
Abstract
Background:
The aim of this study was to evaluate the effectiveness of sunitinib in patients with progressive radioiodine refractory (RAIR) thyroid cancer (TC).
Materials and Methods:
A multicentric retrospective analysis was performed of patients treated in six TUmeurs THYroïdiennes REFractaires participating centers. All patients with progressive RAIR TC who were treated with sunitinib outside a clinical trial between August 2007 and March 2015 were retrospectively and consecutively included. The primary endpoint was the overall response rate (ORR) and disease control rate ≥6 months based on RECIST criteria. Secondary endpoints included evaluation of overall survival (OS) and progression-free survival (PFS) from the first dose of sunitinib. Primary and secondary endpoints were also evaluated according to treatment setting: first or second line of tyrosine kinase inhibitor (TKI).
Results:
Fifty-seven patients (29 men; 50.8%), mean age 62.2 years (range 43–80 years) with progressive RAIR TC were included. Sunitinib was the first-line TKI treatment for 32 (56.1%) patients and the second-line TKI treatment for 25 (43.9%) patients. For all patients, according to RECIST criteria, ORR was 35.1% (20 patients) and disease control rate ≥6 months was 68.4% (39 patients). No complete response was observed. Six (10.5%) patients showed disease progression. When sunitinib was used as first-line TKI therapy, ORR was 46.9% (15/32 patients), and disease control rate ≥6 months was 75% (24/32 patients). When sunitinib was used as second-line TKI therapy, ORR was 20% (5/25 patients), and disease control rate ≥6 months was 60% (15/25 patients). The median OS and PFS were 21.0 (range 15–29) and 10.2 months (range 6–13), respectively, for all patients. With sunitinib as first-line TKI-therapy, median OS and PFS was 30.0 (range 19.0–53.0) and 15 (range 7.0–21.0) months, respectively. As second-line therapy, median OS and PFS were 13 (range 8.0–20.0) and 6 (range 5.0–11.0) months, respectively. Eleven (19.3%) patients experienced grade 3 toxicity, and four patients (7.0%) experienced grade 4 toxicity.
Conclusion:
The efficacy of sunitinib as first- and second-line TKI therapy in a large cohort of patients treated for progressive RAIR TC is herein reported. Further prospective studies are needed to evaluate the effectiveness of sunitinib in RAIR TC.
Introduction
D
Sunitinib is an oral, multi-targeted TKI with antitumor and antiangiogenic activities. It has been identified as a potent inhibitor of c-Kit, VEGF receptors, VEGFR-1, VEGFR-2, PDGFR, RET, FLT-3, and CSF-1R, all of which have an important role in the development of thyroid cancer (11). Sunitinib is currently approved for the therapy of renal cell carcinoma and gastrointestinal stromal tumor on an intermittent treatment schedule (12). Despite the results of preclinical studies, few studies have investigated sunitinib in progressive RAIR TC. In a phase II study including 28 TC patients, sunitinib induced a partial metabolic response (13), and an abstract published at the American Society of Clinical Oncology (ASCO) meeting by Cohen et al. (14) showed promising results on radiologic objective response rate.
In the absence of officially approved drugs, inclusion in a clinical trial should always be the priority for patients with refractory and progressive thyroid carcinoma. Unfortunately, in clinical practice, a substantial proportion of patients cannot be included in any trial for various reasons, such as the unavailability of a protocol or the presence of exclusion criteria, and this has led to the off-label use of TKIs in French referral centers that are part of the TUmeurs THYroïdiennes REFractaires (TUTHYREF) network.
A retrospective multicentric study was conducted on a large cohort of patients to evaluate the efficacy and safety of sunitinib for patients with progressive RAIR TC. The objective of the study was to assess the efficacy on clinical outcomes in RAIR TC treated by sunitinib from six referral centers of the TUTHYREF network.
Materials and Methods
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institution's human research committee.
Study design and patients
All patients with progressive RAIR TC that had progressed within the past 12 months according to RECIST criteria who were treated with sunitinib outside a clinical trial between August 2007 and March 2015 were retrospectively and consecutively included.
Patients were enrolled in one of the six TUTHYREF participating centers. RAIR TC was defined by morphological RECIST (15) progression occurring within 12 months after RAI treatment, or persistent disease after a cumulative dose of 600 mCi (22.2 GBq) or lack of 131I uptake in one or more tumor lesions, as determined by whole-body scan following therapeutic dose of RAI.
