
Abstract
Background:
Accurate immunoassays measuring minute quantities of hormones are the cornerstone of the practice of endocrinology. Despite tremendous advances in this field, novel pitfalls in these tests emerge from time to time. Oral biotin can interfere with immunoassays of several hormones. The purpose of this report is to relate an extreme case of such interference.
Patient findings:
A patient with progressive multiple sclerosis was found to have extremely elevated free thyroxine, triiodothyronine, and suppressed thyrotropin (TSH) levels. His TSH receptor binding inhibiting antibody level was also elevated. This constellation of laboratory findings suggested a diagnosis of severe Graves' disease. All of the assays yielding abnormal results employed the biotin–streptavidin affinity in their design. The patient had no symptoms of hyperthyroidism, and detailed review of his medications revealed intake of megadoses of biotin. Temporary discontinuation of biotin treatment resulted in complete resolution of the biochemical abnormalities.
Conclusions:
Non-physiologic biotin supplementation may interfere with several immunoassays, including thyroid hormones, TSH, thyroglobulin, and TSH receptor binding inhibiting antibody, leading to erroneous diagnoses. Questioning for biotin intake should be part of the evaluation for patients undergoing endocrine tests. Interruption of biotin supplementation for at least two days prior to biotin-sensitive tests should be sufficient to avoid major misdiagnoses.
Introduction
T
Patient
A 55-year-old man with multiple sclerosis undergoing treatment with fingolimod was referred to the Massachusetts General Hospital Thyroid Unit, as screening thyroid function tests revealed markedly elevated thyroid hormone levels, and suppressed thyrotropin (TSH). A thyroid uptake and scan with 250 μCi of 123I had been ordered prior to the referral, showing a thyroid gland of normal shape and normal radioiodine uptake, 25% after 24 hours. His past medical history included progressive multiple sclerosis, psoriasis, hypertension, and spinal stenosis. His medication list included naproxen, oxybutinin, fingolimod, lisinopril, pregabalin, omeprazole, vitamin D, and simvastatin. He denied any symptoms of hyperthyroidism.
He was in no distress, normotensive, with a normal and regular pulse rate. There was no proptosis, diplopia, or lid lag. The skin was warm and dry. There was no tremor. The thyroid exam was normal. Examination of the chest, heart, and abdomen was normal, and there was no peripheral edema. Office-based neck ultrasound showed a normally sized thyroid, with normal echotexture and vascularity, and no nodules. Thyroid function tests were repeated. Total triiodothyronine (T3) and free thyroxine (fT4) were both markedly elevated, while TSH was suppressed and the TSH binding-inhibiting antibody test was positive at a high concentration (Table 1). This combination of test results establishes a firm diagnosis of Graves' disease (4). However, the laboratory data were in striking contrast with the paucity of symptoms and signs observed in the patient. Supplementary tests were therefore ordered (Table 1). The thyroglobulin level was low at 3.9 ng/mL, with negative thyroglobulin antibodies, a finding inconsistent with Graves' disease, and a bioassay for the thyroid-stimulating antibodies was negative. The sex hormone binding globulin was in the normal range. The patient was questioned again regarding his medication list and reported having recently started treatment with biotin, 100 mg three times daily as treatment for his multiple sclerosis, based on a recent pilot study showing benefit (5). He obtained the preparation from a local compounding pharmacy. The patient was asked to stop the biotin treatment temporarily, and two weeks later repeated thyroid function tests showed completely normal results (Table 1). No other change was made to his medication list, and he continued to feel well. Biotin treatment was resumed thereafter.
Assays in which the streptavidin–biotin interaction is employed in the formation of a solid phase.
