
Abstract
Background:
Chinese data on the efficacy of low- and high-dose radioiodine for thyroid remnant are still absent. The aim of the study was to investigate whether a low dose of radioiodine is as effective as a high dose for remnant ablation in Chinese patients.
Methods:
Patients presenting for radioiodine ablation in the authors' department were included. Inclusion criteria were aged ≥16 years, total or near-total thyroidectomy, tumor-node-metastasis (TNM) stage of pT1–3, any N stage, and M0. All patients were randomly allocated to either the high-dose group of 3700 MBq or the low-dose group of 1850 MBq for remnant ablation. The response to treatment was defined as successful or unsuccessful after a six- to nine-month interval. Ablation was considered to be successful if patients fulfilled the following criteria: no tracer uptake in the thyroid bed on diagnosis whole-body scanning and a negative level of serum thyroglobulin.
Results:
There were 327 patients enrolled between January 2013 and December 2014. More than 95% had papillary thyroid cancer. Data could be analyzed for 278 cases (M age = 44 years; 71.6% women), 155 in the low-dose group and 123 in the high-dose group. The rate of initial successful ablation was 84.2% in all patients, 82.6% in the low-dose group, and 86.2% in the high-dose group. There was no difference between the two groups (p = 0.509).
Conclusions:
In Chinese patients with differentiated thyroid carcinoma, the low dose of 1850 MBq radioiodine activity is as effective as a high dose of 3700 MBq for thyroid remnant ablation.
Introduction
O
Radioiodine (131I) ablation is now the standard treatment for differentiated thyroid cancer following thyroidectomy as prophylaxis against recurrence. However, the optimal radioiodine activity required to achieve remnant ablation remains controversial. According to the 2015 American Thyroid Association (ATA) guidelines (6), a low activity of approximately of 1100 MBq is generally favored. This is based on published original randomized controlled trials (RCTs) and systematic reviews/meta-analyses of such studies, including a systematic review reported recently (7), which suggested that low-dose radioiodine (1100 MBq) is associated with success rates of ablation similar to high-dose therapy (3700 MBq).
However, there are no such RCTs reported to date in China. Currently, in China, most centers use an activity of 3700 MBq, an empiric fixed dose of radioiodine for thyroid remnant ablation. In some other centers, the doses are administered according to the size of thyroid remnant, ranging from 1850 to >4000 MBq. As we know, the physique and dietary habits of the Chinese population are different from those of European and American individuals. Therefore, data from China will be valuable and are urgently needed. Hence, this prospective randomized, single-center study was designed in order to evaluate whether low-dose radioiodine (1850 MBq) is as effective as high-dose (3700 MBq) radioiodine for the ablation of thyroid remnants in Chinese patients with low-risk thyroid carcinoma.
Materials and Methods
Patients
Patients presenting between January 2013 and December 2014 for radioiodine ablation were enrolled in this study. Eligibility criteria were: 16–80 years of age, histological confirmation of papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC) according to the World Health Organization (WHO) criteria, tumor stage T1–T3 with or without lymph node involvement but no distant metastasis (i.e., N0, NX, N1, and M0 in the tumor-node-metastasis staging system), post total thyroidectomy (TT) or near-total thyroidectomy (NTT), with or without cervical lymph node dissection.
Exclusion criteria were the presence of aggressive malignant variants, including follicular variant PTC, tall-cell, columnar-cell, poorly differentiated, and diffuse sclerosing thyroid cancer; pregnant or breastfeeding women; severe co-existing conditions; serious abnormality in hepatic function or renal function; and a white blood cell count <3.0 × 109/L. Patients in whom a distant functioning metastasis was found on post-radioiodine therapy whole-body scanning (WBS) or those who refused to comply with the regular care after ablation were also excluded from the study. All patients signed an informed consent form before enrollment in the study. The study was approved by the Ethics Committee of Shanghai Jiao Tong University of Medical Sciences.
