
Abstract
Background:
Hypermetabolism of thyroid nodules on 18F-fluorodeoxyglucose positron emission tomography (PET) is associated with a higher prevalence of malignancy. However, the definition of hypermetabolism and its impact on cytological interpretation are unclear.
Methods:
Medical records of all patients with thyroid nodules who had undergone cytological evaluation at the Moffitt Cancer Center between October 2008 and May 2014 were retrospectively reviewed. Those with a PET scan performed within one year of the cytology composed the study group, and the rest were used as controls. The distribution of the cytological categories, percentage of resection, and prevalence of malignancy among each Bethesda category was compared between both groups.
Results:
Fifteen percent (436) of all thyroid nodules with cytological evaluation were in the study group. Maximum standardized uptake values (SUVmax) were directly associated with the probability of having a malignant or a follicular neoplasm cytological diagnosis; and inversely associated with the probability of having a benign cytological diagnosis. However, the prevalence of cancer within each Bethesda category was not associated with SUVmax values. It was found that the prevalence of malignant cytology increased to >5% with SUVmax values ≥2.5. SUVmax values were significantly higher in malignant than in benign nodules on histology (mean values 10.8 vs. 5) but with significant overlap between both groups for either the whole cohort or nodules with indeterminate cytology only limiting its use for differential diagnosis.
Conclusions:
The prevalence of malignancy in thyroid nodules with a SUVmax <2.5 is similar to the general population, and management should not be modified in those patients. The increased prevalence of malignancy among hypermetabolic thyroid nodules (SUVmax ≥2.5) is well characterized by cytology and does not impact the interpretation of cytological categories. Therefore, SUVmax value does not add relevant information once cytology is available.
Introduction
T
This study aims to answer two questions. First, is there a SUVmax threshold that should be considered to modify the standard management of thyroid nodules, and if so, what is it? Second, does hypermetabolism, by increasing the pretest prevalence of malignancy, impact the interpretation of thyroid cytopathology?
Patients and Methods
In this retrospective Institutional Review Board–approved study, the medical records of patients with thyroid cytopathological evaluations performed at Moffitt Cancer Center between October 2008 and May 2014 were reviewed. All cytological diagnoses followed the Bethesda System for Reporting Thyroid Cytopathology (Bethesda; non-diagnostic, B-I; benign, B-II; atypia/follicular lesion of undetermined significance, B-III; follicular/Hürthle cell neoplasm, B-IV; suspicious for malignancy: B-V; malignant: B-VI). The prevalence of malignancy for each Bethesda category was estimated on resected nodules, for which there was a clear histological correlation. In nodules with multiple biopsies, only the most recent cytology report was used for the study. Final histological diagnosis was obtained from a review of histology reports. Only the histology of the biopsied nodule was used to assess the prevalence of malignancy in each Bethesda category; other nodules within the thyroid (including incidental malignancies in nodules that had not undergone FNA) were not included in the denominator or the numerator of the calculation. In four nodules, focal areas of microcarcinoma were detected within an otherwise benign-appearing nodule. These nodules were included in the malignant group, but the pathological size of the malignant foci was used as the pathological size of the tumor.
