
Abstract
Background:
There are few published quality metrics relevant to fine-needle aspirations (FNA) of the thyroid and endocrinology. With the development of a Thyroid Nodule Clinic within an academic practice, the Division of Endocrinology, in collaboration with the Department of Medicine Quality Improvement Team, established a system to monitor the results and follow-up of thyroid biopsies to ensure patient safety and to prevent adverse clinical outcomes attributable to delayed or incomplete follow-up.
Methods:
All FNA performed are identified using billing data from the Thyroid Nodule Clinic. Results were followed using the Beth Israel Deaconess Online Medical Record (OMR) system, and information is collected on documented follow-up plan and actions taken. Missing data are flagged for review. Over the reporting period, the monitoring process and categories were modified to account for adoption of the Bethesda reporting criteria and implementation of gene expression classifier testing. Specific workflow plans were developed for each cytopathologic classification.
Results:
Between July 2007 and June 2014, 3895 FNAs were performed. The quality improvement tracking process found that 3856/3895 (99%) biopsy cases had documented follow-up since initiation of the project.
Conclusion:
This monitoring process has ensured quality patient care, with confidence that patients having FNAs are receiving documented necessary follow-up for treatment of their nodular conditions. This system serves as a potential model for others to use in their endocrine practice in managing the results of thyroid nodule biopsies.
Introduction
T
The Institute of Medicine has identified several major deficits, including voids in coverage, loss of information, and poor communication, which prevent patients from receiving evidence-based care that meets their needs (3), and suggested several areas of improvement focused on delivering safe, timely, and effective patient-centered care. In line with these goals, system-wide attempts have been made at improving follow-up of abnormal test results with the goal of limiting harm to patients. It has been estimated that only 65% of abnormal pathology results are communicated back to the patient within an appropriate time period (4 –6), and many malpractice lawsuits find their basis in poor communication and missed diagnoses (7).
The advent of the electronic medical record (EMR) system allows for easier access to laboratory data and pathology and radiology reports, among other benefits, and has improved communication between physicians (8). However, despite online reminders and improved communication, test results are often lost (9), resulting in negative patient outcomes (10). Because of this known danger, there has been increasing interest in improving safety mechanisms and ensuring adequate care coordination.
Coordination can be particularly cumbersome and difficult when several disciplines are involved in a patient's care. This is particularly problematic for management of thyroid nodules, given that adequate patient care often requires input from endocrinologists, radiologists, surgeons, and cytopathologists. Approximately 10% of all thyroid fine-needle aspirate (FNA) results are malignant, with an additional 25% of results classified as indeterminate, atypical, or insufficient (11). With more than a third of all FNA results requiring short-term follow-up testing and/or surgery, it is imperative that patients be aware of these results and action be taken appropriately.
With these goals in mind, the Division of Endocrinology at Beth Israel Deaconess Medical Center (BIDMC) established a multidisciplinary Thyroid Nodule Clinic (TNC), with the aim of providing a collaborative, convenient, comprehensive assessment of thyroid nodules and improved patient care coordination. A QI program was designed and implemented within the TNC to improve communication and enhance patient safety while ensuring evidenced-based medical care was being provided to the patients evaluated in clinic. The authors are not aware of any similar previously described system for monitoring thyroid FNA results, ensuring documentation of follow-up plan and appropriate disposition of results with high reliability.
Methods and Materials
BIDMC is a 600-bed academic medical facility located in Boston, Massachusetts, with >500,000 outpatient visits annually (12). The multidimensional QI and patient safety program of the Department of Medicine includes a comprehensive peer review process and a medical patient care committee, which is tasked with setting clinical priorities and division-based quality measure dashboards, a tool that displays clinical quality data to provide timely feedback on the quality of care provided. Additionally, this committee identifies possible performance improvement projects and is responsible for education of house officers, medical students, and faculty in QI strategies (11).
In line with the goals of the Program for Quality Improvement and Patient Safety (QI/PS) (13) at BIDMC, the Division of Endocrinology sought to improve its own quality measures, with a specific interest in monitoring appropriate follow-up of thyroid nodule FNA pathology results. The TNC is a collaborative effort to provide state-of-the-art care for a variety of thyroid diseases and performs between 600 and 700 thyroid nodule FNA annually. Data collection with the TNC began in July 2007 and is described through June 2014.
Data collection and coordination
Based on billing records from the TNC, FNAs performed by endocrinology and an onsite TNC radiologist were identified. Biopsies ordered by a patient's primary-care doctor, and performed in radiology, were not included in this analysis. Thus, this process tracked only the performance internal to the TNC.