Study procedures and measurements
By using a random number table, patients were randomly assigned to one of two study groups: low-dose (1850 MBq) or high-dose (3700 MBq) radioiodine. The interval between thyroid surgery and ablation therapy was one to six months for all patients. All patients were instructed to discontinue levothyroxine and follow a low-iodine diet for four weeks before ablation. A complete pre-ablation workup was performed, including physical examination, blood routine test, blood biochemistry, neck ultrasonography, electrocardiogram, chest X-ray, serum thyrotropin (TSH-off), serum thyroglobulin (Tg-off), and serum anti-Tg antibodies (TgAb-off) measurements. TSH-off, Tg-off, and TgAb-off were measured by an immunoradiometric assay (IRMA). Thyroid scanning was performed to assess remnant size with 185 MBq technetium-99m pertechnetate given intravenously. Uptake of radioiodine in the thyroid bed was measured 24 hours after administration of 7.4 MBq.
After radioiodine was administered, all patients stayed in a hospital isolation unit until an assessment of radiation risk and clinical conditions permitted discharge. The remaining whole-body radioiodine activity was required to be <400 MBq corresponding to approximately 15 mSv/h dose equivalent rate measured with a Geiger counter at a distance of one meter. 131I WBS and single-photon emission computed tomography (SPECT) were performed three to seven days after ablation using a double-headed gamma camera (Philips Precedence 16) equipped with high-energy parallel-hole collimators.
Study endpoints
The success of ablation was assessed six to nine months after 131I administration. Patients were instructed to start a low-iodine diet and discontinue levothyroxine four weeks before the assessment. Diagnostic 131I WBX (Dx WBS) was performed with a tracer dose of 185 MBq 131I. Neck ultrasonography was performed. TSH-off, Tg-off, and TgAb-off were measured by IRMA.
Ablation was considered successful when patients fulfilled the following strict criteria: (i) absence of tracer uptake (or less than twice the background activity in the thyroid bed on Dx WBS in the thyroid bed); and (ii) serum Tg-off ≤2 ng/mL (8). Patients who did not meet the full criteria of successful ablation were classified as having “unsuccessful ablation” and received an additional radioiodine activity (of at least 3700 MBq) for the second-dose ablation therapy.
Statistical analysis
Descriptive quantitative data are expressed as means ± standard deviation; qualitative data are expressed as percentages. The Kolmogorov–Smirnov test was used to determine whether quantitative data were normally distributed. Student's t-test, the Mann–Whitney U-test, and the Kruskal–Wallis test were used to compare continuous variables, and the chi-square test was used to detect differences in the proportion of cases. For multivariate analysis, a binary logistic regression procedure with both forward and backward stepwise methods was carried out to determine which independent factors are most expected to predict successful ablation at the first post-ablative evaluation. Accordingly, the odds ratios of the successful versus unsuccessful ablation for independent predictors and the corresponding confidence intervals (CI) were estimated. A statistically significant difference was considered when the p-value was <0.05. SPSS v18.0 (SPSS, Inc.) was used for statistical analysis.
Results
Patients
From January 2013 to December 2014, 327 patients were enrolled. Their clinical characteristics are shown in Table 1. Five cases that were revised as T4 stage and three cases as follicular variant PTC (FVP) were excluded. Following the first post-ablation WBS, nine patients were excluded from further evaluation on account of occult metastatic disease: seven with lymph node metastases and two with lung metastases. Thirty-two patients refused to cooperate further with the investigation. The remaining 278 patients formed the basis of the analysis (155 and 123 patients in the low- and high-dose groups, respectively; Fig. 1).