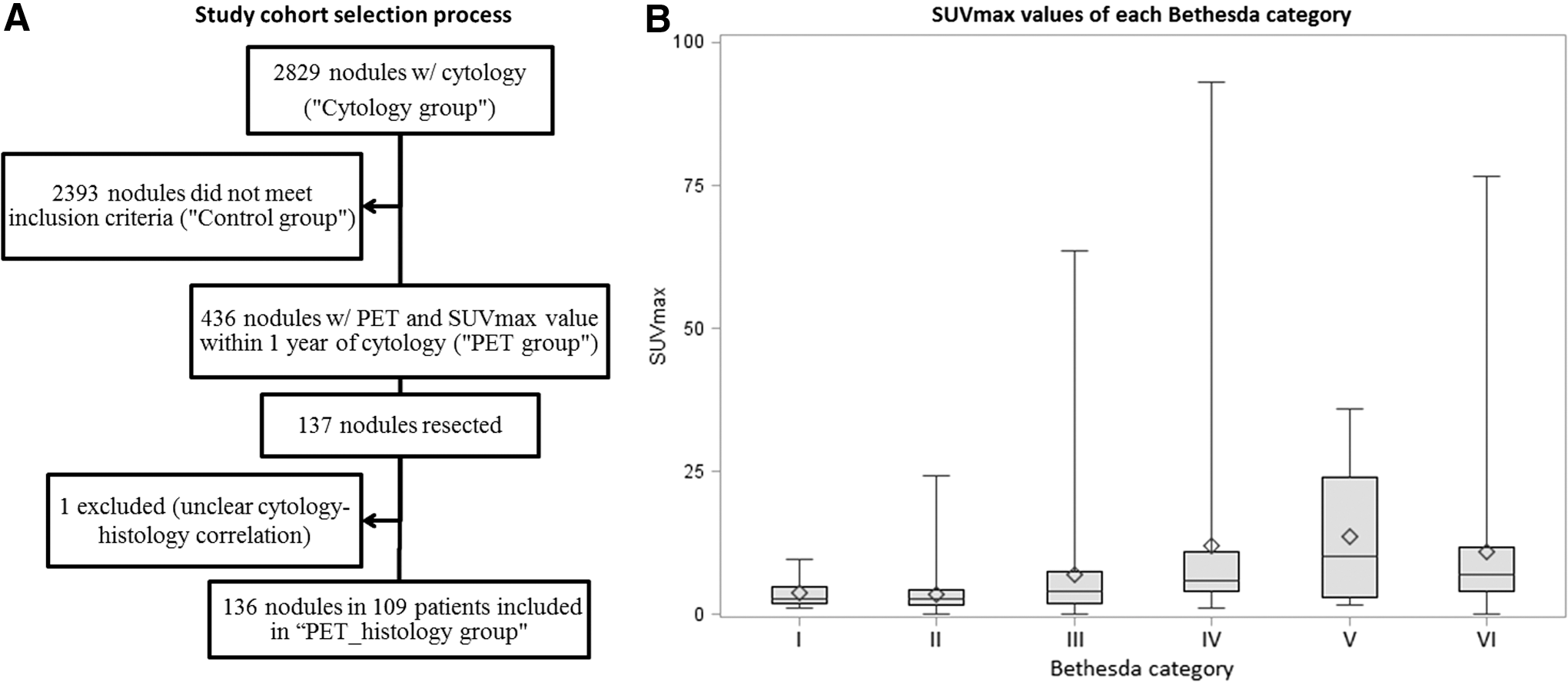
For the purpose of this study, patients with PET (or PET/CT) scan imaging performed within one year of their thyroid cytological evaluation who had a reported SUVmax for the thyroid nodule biopsied or images available for review were selected. Most of these PET scans were done for the evaluation of another malignancy. A nuclear medicine specialist (J.M.-S.), with expertise in PET scan imaging, reviewed images of 241 nodules in which SUVmax was not specified or when correlation with the nodule biopsied was unclear per report. In 35 of them, SUVmax was not measured due to system incompatibility, and these were excluded. Of a total of 436 nodules with SUVmax available (PET group), 137 were resected, but one had an unclear cytology–histology correlation. Finally, 136 nodules were included to calculate the prevalence of malignancy within each diagnostic category of the Bethesda system (PET_histology group; Fig. 1A). The distribution of the cytological categories, percentage of resection, and prevalence of malignancy among each Bethesda category was compared against the patients in the Cytology-group who did not meet criteria for inclusion in the PET-group (Control group).
(
“Significant hypermetabolism” was defined as the SUVmax threshold above which the percentage of malignant diagnosis by cytology in the PET group was above the national average (around 5%), according to a recent meta-analysis (7).
Analysis cohort comparisons were made with Fisher's exact test for categorical variables and the Wilcoxon–Mann–Whitney test for continuous variables. The p-values for mean SUV group comparisons were calculated using the Kruskal–Wallis test. All p-values are two-sided unless otherwise stated, and were considered statistically significant at the 0.05 level. All statistical analyses (including plots and charts) were performed using SAS v9.4 (SAS Institute, Cary, NC).