The auditing process is performed on a quarterly basis, allowing at least a four-month and up to a six-month lag time from date of initial FNA. This lag time allows the clinicians adequate time to contact patients with results and capture downstream events, including execution of follow-up based on appropriate disposition of cytologic results. As this QI review was designed as a retrospective assessment of current clinical practice, there were no guidelines imposed on clinicians with regards to appropriate time frame of follow-up, with the expectations that clinicians acknowledge results and communicate with patients in a timely fashion. Physician autonomy allows for a variety of modes of communication with patients, including but not limited to phone calls, letters, and e-mail communication via a secure patient portal, provided that this communication is then documented in the online medical record (OMR). Documentation of disposition is monitored via manual review of BIDMC's OMR system, which houses all outpatient visit notes, laboratory data, and radiology and pathology reports.
Performance indicators
Initial metrics from 2007 to 2010 classified biopsy results into one of the following categories: (i) cytology insufficient, as defined as non-diagnostic or insufficient on FNA cytopathology report; (ii) benign; (iii) indeterminate, which included atypical results, follicular neoplasm (FN), or suspicious for follicular neoplasm (SFN); (iv) malignant, including any notation of malignancy, suspicious for papillary carcinoma, or non-Hodgkin's lymphoma.
The Bethesda reporting criteria (14) system allowed for the standardization of diagnosis of thyroid nodule disease, streamlined communication between healthcare professionals, and provided consistency of recommendations regarding appropriate follow-up and treatment. The BIDMC's cytologic classification system changed from July 2010 in an attempt to be consistent with the newly implemented Bethesda criteria. As a result of the change in classification, the initial “indeterminate” category was subsequently divided into two separate categories, now identified as indeterminate (FN/ SFN) and atypical cytology. For quality assurance and clinical purposes, the Bethesda criteria for “suspicious for malignancy” and “malignancy” remained classified as malignancy. Our quality metrics correlate with the Bethesda criteria, as shown in Table 1.
QI, quality improvement.
Appropriate disposition of thyroid nodule FNA results is based on the 2009 guidelines of the American Thyroid Association (ATA) (15) and is defined in the following manner. Cytology insufficient results should be followed up with repeat FNA. Indeterminate results should be followed with a radioiodine scan, surgery, repeat FNA with Gene Expression Classifier (GEC) testing, or clinical evaluation, which may include watchful waiting with follow-up ultrasound. Radioiodine scans are suggested as a reasonable step in the management of indeterminate results based on the 2009 ATA guidelines. For the