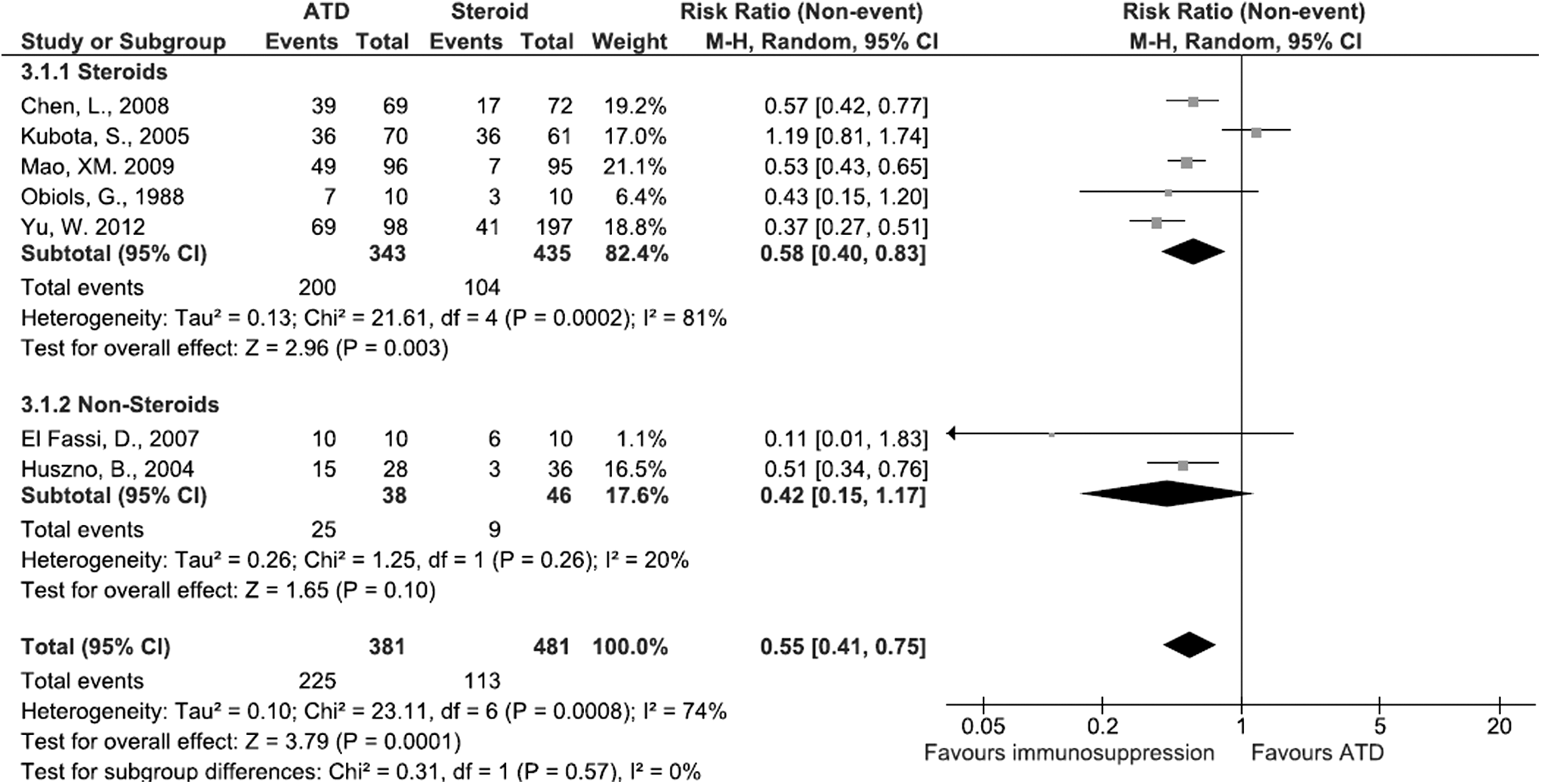
Forest plot comparing additional immunosuppressive therapy with standard treatment with antithyroid drugs alone in steroids and non-steroids.
In Mao (2009) (23), 87.4% of the ATD group (96 patients) and 89.5% of the intervention group (95 patients) had positive TRAb (206 patients enrolled; 191 included into the analysis). In Yu (2012) (20), only mean and standard deviation of TRAb titers were reported for the intervention and control group accordingly.
CI, confidence interval; TRAb, thyrotropin-receptor antibody.
Risk of bias across studies
As there was strong evidence for heterogeneity (I 2 = 74%, p < 0.001) for the primary outcome, a funnel plot was computed (see Supplementary Appendix Fig. 3) showing slight asymmetry. Egger's test for publication bias did also indicate possible publication bias across studies (−0.93 [CI −7.28 to 5.42], p = 0.72). This may be explained by small study effects, poor design of the included studies, and true heterogeneity considering the genetic differences in the studied populations (18).
Discussion
Summary of evidence
This is the first systematic review and meta-analysis focusing on the use of immunosuppressive therapy when used in addition to standard treatment for reducing the risk of relapse in patients with hyperthyroidism due to Graves' disease. The study was able to include a total of seven trials. However, all of them had small patient numbers and overall moderate to low trial quality and risk of bias. The pooled analysis showed a strong reduction of relapse risk, which was similar in trials using corticosteroid drugs and other non-corticosteroid immunosuppressive drugs, as well as in randomized trials and controlled trials. In addition, the type of trials (i.e., randomized trials vs. controlled trials) did not have an influence on effects. An overall relapse rate of 59% was observed in the control group. A recent literature review by Franklyn and Boelaert reported a relapse rate of 50–80% (4), and a large systematic review by a Cochrane group found an average relapse rate of 51–68% depending on treatment regimen (6).