Results
Basal characteristics of the PET_histology group are compared with the rest of the PET group in Table 1. Patients with nodules in the PET_histology group were younger and less often diagnosed with another malignancy, and resected nodules had higher SUVmax and were more likely to have a malignant or indeterminate cytological diagnosis when compared with the rest of the PET group. When analyzing individual cytological categories, there were no differences in SUVmax between nodules in the PET_histology group and the rest of the PET group, except for the B-IV and B-VI categories. Interestingly, in both groups, the SUVmax was lower on average for the PET_histology group than in the non-resected nodules (10.4 ± 18.4 vs. 13.1 ± 16.1, p = 0.03, for B-IV nodules; 9.9 ± 12.2 vs. 12.9 ± 14.2, p = 0.04, for B-VI nodules). There were three groups with a significantly different SUVmax value according to the cytological category (Fig. 1B): (i) B-I and B-II (median 2.7; range 0–24.3); (ii) B-III (median 3.9; range 0–63.5); and (iii) B-IV, B-V, and B-VI (median 7.0; range 0–93; p < 0.001). However, all groups had a significant overlap of SUVmax.
p-Values for categorical variables from Fisher's exact test and for continuous variables from Wilcoxon–Mann–Whitney test.
Age at the time of FNA.
Missing data for eight patients from the resected group and 10 patients from the non-resected group.
Absolute value of time from FNA to PET.
PET, positron emission tomography; SD, standard deviation; US, ultrasound; SUVmax, maximum standardized uptake; FNA, fine-needle aspiration.
The cytological diagnosis, rate of resection, and prevalence of malignancy within the PET group is compared with the Control group in Table 2. In the PET group, more nodules were classified as B-IV and B-VI and fewer as B-II when compared with the control group. Nodules were less likely resected in the PET group. The rates of resection for categories II, III, IV, V, and VI were 7%, 34%, 47%, 67%, and 67% in the PET group, and 17%, 59%, 79%, 93%, and 92% in the Control group. The overall prevalence of malignancy was higher in the PET group. This observation is likely due to a relatively higher proportion of nodules resected with a malignant cytology in the PET group (40% vs. 25% of all resected nodules in the Control group) because differences among individual categories were not statistically significant, although the p-value for the B-IV category approached significance (p = 0.06).