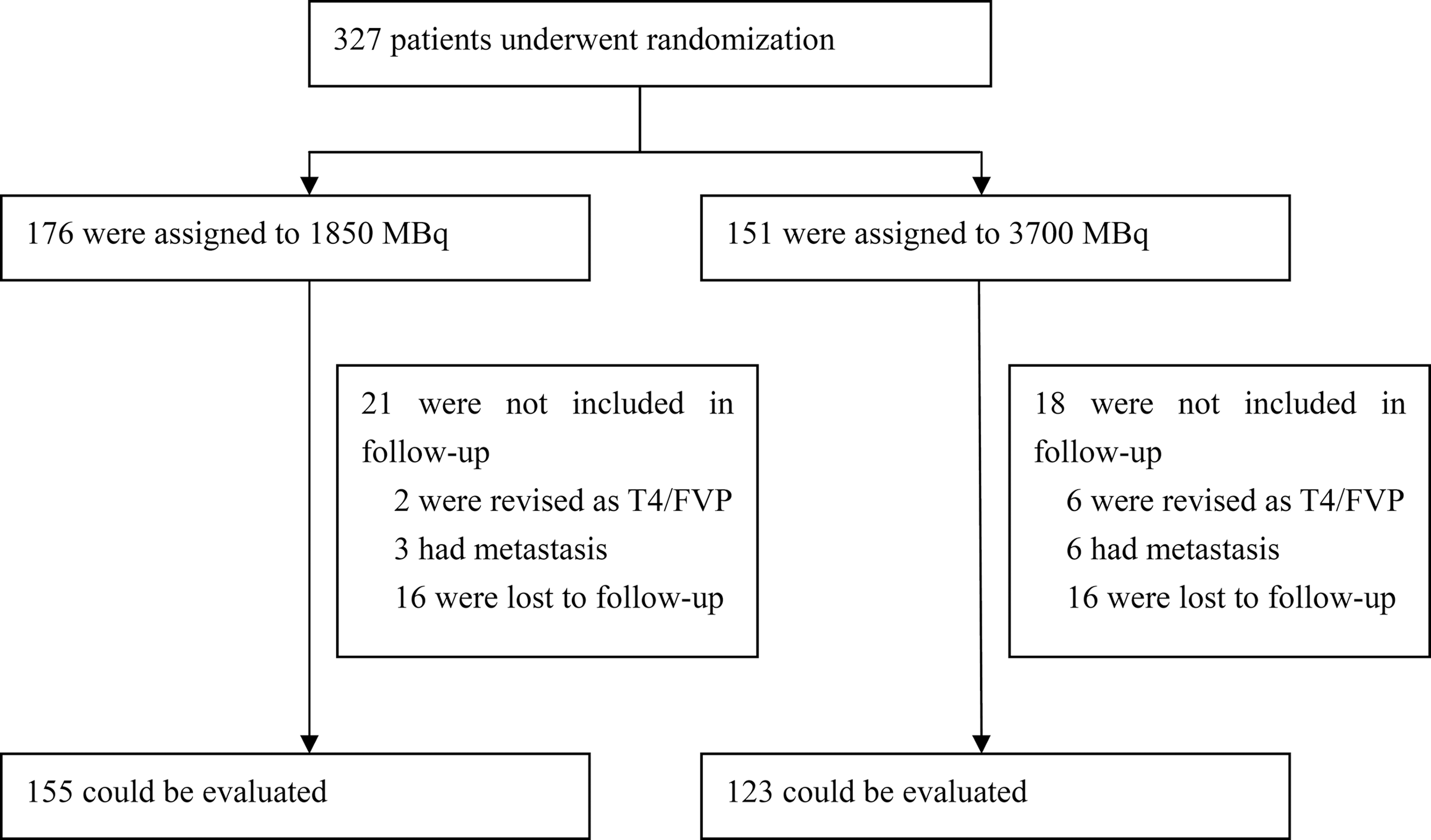
Randomization of the study patients. FVP, follicular variant papillary thyroid carcinoma.
There were no significant differences between clinical parameters, histopathology, tumor stage, postsurgical serum TSH, Tg, and anti-Tg antibody levels between the two groups.
Positive TgAb-off: >30%.
TSH, thyrotropin; TgAb, thyroglobulin antibodies.
The mean age of the patients was 44 ± 13 years (range 16–79 years). One hundred and ninety-nine (71.6%) patients were female. In the first pre-ablation assessment, the mean TSH-off was 68.5 ± 34.0 mIU/L, and the mean Tg-off value was 11.28 ± 22.17 ng/mL. The mean age, sex, type of surgery, histopathology of the tumor, Tg-off, TgAb-off, and TSH-off in the baseline pre-ablation did not differ between the two groups (Table 1).