When looking at the two trials reporting thyroid volume and TRAb levels after treatment initiation, beneficial effects were found in the pooled analysis. Based on these studies, the reduction in thyroid volume and TRAb levels is clinically relevant, as it has been shown that goiter size and antibody levels at the time of ATD withdrawal are predictors of risk of relapse (25).
Despite the strong reduction in relapse risk found in this analysis, there remain important unanswered questions regarding safety (adverse effects), efficacy, optimal timing and duration, as well as type of immunosuppressive therapy. Some studies used interventional application forms (i.e., intrathyroidal injections), which can cause bleeding, local infections, and perforation of cervical structures (e.g., nerves, trachea, carotid artery) (26). None of the studies found by the systematic review systematically reported safety issues and drug side effects. Therefore, the emphasis of future trials should be put on adverse effects to clarify not only the benefits but also the potential harm associated with these different immunosuppressive drugs.
Interestingly, there was no difference observed in regard to the immunosuppressive agent that was being used in the trials, nor in regard to the route of application. This may be explained by the small number of trials and included patients. Still, corticosteroids represent a standard treatment for different autoimmune and inflammatory diseases, but side effects of steroid exposure, including bone health and metabolic disturbances, are important. From a physiopathological perspective, the application of rituximab is appealing. As Graves' disease is thought to be a prototypic type II autoimmunity reaction (2), the use of rituximab provides a targeted therapy and is based on a plausible pathophysiological rationale. A potential drawback is the missing effect on mature plasma cells producing TRAb (3). Additionally, a change of treatment policy could prevent a substantial amount of Graves' ophthalmopathy, as roughly 25% of patients develop their illness simultaneously with hyperthyroidism and 20–30% are not responsive to corticosteroid therapy (27,28). Its effectiveness in this field has already been systematically reviewed elsewhere (27), without, however, giving conclusive recommendations due to the scarcity of studies.
Strengths and limitations
The strengths of this study are the predefined study protocol adhering to PRISMA guidelines for systematic reviews, the inclusion of studies from all around the globe without language restrictions and thus reflecting different ethnicities and genetic backgrounds (2), and the relevance of this topic in everyday practice. As one might argue that the response to immunosuppressive drugs depends on genetic background, the robust findings of the included trials from different countries without evidence for subgroup effects suggest otherwise and increase the clinical applicability and external validity. Additionally, although there have already been various systematic reviews assessing different treatment options for Graves' disease (1,5,6,29), there is no previous systematic review on the benefits of immunosuppressive drugs on relapse risk.
The study does have several limitations. First, trials were mostly small, monocentric, and with a moderate to high risk of bias (four medium, three low quality). Only three of seven included studies were randomized, and the others were controlled trials. Second, the overall number of included trials was small, and the number of enrolled patients was low, thus reducing the precision of the calculations. In addition, none of the included studies had blinding of participants or assessors (placebo-controlled). An intention to treat analysis was performed in only three trials, and adverse effects were not systematically reported. Still, studies reported eligibility criteria, and mean follow-up was at least one year after withdrawal of ATD, mainly 24 months. It is known that most relapses occur within the first two years (1).
For secondary outcomes, there were few trials reporting data on TRAb levels and thyroid volume. In addition, adverse outcomes were not reported systematically. This is an important shortcoming, as adverse effects of immunosuppressive therapy could outweigh the potential benefits. Corticosteroids are associated with higher rates of infection and other metabolic side effects such as osteoporosis, diabetes mellitus, impaired hypothalamic–adrenal axis, and muscle wasting. In a recent literature review, it was noted that >50% of patients may experience lipodystrophy after only three months of steroid exposure with a dose-dependent increase in risk. In addition, 5–15% of patients may develop diabetes mellitus within the first three years of treatment. Alterations of lipids also occur (30). The mean risk of hypertension seems to be increased by a risk ratio of 2.2 (31). Furthermore, there is an increase in risk of heart failure, myocardial infarction, atrial fibrillation, and stroke (30,32 –34).
Use of rituximab in Graves' orbitopathy is emerging, and adverse effects are known from these studies, as well as from its use in other autoimmune diseases and cancer. Adverse effects range from fever/chills upon infusion up to lethal anaphylaxis (28,35) and progressive multifocal leukoencephalopathy. Severe infections have also been observed (28). Additionally, it has substantial costs, and cost-effectiveness data are currently lacking for patients with Graves' orbitopathy.
Conclusions
In conclusion, this systematic review and meta-analysis suggests that there may be a significant reduction in relapse risk when immunosuppressive drugs were added to standard treatment of Graves' disease. This effect was independent of type of immunosuppressive drug used and type of trial. There were also additional beneficial effects on thyroid volume and TRAb associated with the interventional drugs used. Yet, the small number of trials with high heterogeneity in regard to type of drugs used and with mostly moderate to low quality calls for a large-scale randomized controlled trial to provide more definitive conclusions.
Footnotes
Acknowledgments
The authors want to express their gratitude to Mrs. Yu Lu Li, MD, for her translation of Chinese articles. This study was supported in part by the Swiss National Science Foundation (SNSF Professorship, PP00P3_150531/1) and the Research Council of the Kantonsspital Aarau (1410.000.044). Funders had no role in the design, analysis, or writing of this article.
Author Disclosure Statement
All authors declare no conflicts of interest.