p < 0.001 for comparisons between the PET group and the Control group, calculated from Fisher's exact test with Monte Carlo estimate.
Based on resected nodules with clear cytology–histology correlation only. Excluded one nodule resected in the PET group (PET_histology group) and 28 in the Control group. Differences in the prevalence of malignancy between both groups were also significantly different (Fisher's exact test, p < 0.001), but differences disappeared when each category was analyzed individually.
On histology, there were significant differences on mean SUVmax between benign and malignant nodules (Table 3). However, significant overlap was again present. Based on the receiver operating characteristic (ROC) curve developed for the PET_histology group, the SUVmax that minimizes the difference between sensitivity and specificity is 4.6, yielding a sensitivity and specificity of 53% and 55%, respectively (Fig. 2A). With this threshold, the positive and negative predictive values achieved in this cohort, with 64% prevalence of malignancy, would be 68% and 60%, respectively. If only the indeterminate categories (B-III and B-IV) are considered in order to develop the ROC curve, the area under the curve is 0.55, confirming the great overlap in SUVmax of benign and malignant nodules within these two categories as well (Fig. 2B).
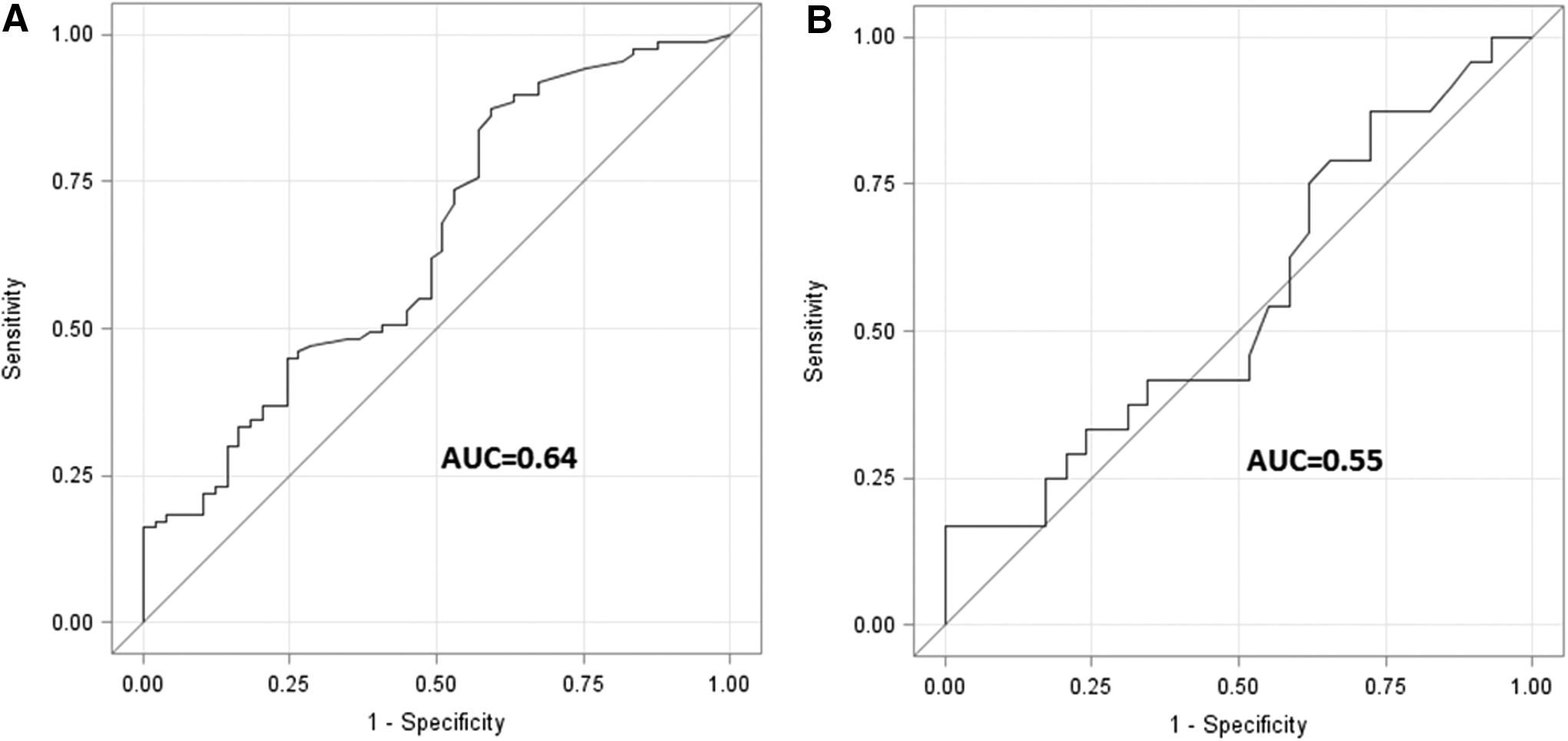
Receiver operating characteristic (ROC) curves for the PET_histology group according to histological diagnosis (benign vs. malignant). (
All benign: includes three nodules with final histology of chronic lymphocytic thyroiditis not included in the breakdown; all had SUVmax >2.5. MNG, multinodular goiter, including hyperplastic and adenomatoid nodules; FVPTC, follicular variant of papillary thyroid carcinoma; Other PTC, other variants of PTC different from the FVPTC; Other, other malignancies.
Below 2.5 SUVmax includes: two MTC and three non-thyroid malignancies (two intrathyroidal PTH carcinomas and one renal cell carcinoma). ≥2.5 SUVmax includes: five follicular thyroid carcinomas (three of them Hürthle cell variant), three undifferentiated (anaplastic)/poorly differentiated thyroid carcinomas, three MTC, one intrathyroidal parathyroid carcinoma, and one tumor of uncertain malignant potential.
Comparison of SUVmax of benign vs. malignant nodules; p = 0.005.
Comparison of SUVmax of multinodular goiter and adenomas; p = 0.01.
Comparison of SUVmax of FVPTC and other variants of PTC; p = 0.01.
Comparison of histological distribution between nodules with SUVmax <2.5 and ≥2.5; p < 0.0001.