Ablation success
The rate of initial successful ablation was 84.2% in all patients. Ablation was considered successful in 128/155 (82.6%) patients in the group receiving low-dose radioiodine and in 106/123 (86.2%) patients in the group receiving high-dose radioiodine. There was no evidence of a dose effect on success rates (p = 0.509; Table 2). At the time of the six- to nine-month follow-up, the number of cases with a Tg-off value ≤2 ng/mL was 135 (87.1%) and 110 (89.4%) in the low- and high-dose groups, respectively. The number of cases of increased Tg-off was 10 (6.5%) and 7 (5.7%) in the low- and high-dose groups, respectively. There were no differences between the two groups (p > 0.05).
Predicting factors
Using univariate and multivariate analyses, an attempt was made to find the significant factors that independently influence successful ablation. However, in univariate analysis, all the categorical factors, including the dose of radioiodine, papillary or follicular subtypes, age, sex, residence, time from surgery to ablation, lymph node metastasis, TT or NTT, the baseline serum Tg-off value, TgAb-off value, and TSH-off value, were not significant factors that independently influenced successful ablation (p > 0.05).
Retreatment
A total of 27 (17.4%) patients receiving low-dose radioiodine were given a subsequent second dose compared to 17 (13.8%) patients receiving high-dose radioiodine. Among the patients in the low-dose group, the second radioiodine doses were 3.7 GBq in four patients, 3–4 GBq in 15 patients, and >4 GBq in eight patients. Among the 17 patients in the high-dose group, all second doses were between 3 and 4 GBq. The second radioiodine dose was given mainly because clinicians were concerned about an initially positive scan or an increase in the Tg-off level at six to nine months. By the end of December 2016, the follow-up periods of all patients were two to three years; no recurrences were found in any of the patients.
Adverse events
Short-term adverse effects such as nausea, taste disorders, and salivary-gland dysfunction were not evaluated in this study. However, blood, hepatic function, and renal function were compared between pre-ablation and at six to nine months of follow-up using blood cell counts and blood biochemistry. It was considered abnormal when white blood cells were <3.0 × 109/L, and hepatic function or renal function was higher than the upper limit of normal values when they had been normal before ablation. It was found that there was no significant difference in white cell count, hepatic function, or renal function between the two groups at the six- to nine-month follow-up (Table 3).
Discussion
Several RCTs studying the efficacy of low- and high-dose radioiodine for thyroid remnant ablation have been published. However, data from Chinese thyroid cancer patients are still lacking. Therefore, this prospective randomized study was designed to investigate this issue in Chinese patients. Strict criteria were used to enroll patients with low-risk DTC undergoing TT or NTT with or without cervical lymph-node dissection. Patients with aggressive histologies were excluded. The results demonstrate that the rate of initial successful ablation was 84.2% in all enrolled patients, and low-dose radioiodine (1850 MBq) was as effective as high-dose activity (3700 MBq) for thyroid remnant ablation (82.6% vs. 86.2%; p = 0.509).
As mentioned above, several RCTs have been published studying the efficacy of different doses of radioiodine for thyroid remnant ablation, including two large multicenter trials in the United Kingdom and France (9,10). The design of the two studies was similar to this study, but they compared the efficacy of 1100 and 3700 MBq radioiodine for remnant ablation. Both studies found that low-dose radioiodine is as effective as high-dose radioiodine. Additionally, both trials also assessed the effects of thyrotropin alfa (rhTSH) and thyroid hormone withdrawal on radioiodine treatment for thyroid cancer. However, rhTSH has not been approved for remnant ablation in China. Therefore, the present study could not evaluate this aspect.