purposes of the QI review, no cross-reference with thyrotropin values was performed. Atypical results necessitate repeat FNA with GEC testing and/or surgery, and malignant findings require surgery. The model for implementation of these recommendations is shown in the flow chart in Figure 1. Use of the GEC was implemented in April 2013 to aid in management decisions of atypical/indeterminate nodules. Minimal, if any, changes are needed based on the new 2015 ATA thyroid nodule guidelines, as we have already incorporated GEC testing into our algorithm.
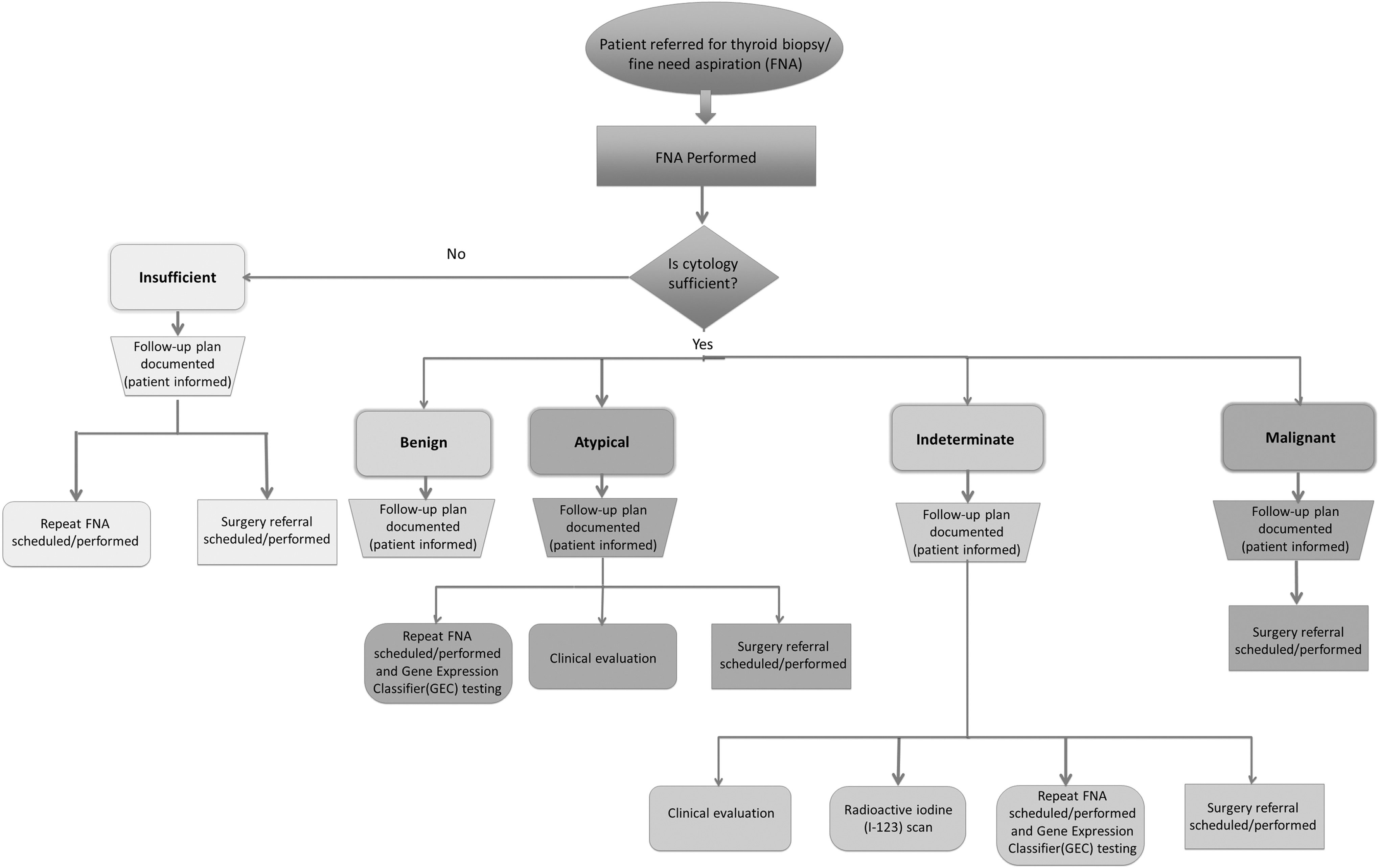
Thyroid biopsy/fine-needle aspiration workflow by cytopathology findings.
Clinical management choices outside of these guideline-based actions or missed follow-up cases are flagged by the project QI analyst to the attending of record. The quarterly monitoring system allows physicians a four- to six-month period to contact patients with results, document follow-up, and execute an appropriate plan. Any patient flagged for missed or inappropriate follow-up during this time period is then evaluated with a re-look within three to six months of the event to determine if appropriate care had been rendered.
Results
There were 3895 FNAs performed between July 2007 and June 2014. In July 2010, the Bethesda criteria were adopted, which split the former “indeterminate” category into “indeterminate” and “atypical,” with appropriate disposition based on ATA guidelines. For the purposes of this analysis, a summary of the data based on the timeline of adoption of the Bethesda criteria as highlighted above into pre-Bethesda and post-Bethesda is provided. In the pre-Bethesda period, 1426 FNAs were performed, with 57% benign, 13% insufficient, 21% indeterminate, and 8% malignant. During the post-Bethesda reporting period, 2469 FNAs were performed, with 56% benign, 19% insufficient, 11% atypical, 9% indeterminate, and 6% malignant (Table 2). Results discussed below reflect the distribution of cytopathologic findings across the entirety of the review period.
FNA, fine-needle aspiration.
Cytology insufficient
Of the 663 cytology insufficient FNA findings, 98% had a documented follow-up plan by the end of each quarter. During the surveillance period, there was a trend toward improved rates of scheduling/performing repeat FNAs, with an average of 86% of patients with appropriate disposition during the 2008–2009 period, improving to 88% by 2013. Notably, there is a subset of patients with insufficient FNA findings who have had multiple insufficient biopsies. These patients may be followed clinically with routine ultrasound monitoring in the absence of any concerning characteristics after initial plans for repeat FNA are in place, as opposed to exposing patients to limitless unsuccessful FNAs. Alternatively, core-needle biopsy can also be considered in select cases of repeated insufficient FNAs and may improve diagnostic yield (16). Core biopsy results were not monitored as part of the system, as these are not performed in the TNC.