Study endpoints and definitions
The primary endpoint was the overall response rate (ORR) and disease control rate. ORR was defined as the proportion of patients with tumor size reduction at the time of maximal response (15): the sum of partial responses (PR) and complete responses (CR). Disease control rate ≥6 months was defined as the proportion of patients with CR, PR, and stable disease (SD) ≥6 months. ORR and disease control rate ≥6 months were also evaluated according to first- or second-line TKI treatment.
Secondary endpoints included evaluation of overall survival (OS) and PFS from the first dose of sunitinib. OS was defined as time to treatment start to death from any cause or censoring at the last follow-up. PFS was defined as the time from treatment start to confirmed progression, death, or censoring at the last follow-up. ORR, OS, and PFS were also evaluated according to first- or second-line TKI treatment and histologic type.
The safety and toxicity profile of continuous daily treatment with sunitinib in this population were also evaluated.
Sunitinib
Sunitinib was administered at a dose of 50 mg/day for four of six weeks, or 37.5 mg/day for three of four weeks, or 37.5 mg/day continuously at the physician's discretion.
Evaluation criteria
The treatment response was assessed according to RECIST v1.1 (15), comparing the pretreatment neck-chest and abdomino-pelvic computed tomography (CT) performed every eight weeks under sunitinib treatment. Responses required confirmation at least four or more weeks after the initial documentation. All the assessments were centrally reviewed by an independent radiologist masked to clinical data (i.e., time to progression or treatment).
Severe acute toxicities were evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE) v4.0.
Statistical analysis
Data are expressed as mean (±standard deviation [SD]) or median (interquartile range [IQR]), according to data distribution. OS and PFS were computed by the Kaplan–Meier method and compared with the log-rank test. A p-value of <0.05 was considered significant. Analyses were performed using Stata v13.0 (Stata Corp., College Station, TX) statistics software.
Results
Patient characteristics
Fifty-seven patients (29 [50.8%] men; M age = 62.2 years; range 43–80 years) with progressive RAIR TC were treated with sunitinib outside clinical trials from August 2007 to March 2015 (Table 1). All of them had a follow-up CT scan available.
TKI, tyrosine kinase inhibitor.
Twenty-three (40.3%) patients had a diagnosis of papillary thyroid cancer, 24 (42.1%) had follicular thyroid cancer, and 10 (15.5%) had poorly differentiated tumors. Distant metastases were located in the lung in 44 (77.3%) cases, in the bone in 27 (47.7%), and in lymph nodes in 30 (50.6%). Sunitinib was the first-line TKI treatment for 32 (56.1%) patients and the second-line TKI treatment for 25 (43.9%) patients. None of the patients received sunitinib as a third-line TKI treatment.
The sunitinib regimen was 50 mg/day for four out of six weeks in 23 (40.6%) cases, 37.5 mg/day for three out of four weeks in 28 (49.1%) cases, and 37.5 mg/day continuously in six (10.3%) cases. Mean treatment duration was 11.8 months (range 1–40 months). The mean follow-up was 21.0 months (range 3–90 months).
Tumor response according to RECIST
The best tumor response according to RECIST criteria is summarized in Figure 1. ORR was 35.1% (20 patients): no CR was observed. Disease control rate ≥6 months was 68.4% (39 patients). Six (10.5%) patients showed disease progression as best tumor response. The mean maximum change in tumor size from baseline was 15% (range 6.94–23.03%).

Maximum changes in tumor size in response to sunitinib therapy for differentiated thyroid cancers.
When sunitinib was used as first-line TKI therapy, ORR was 46.9% (15/32 patients), and disease control rate ≥6 months was 75% (24/32 patients). When sunitinib was used as second-line TKI therapy, ORR was 20% (5/25 patients), and disease control rate ≥6 months was 60% (15/25 patients). There was no significant difference of ORR according to histology subtypes (p = 0.709).