In other small-scale randomized studies comparing the efficacy of 1100 and 3700 MBq radioactivity, Fallahi et al. reported that the rate of successful ablation in the low-dose group (1100 MBq; 39.2%) was lower than in the high-dose group (3700 MBq; 64.1%) (11); Johansen et al. reported that ablation was successful in 81% of the low-dose group and 84% of the high-dose group (12); and Mäenpää et al. also found that 1100 MBq was as effective as 3700 MBq (13). In studies using other activities, a large-sample trial in Northern India (14) including 509 participants, which were divided into eight groups treated with different activities ranging from 555 to 1850 MBq, reported that a higher success rate (81.6%) was achieved with activities of ≥925 MBq compared to lower activities (555 or 740 MBq; 61.8%); Caglar et al. found there were no significant differences, using three different criteria, in successful ablation between a low-dose group treated with 800 MBq and a high-dose group (3700 MBq) (15).
As discussed in a previously published systematic review by the authors' group (7), most studies concluded that low-dose radioiodine is as effective as high-dose treatment for remnant ablation. In case of discrepancies, probable reasons include the utilization of different criteria for the definition of successful ablation and the interval between ablation and follow-up evaluation. This study used a strict definition for “successful ablation” based on an off-T4 serum Tg and diagnostic 131I WBS. The interval to assess success of ablation was six to nine months after the administration of radioiodine. At present, in China, the most commonly used activities in different centers range from 1750 to 3700 MBq. Therefore, in this study, the efficacy of 1750 and 3700 MBq was compared. In the future, a multicenter trial will be designed with the aim of assessing the efficacy of lower activities such as 1100 MBq.
This study attempted to construct univariate and multivariate models on the basis of the categorical factors for predicting the outcome of ablation. No significant difference was found in the outcome between papillary or follicular subtypes, age, sex, and TT or NTT procedures. In some other studies, the tumor size, type of surgery, postsurgical radioiodine uptake, and administered activity for ablation therapy were reported to be important factors affecting the outcomes after the first dose (9). In the present study, most patients underwent TT, and the TSH and Tg levels of the enrolled patients varied in small range and were not of predicting value. Moreover, no differences were found in the trend of Tg-off between the pre-ablation and the diagnostic scan time point between the two groups. Moreover, the residence of patients was included in the model because patients in coastal areas have diets rich in iodine, which is supposed to affect ablation efficacy. It was found that location was not a predicting factor, probably because all patients followed a strict four-week low-iodine diet, suggesting that the body iodine content did not affect the ablation outcome.
A limitation of this study, however, is that not all possible short- or long-term adverse effects associated with the administration of higher radioiodine activities were evaluated. Only white cell count, hepatic function, and renal function were analyzed, and it found that there were no differences between the two groups. In the studies by Mallick et al. (9) and Schlumberger et al. (10), patients receiving low-dose radioiodine had fewer early side effects and had a significantly better quality of life than those receiving a high dose. The side effects of radioiodine treatment include nausea, taste disorders, salivary gland dysfunction and dry mouth, dry eyes, as well as transient gonadal dysfunction (16 –18). The risk for radioiodine-induced cancers has not been well established, but the risk of any second primary cancer after initial diagnosis of thyroid cancer is increased approximately 30% over that of the general population (19,20). By the end of December 2016, the follow-up periods of all patients were two to three years, and no recurrences were found in any of the patients. However, long-term follow-up will be required to examine recurrence rates.
In China, a low-dose activity of 1750 MBq is sufficient for thyroid remnant ablation compared to 3700 MBq. This finding is consistent with the results of trials in Europe and other countries. Thus, the use of a low dose of radioiodine for thyroid remnant ablation will be an attractive option for the management of low-risk thyroid cancer that reduces the amount of whole-body irradiation and maintains quality of life. The result may also be helpful for changing the present situation where there are big differences in the doses of radioiodine administered in different centers in China.
Footnotes
Acknowledgments
This study was funded by the National Natural Science Fund (grant 51233007, 81271612, and 81401439), Shanghai Pujiang Program (grant 13PJD022), and Shanghai Health Bureau Fund (grant 20124016).
Author Disclosure Statement
The authors have nothing to disclose.