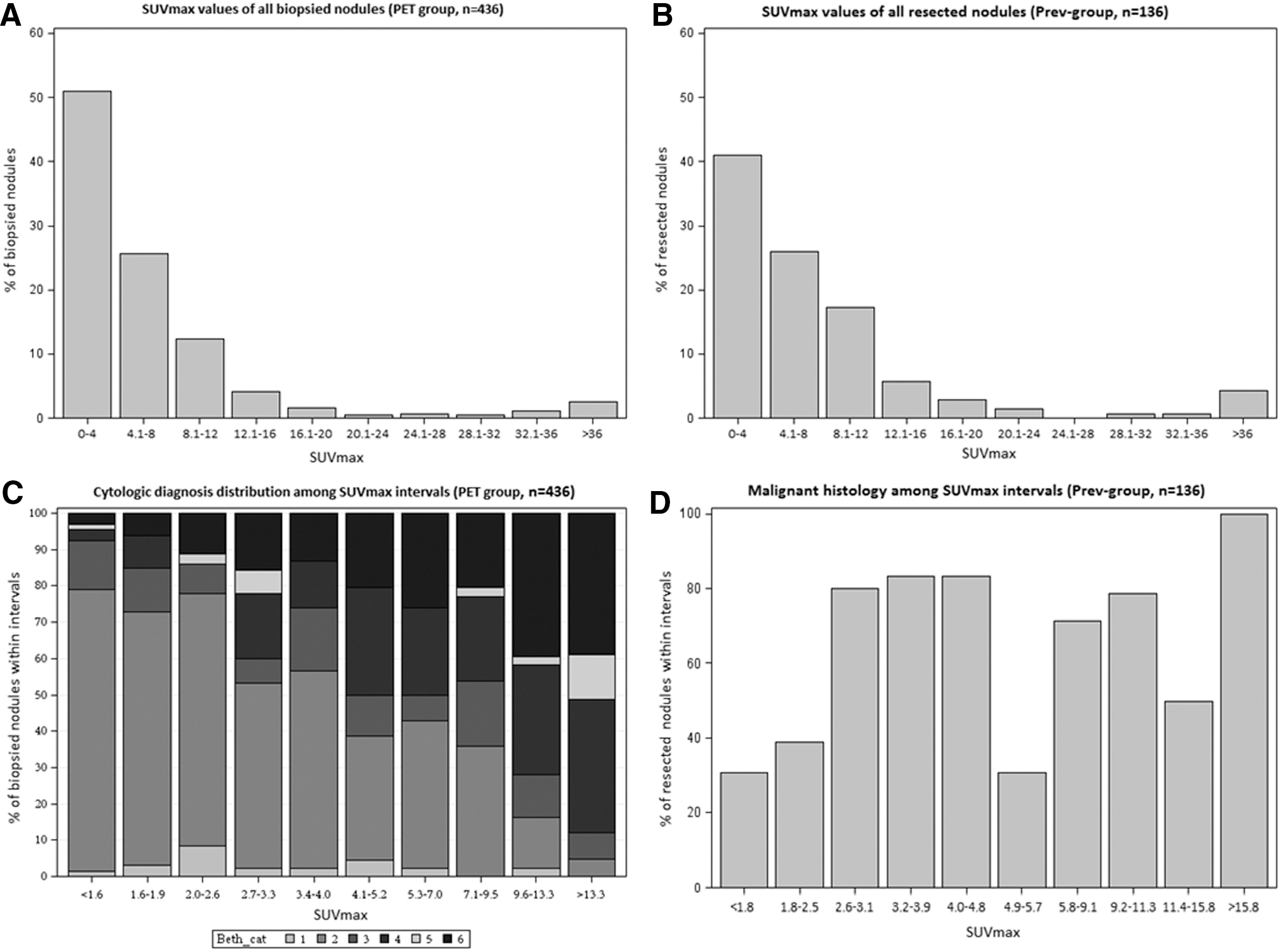
The graphics in Figure 3 represent the distribution of SUVmax in the PET group (Fig. 3A) and the PET_histology group (Fig. 3B), and the distribution of malignant cytology in the PET group (Fig. 3C) and the malignant histology in the PET_histology group (Fig. 3D) along SUVmax. As observed in Figure 3C, the proportion of FNA cytology specimens diagnostic for malignancy increased almost linearly. The proportion of B-IV diagnosis was almost superimposable to that of B-VI, whereas B-II specimens had an inverse distribution to B-VI. The cytological specimens classified as B-III distributed evenly along all SUVmax ranges, representing around 10% of all specimens in each interval. According to these findings, “significant hypermetabolism” was defined as a SUVmax of ≥2.5. Twenty-eight percent (124/436) of the nodules in the PET group had a SUVmax below this threshold, and 75% (75/124) of those biopsies were interpreted as benign, whereas only 5% (6/124) of the specimens were diagnostic for malignancy. Conversely, 35% (109/312) of the nodules with a SUVmax ≥2.5 had a benign cytology, whereas 24% (76/312) had a malignant cytological diagnosis. The distribution of cytological categories between nodules with a SUVmax <2.5 and ≥2.5 was significantly different (p < 0.0001). The distribution of final pathological diagnosis was also significantly different between nodules with a SUVmax <2.5 and ≥2.5 (p < 0.0001; Table 3). Eleven percent (10/87) of all malignancies on histology were below this threshold, and 70% of them had a cytology diagnostic or suspicious for malignancy. The prevalence of malignancy among resected thyroid nodules with indeterminate cytology and a SUVmax <2.5 was 33% (3/9). There were no differences in the prevalence of malignancy of thyroid nodules with indeterminate cytology below or above the proposed threshold (data not shown). All resected nodules with benign cytology were confirmed as benign on histology.