Clinical efficacy and survival
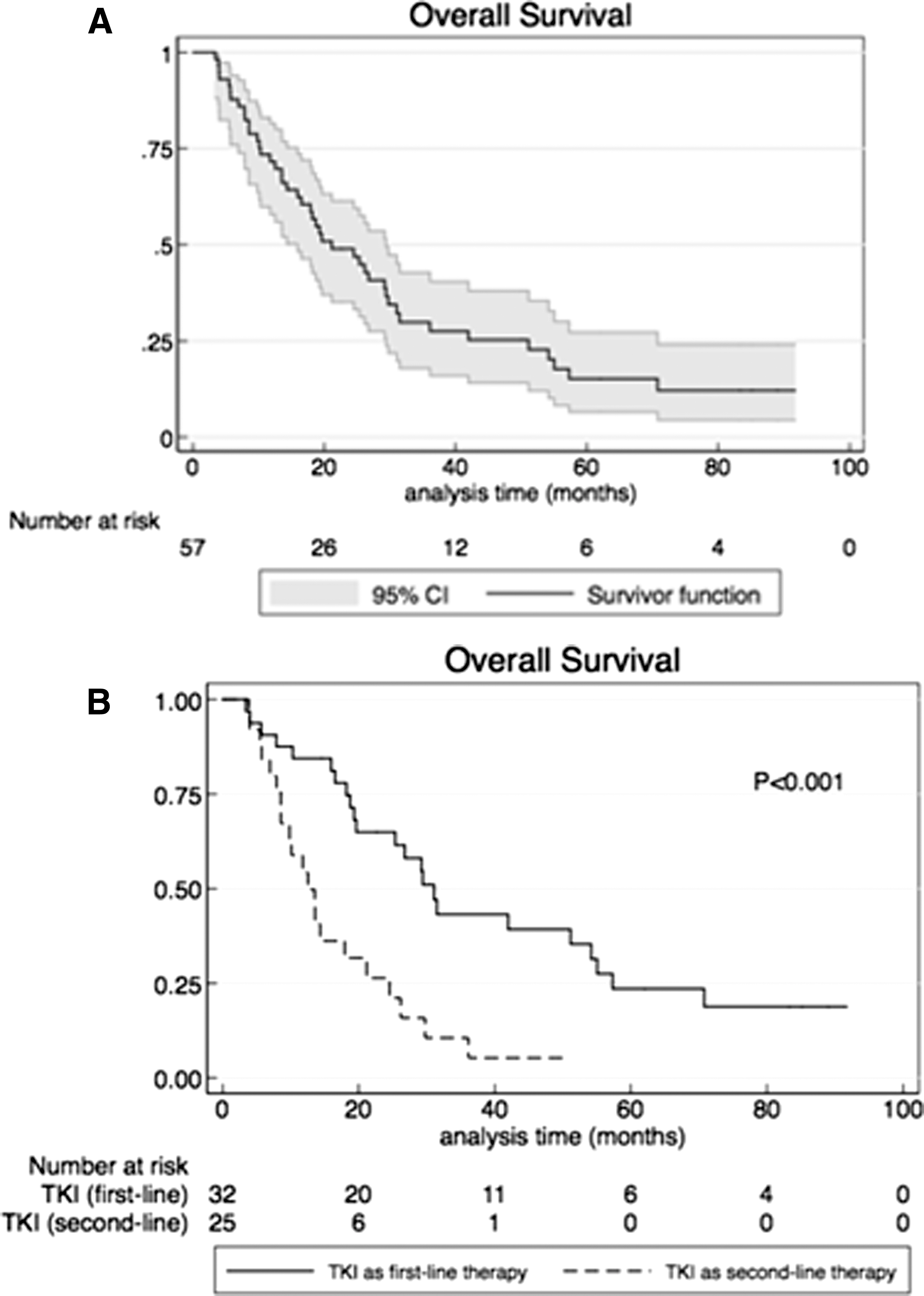
At the time of the primary analysis of OS after a mean follow-up of 21.0 months (range 3–90 months), there were 44 events: 42 patients died because of disease progression, and two died because of cardiovascular disease (one pulmonary embolism and one myocardial infarction). Thirteen patients were still alive at the end of the primary analysis. The median OS was 21.0 months (range 15–29 months). The one- and two-year overall survival rates were 71.6% and 49.0%, respectively (Fig. 2A).
(
All 57 patients presented with disease progression. The median PFS was 10.2 months (range 6–13 months; Fig. 3A). The one- and two-year PFS rates were 42.1% and 12.3%, respectively.

(
Clinical features according to TKI line and histological analysis
OS and PFS differed between patients receiving sunitinib as first-line TKI treatment (group 1) and patients who received sunitinib as second-line TKI treatment (group 2; Figs. 2B and 3B). Patient characteristics according to first- and second-line TKI therapy are summarized in Table 2.
Group 1 received sunitinib as first-line TKI therapy, and group 2 received sunitinib as second-line TKI therapy.