Discussion
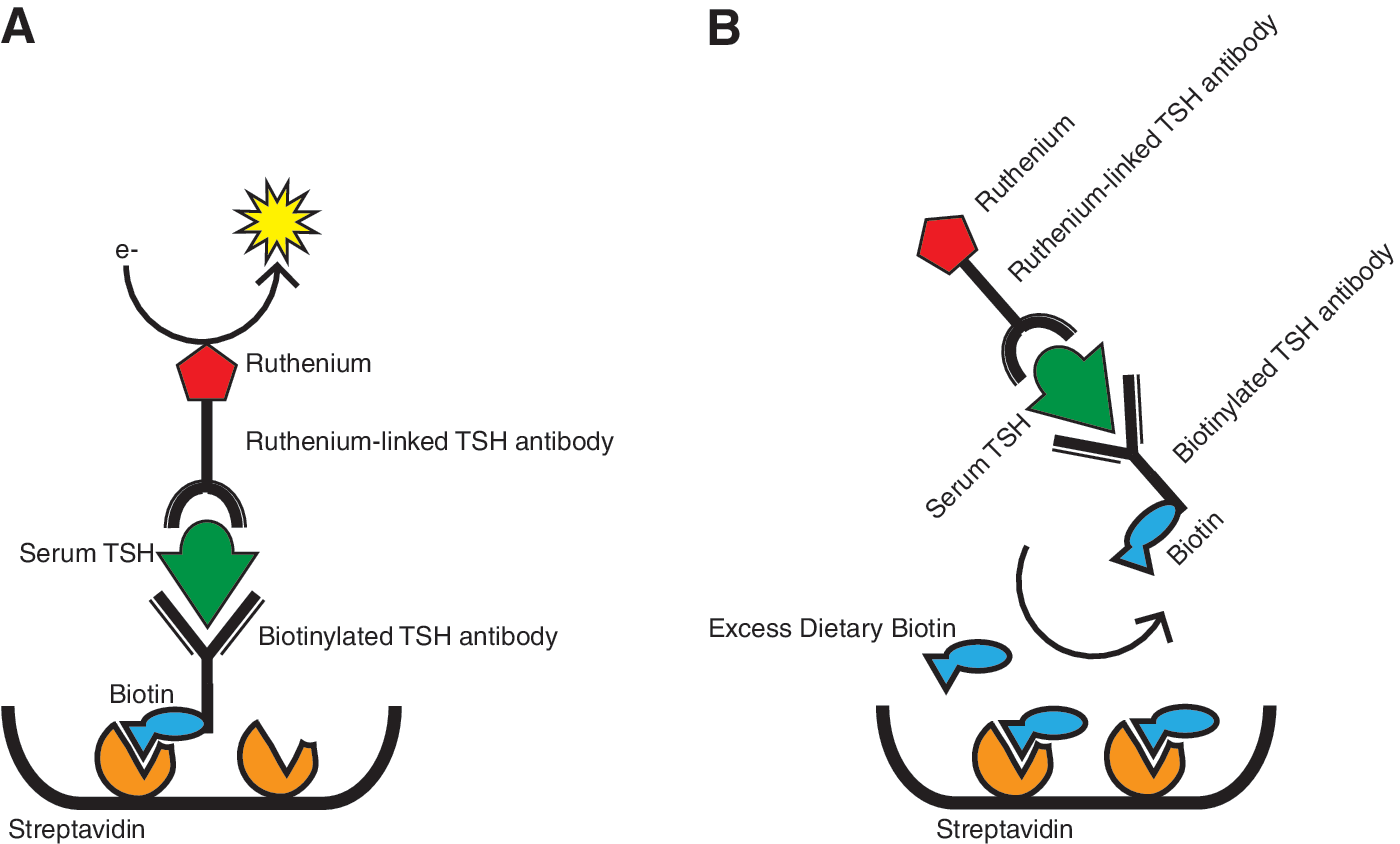
This patient displayed markedly abnormal thyroid function tests in the absence of symptoms of thyroid dysfunction. All the abnormal tests where obtained with immunoassays employing the streptavidin–biotin immobilizing system. The complete restoration of normal thyroid function tests just two weeks after the interruption of megadose biotin treatment suggests the latter as the cause of the biochemical abnormalities observed. Streptavidin, a protein produced by Streptomyces avidinii, binds biotin with a dissociation constant of 10–15 M, an affinity 10–3–10–6 times higher than most antibodies show for their specific haptens (6). This extremely high affinity, together with the ease by which the small biotin molecule can be incorporated in enzymes or small molecules, has made the system extremely useful in precision immunometric assays. In the T3 assay used in this patient (Fig. 1A), the serum sample is incubated with a T3-specific antibody, linked to a ruthenium complex. Biotinylated T3 competes for unoccupied sites on the ruthenium-labeled antibodies (Fig. 1B). Streptavidin-coated magnetic microparticles then capture the biotinylated T3-antibody complex on the surface of an electrode. Application of a current to the electrode results in light emission from the ruthenium (chemiluminescence). The emitted chemiluminescence will be inversely proportional to the T3 level in the serum sample. Large biotin excess in the serum sample is expected to saturate the streptavidin binding sites, resulting in little or no labeled T3-antibody complex binding to the electrode, and hence a falsely elevated T3 level. In contrast, the TSH assay used for this patient, employs a typical “sandwich” design (Fig. 2A). The serum sample is incubated with a mixture of a biotinylated monoclonal TSH antibody, and a ruthenium-labeled monoclonal TSH antibody. The immune complexes formed between the two antibodies, and the TSH in the serum is then captured by streptavidin-coated magnetic microparticles. The chemiluminescence produced upon application of a voltage will in this case be directly proportional to the TSH level in the serum sample. Large biotin excess in the serum will result in reduced binding of the immune complexes to the solid phase (Fig. 2B), and hence a falsely low TSH level. This interference from biotin may be particularly intense in the Roche system, in which the solid phase is generated only after the patient's serum is added to the mixture. Other assays, in which the interaction between biotinylated antigens or antibodies and streptavidin is established before the incubation with the sample, may be more resistant to this interference.