(
Discussion
This study demonstrates that the increase in the prevalence of malignancy observed in hypermetabolic thyroid nodules is well characterized by cytology and has a linear correlation with SUVmax. At the same time, this study suggests that SUVmax does not influence the interpretation of thyroid cytopathology. Finally, the SUVmax threshold (2.5) beyond which the prevalence of malignancy exceeds that of the general population was identified.
The study has several limitations, starting with the retrospective design. Another limitation is that it is a single-center study, which limits its external validity. PET (or PET/CT) scans were done either at the authors' institution or at an outside center, and may have used different protocols for acquiring images. This may have an impact on the SUVmax measurement, partially limiting the use of absolute values. However, this replicates the real world in the clinic were a physician may deal with images obtained in different centers under different conditions. Nodules of patients with multiple thyroid nodules were also included, which may complicate the correlation of the nodule biopsied and the nodule described on the PET scan. To limit this error, an experienced nuclear medicine specialist (J.M.-S.) reviewed the images in all cases in which this correlation was unclear per report (47% of all nodules in the PET group), minimizing this risk. Conversely, the pathological diagnoses have strong consistency, since all cytological and 98% (133/136) of the histolopathological specimens were interpreted at the authors' institution's pathology department.
The data from the authors' cancer center have allowed a large population of patients with thyroid nodules evaluated with PET (or PET/CT) scan for another malignancy to be accumulated. This places the authors in a unique position to describe the metabolic rate of thyroid nodules in general and its association with cytological diagnosis. Nonetheless, this cohort could be biased by the fact that patients with incidental hypermetabolic nodules could have been more likely brought to the attention of the physician and therefore biopsied. In fact, the proportion of specimens classified as follicular neoplasm or malignant by cytology is higher than it is in the Control group. These cytological categories have higher mean SUVmax than other categories do, which might have triggered the biopsy. However, 206 nodules were not described in the PET scan report, or SUVmax was not specified. In fact, only nine of these nodules that had images reviewed had a SUVmax >10, and the average SUVmax for the other 197 nodules was 2.4 (median 1.8). Interestingly, this SUVmax is concordant with the threshold that is proposed to define significant hypermetabolism. The elevated rate of patients with another malignancy (90%) is also responsible for the low rates of resection observed (30%) in this cohort. In fact, nodules in patients without other malignancies were more often resected than in patients with other known malignancies. This likely led to a selection bias, increasing our overall prevalence of malignancy and, specifically, among indeterminate cytological categories, as resection could be preferentially offered to patients with the most suspicious nodules. It is unknown whether higher rates of resection would have changed the findings.
Several studies have explored the use of PET scan imaging to improve the cytological diagnosis accuracy in thyroid nodules with indeterminate cytology (10 –18). All of them selected patients with cytological indeterminate thyroid nodules who were surgical candidates to be evaluated with PET scan before surgery, searching for a SUVmax threshold able to differentiate benign from malignant nodules (10 –18). The sensitivity and specificity achieved in these studies by different SUVmax thresholds was around 90–95% and 50–55%, respectively (19,20). However, the results of these studies are difficult to compare due to the heterogeneous, and arbitrary, definition of hypermetabolism. In some series, any focal uptake has been considered as PET positive (10,11,14,17,18), whereas in others, a SUVmax value >2 (12,15), or an area under the SUV curve >175.5 (16), were used as a threshold. Moreover, relying on a precise SUVmax threshold to classify a thyroid nodule as benign or malignant could be inadequate, given the numerous factors that influence SUVmax (21 –24).
Unlike these studies, the present study reviewed all clinical records of patients with biopsied thyroid nodules, independent of whether they were surgical candidates, and looked for patients who had had a PET scan done, typically for another malignancy. This approach reduces selection bias, as many thyroid nodules that were not described in the PET scan report were included, allowing for a descriptive analysis that is not otherwise possible.