The median OS in group 1 was 30 months (range 19–53 months), which was significantly higher than 13 months (range 8.0–20.0 months) in group 2 (p < 0.001; Fig. 4). Median PFS for group 1 was 15 months (range 7–21 months), which was significantly higher than for group 2 (6 months; range 5–11; p = 0.037; Fig. 5). No differences were found in OS (p = 0.121) and PFS (p = 0.78) according to the initial histological subtypes (Figs. 4 and 5).
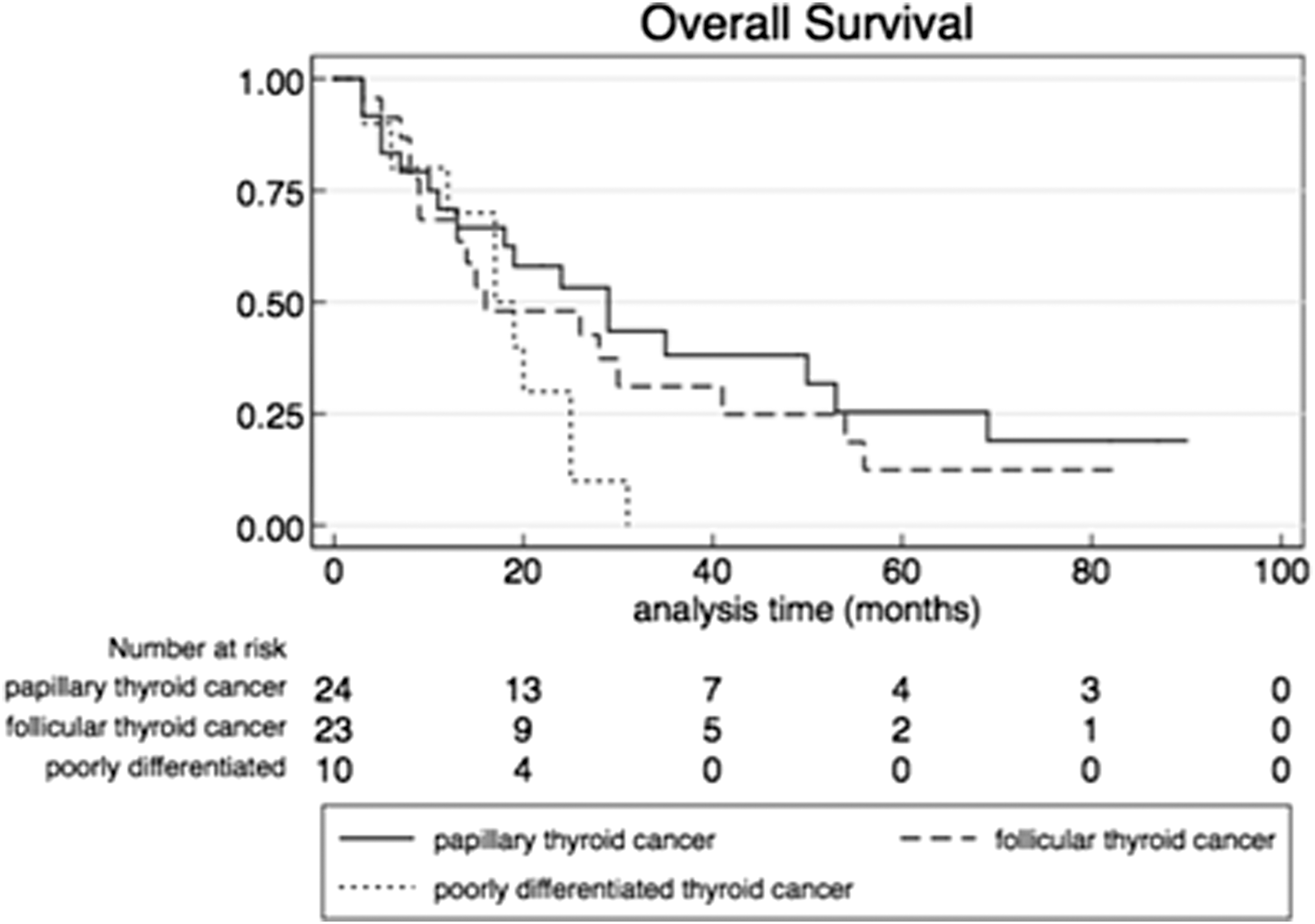
OS according to histologic type (p = 0.121).

PFS according to histologic type (p = 0.78).