Mechanisms of biotin interference in different assay systems. (
(
It is interesting to note that the sex hormone binding globulin level, also measured with an assay employing biotin, did not appear to be affected as much. The reason for this discrepancy remains uncertain. Other assays, in which the biotinylated antigens or antibodies are allowed to react with streptavidin before the serum sample is added, may also be less sensitive to this interference.
Biotin, also termed vitamin H, is a component of the normal diet and an important co-factor in enzymatic carboxylation reactions (7). The estimated daily requirement for biotin is 30–100 μg daily (8). Normal circulating biotin levels range from 220 to 3000 pg/mL. Biotin supplementation is widely marketed in the United States as a remedy for common hair and skin problems, and it is available over the counter in all retail pharmacies in dosages up to 10 mg, greatly exceeding the daily requirements.
The interference of pharmacologic biotin levels in immunoassays of hormones has been previously described in a few case reports. Waghray et al. described two cases of unexplained low parathyroid hormone (3). Kwok described falsely depressed TSH in a girl taking biotin supplementation (1). Indeed, the package inserts for all the assays described in this paper include a warning on biotin interference, but these inserts are not readily available to clinicians. This case is unique because of the magnitude of the observed interference and the ill-fated combination of falsely low and falsely elevated test results, from which a biochemically consistent but completely erroneous diagnosis of severe Graves' disease hyperthyroidism was derived. Indeed, elevated free and total thyroid hormone, suppressed TSH, and elevated TSH binding inhibiting antibodies should be considered unequivocally diagnostic for Graves' disease (4). A patient with test results in the range described in this report could easily be treated with radioiodine or submitted to a thyroidectomy in error. Clearly, the magnitude of the described laboratory artifacts must be related to the extremely high dose of biotin taken by the patient—about 3000 times the upper limit of daily requirements. However, it is possible that cases less dramatic and therefore more difficult to identify than in the patient reported here may occur with smaller doses of biotin. For example, one in vivo study showed a sevenfold increase in the fT4 level two hours after the intake of 30 mg of biotin, followed by a time-dependent decline in the interference over the following 24 hours (2). Several worrisome scenarios can be envisioned. A patient with thyroid cancer might be hurt by a biotin-related underestimation of her thyroglobulin level. Even worse, her falsely low TSH at the same time might be judged to be within the therapeutic target for her condition, a “perfect storm” for a bad outcome. A patient with Graves' disease on methimazole might be advised not to stop her medication based on persistently positive TSH receptor antibody tests, and so on.
While the efficacy of high-dose biotin therapy on hair and skin concerns is not documented in any clinical study, the supplement does not appear to be unsafe. Therefore, a blanket warning against its use seems unreasonable. However, it is important that clinicians actively inquire about biotin intake with their patients. Based on in vivo data from Wijeratne et al. (2), patients taking biotin should be advised to withhold the supplement for at least two days preceding their blood tests.
Footnotes
Acknowledgments
I am indebted to Dr. Samuel Refetoff for alerting me on the possible impact of biotin interference while discussing a separate patient. I also wish to thank the Customer Service at Roche Diagnostics USA for promptly providing the technical information on the assays described in this paper.
Author Disclosure Statement
No competing financial interests exist with the matter of this article.