This study shows that most thyroid nodules have a relatively low metabolic rate (>50% had a SUVmax of ≤4.0), but with a significant number of outliers (>10% had a SUVmax >12.0; Fig. 3). Most nodules (85%) with indeterminate cytology had a SUVmax ≥2.5. The higher prevalence of malignancy observed in hypermetabolic nodules is adequately characterized by cytopathology and classified as B-VI. There is a linear increase in the rate of thyroid nodules classified as B-IV or B-VI with increasing SUVmax. Conversely, the distribution of B-II is inversely associated with SUVmax, while no effect is observed in the B-III category.
Hypermetabolism does not seem to impact the interpretation of thyroid cytopathological diagnosis. Although the prevalence of malignancy was higher among resected nodules with indeterminate cytology in the PET group (PET_histology group) than it was in the Control group, differences were not statistically significant. This finding is likely due to selection bias, as described earlier. If it is assumed that all non-resected nodules in both the PET group and the Control group are benign, the lowest institutional prevalence of malignancy for the B-III nodules would be 14% and 15.9%, and for the B-IV nodules it would be 21.5% and 23.8%, respectively. Furthermore, a SUVmax threshold with significant clinical value for indeterminate thyroid nodules could not be found, supporting the ATA recommendation of not using PET scan imaging for the characterization of such thyroid nodules (5). It is reassuring that all patients with a benign cytology had a benign final histology, despite this possible selection bias.
It has been suggested that SUVmax might not be very reliable in nodules <1 cm, increasing the yield of false-negative results (10). According to measures on the resected specimen, 24 (17%) nodules were below this threshold. Of these, only one (4%) had a SUVmax of 0.0 and was diagnosed as a 0.7 mm encapsulated, non-invasive follicular variant of papillary thyroid carcinoma (PTC) that had a cytology diagnostic for malignancy. This type of tumor is known to have an extremely low malignant potential, and there is a current debate over whether to change the standard nomenclature to avoid using the term “carcinoma” for these lesions (25,26). On the other hand, only 5/26 (20%) with a SUVmax <1 were <1 cm in size, supporting the reliability of SUVmax in small tumors. Nonetheless, it is unlikely that these small tumors will be biopsied in the future, even in the presence of hypermetabolism, unless there is evidence of extrathyroidal spread, given their demonstrated low rate of progression (27).
Another interesting observation from this study is that different histological diagnoses have different SUVmax values, although again showing important overlap among them. Among benign diagnoses, hyperplastic nodules had a significantly lower SUVmax than adenomas or chronic lymphocytic thyroiditis had. Among malignancies, non-thyroid malignancies, medullary thyroid carcinomas, and follicular variant of PTC have the lowest SUVmax values, and constitute most of the malignancies below the proposed SUVmax threshold. Other variants of PTC and anaplastic or poorly differentiated thyroid carcinomas had similar SUVmax values of around 10. The highest SUVmax was observed among follicular thyroid carcinomas, especially in the oncocytic variants. Interestingly, the SUVmax of the follicular variants of PTC was significantly lower than it was for other variants of PTC and very similar to the SUVmax found in adenomas. This finding would correlate with the recent molecular finding that the gene-expression profile of the follicular variant of PTC is more similar to follicular adenomas than it is to other variants of PTC (28).
The present findings indicate that a SUVmax of <2.5 should not be considered a high-risk feature, and therefore the size threshold for biopsy should not be lowered in those nodules. Conversely, increasing SUVmax above 2.5 should progressively strengthen the recommendation of lowering the threshold for biopsy, as the probability of malignancy increases (Fig. 3C). This threshold is clinically relevant, as 30% of the nodules have a SUVmax of <2.5. Nonetheless, SUVmax is influenced by many factors, making it necessary to evaluate the complete clinical picture in order to decide the most appropriate management.
Conclusions
SUVmax is not useful for the characterization of thyroid nodules with indeterminate cytology due to significant overlap of those that are benign with those that are malignant. Thus, management of thyroid nodules with indeterminate cytology should not be influenced by SUVmax levels. Furthermore, SUVmax levels <2.5 do not increase the average risk of malignancy, and the threshold to biopsy those nodules should not be different from the general population. Conversely, higher SUVmax levels would justify lower thresholds for biopsy, as the prevalence of malignancy increases progressively.
Footnotes
Acknowledgments
Dr. Pablo Valderrabano gratefully acknowledges the financial support from the Alfonso Martín Escudero Foundation (Spain).
Author Disclosure Statement
No competing financial interests exist.