Toxicities and complications
The most frequent toxicities (grade 2 or more) were asthenia (17.5%), neutropenia (15.8%), hand/foot syndrome (12.3%), and mucositis (12.3%; Table 3).
One proteinuria grade 3, one cardiac insufficiency grade 3, one pulmonary embolism grade 4, one HTA grade 4 (hypertensive encephalopathy), and one brain hemorrhage grade 4.
Eleven (19.3%) patients experienced grade 3 toxicities, and four (7.0%) patients experienced grade 4 toxicities. No treatment-related death was observed. The most frequent grade 3 or more toxicities were neutropenia (10.5%), asthenia (8.8%), thrombocytopenia (7.0%), mucositis (7.0%), and hand/foot syndrome (7.0%). One grade 3 proteinuria with nephrotic syndrome occurred with recovery of the kidney function after drug withdrawal. One grade 3 cardiac insufficiency occurred with recovery of the left ventricular ejection fraction after drug withdrawal. The grade 4 toxicities were brain hemorrhage (one patient), pulmonary embolism (one patient), and hypertensive encephalopathy (HTA; one patient). One patient died secondary to myocardial infarction 10 months after sunitinib was stopped. This death was not considered a toxicity-related death.
Treatment was withdrawn in 10 (17.5%) patients because of toxicities, and treatment doses were decreased in nine (15.8%) cases.
Discussion
Angiogenesis is a relevant therapeutic target in thyroid cancer. The two antiangiogenic drugs sorafenib and lenvatinib are currently approved for progressive RAIR TC. In the DECISION phase III study, median PFS was 10.8 months for sorafenib (5). Median PFS was 18.3 months for lenvatinib in the SELECT phase 3 study (6). The present study reports the largest cohort of patients treated with sunitinib for RAIR TC.
There are a number of recent reports on the rationale for therapy with sunitinib. Overexpression of VEGF and other growth factors is commonly found in thyroid tumors, particularly those bearing BRAF mutations (16,17). Targets of sunitinib include vascular endothelial growth factor receptors type 1 and 2 (VEGFR1 and 2), platelet-derived growth factor receptors (PDGFRs), and Akt phosphorylation (18,19). All these data suggests efficacy of sunitinib. However, only few studies evaluated sunitinib as first-line TKI, and the number of patients included was low. The present results are in agreement with those of previous studies showing an objective response rate ranging from 13% to 28% (13,14) and a median time to progression of 12.8 months (13). As previously reported, tolerance was manageable and similar to that found in prior clinical trials for the treatment of others cancers.
Importantly, new insights about the role of second-line anti-angiogenic therapy in thyroid cancer are reviewed here. Twenty-five patients included in this study received sunitinib after progression on a first-line anti-angiogenic drug. In this specific cohort, objective response rate and median PFS were 20% and 6 months, respectively. It is shown here that sunitinib was associated with moderate clinical activity, even in patients refractory to first-line antiangiogenic drugs, reflecting the differential binding capacities of TKIs to angiogenic kinases, as previously reported (20,21). Dadu et al. (21) compared a group of 25 patients receiving salvage therapy after sorafenib failure with a group of 35 patients receiving no treatment after sorafenib failure or still receiving sorafenib despite failure. Median PFS and OS were significantly longer with salvage therapy compared with sorafenib alone. However, salvage therapies were heterogeneous, and only 10 patients received sunitinib in this study. In the SELECT study, 20% of patients received lenvatinib as second-line TKI, and results were similar to first-line therapy with lenvatinib (5).
The present study has the limitation of being a retrospective study design with a limited number of patients and the lack of a control arm. Patients in groups 1 and 2 were not homogeneous, and responses according to metastases sites were not evaluated in this study. In the study by Cabanillas et al. (20), responses were better in lung metastases than they were in lymph nodes and bone metastases. Similar results were found by Massicotte et al. (22). Another limitation is that the relationship with BRAF and KRAS status was not evaluated. Sunitinib was found to be ineffective in KRAS- or BRAF-mutated thyroid carcinoma cells. Sunitinib-resistant cells lines were shown to be heterozygous for the KRAS G12R mutation, and all sunitinib-sensitive TC cell lines exhibited wild-type KRAS and BRAF genotypes (23).
In conclusion, the present study shows that sunitinib is potentially associated with clinical benefit, especially as a first-line agent. Further prospective studies are needed to evaluate the effectiveness of sunitinib in progressive RAIR TC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.