Indeterminate
From July 2007 to June 2010, prior to adoption of the Bethesda criteria, 21% of the FNA results were found to be indeterminate, whereas from July 2010 forward, 9% of the FNA results had a cytopathology finding designated as indeterminate (FN/SFN). A follow-up plan was documented for 100% of patients whose FNA was classified as indeterminate. Prior to adoption of the Bethesda system, 55% of patients with an indeterminate finding were referred for surgery. Post adoption of the Bethesda classification and recommendations, referrals for surgery increased to 64%. Of those patients with indeterminate FNA results who were referred for surgery, 93% had the surgery done within six months of the index FNA (Table 3). Surgical results were not monitored as part of this process. Since implementation of GEC testing in April 2013, 31% (21/68) of FNAs classified as indeterminate were re-biopsied for GEC testing. Fourteen were found to be benign by GEC, while seven remained suspicious and were referred for surgery.
Clinical evaluation (watchful waiting, follow-up ultrasound) was introduced as a disposition during the interim period after the adoption of the Bethesda classification and prior to the availability and implementation of Gene Expression Classifier (GEC) testing.
Denominator for surgery done comes from surgery referral.
Atypical
From July 2010 to June 2014, 260 specimens (11% of FNAs performed in the TNC) were classified as atypical, and 98% had a documented follow-up plan. Of these patients, 171 (65.7%) were referred for repeat FNA, and 34.2% were referred directly for surgery. By six months following the initial FNA, 81.2% had the repeat FNA completed; 102/111 patients referred for surgery underwent surgery by the six-month assessment. Of the 42 GEC tests performed, 27 were classified as benign, and 15 returned as suspicious, resulting in surgical referral.
Malignant
Of all patients with a malignant finding, 99% had a follow-up plan documented. Of these, there was documentation that 97% of patients were referred to surgery, with 93% completing surgical resection within six months of the FNA.
Discussion
Through implementation of an ongoing quality assurance process, nearly 100% follow-up of abnormal pathological results was ensured, with appropriate and timely disposition of results. The results and outcomes compare favorably when contrasted with previously published studies, which have demonstrated only up to a 65% documentation rate of abnormal test results (4 –6). Furthermore, the authors are not aware of any previous studies evaluating the appropriate and timely disposition of abnormal results based on recommended treatment guidelines.
Several steps are recognized in the management of patient results, including clinician acknowledgement of the result, patient notification, and appropriate follow-up. Physicians spend a considerable amount of time with the formulation of plans and documenting disposition of test results (17). Yet, previous data suggest that the primary etiology of poor patient outcomes is failure in patient notification (7). This is particularly problematic when patient care requires multidisciplinary coordination, with no single individual tasked with ensuring adequate follow-up care (18). It was found that even at the initiation of the monitoring process, clinicians are quite efficient when it comes to notifying patients of pathology results, documenting communication, and ensuring adequate follow-up. With enhanced oversight, the physicians were able to optimize their patient care with little-to-no disruption in their daily practice.
It has been well-described that failure to follow up on abnormal results leads to missed diagnoses, poor patient outcomes, and increased risk of litigation to the physician. Up to 25% of missed follow-up cases result in delayed care, with 18% of missed cases leading directly to patient harm, as defined as causing pain, suffering, or adverse clinical consequences (19). Reasons for missed follow-up are multifactorial and often include several elements such as workplace design systems, individual physician practices, and organizational factors (9). The EMR cannot be solely responsible for alerting practitioners to abnormal test results, as it has been demonstrated that even among facilities using a common system, there is tremendous variability in follow-up (4). So-called sociotechnical factors (i.e., non-technical factors that affect workflow) have been shown to be critically important in the monitoring of results, yet can be very difficult to measure or act upon (20,21). This quality assurance program effectively neutralizes these factors without requiring a major overhaul of current system practices, and overcomes individual physician inertia and resistance to changing practices.
Implementation of a QI program based on guideline adherence can prove to be challenging, as guidelines are subject to change, and monitoring metrics must be adjusted as new guidelines emerge. The system described here has the benefit of being flexible, allowing for easy incorporation of changing classifications, guidelines, and technology, as demonstrated in 2010 with the enactment of the Bethesda criteria. With widespread implementation of these new criteria, it was possible to update the monitoring procedures and classifications successfully without disruption to the data-collection process. The standardization of terminology with the Bethesda criteria also allowed for non-physician reviewers to be involved in the monitoring process. This feature of this program is imperative for success, as medicine and healthcare continue to evolve.
Further evidence of the adaptability of the system is demonstrated by successful incorporation of recommendations regarding GEC testing into the algorithm. Through cytogenetic testing and early identification of benign nodules, the hope is that those patients subjected to unnecessary surgery will be limited (22), further improving patient care. An increase in the indeterminate nodules managed with “clinical evaluation” was noted in the later quarters of 2012 and first quarter of 2013. This pattern can likely be attributed to a number of physicians waiting for the introduction of GEC, which was seen in April 2013.
There are a number of limitations to the data and this system. It is not possible to capture documentation of treatment options and follow-up when patients choose to seek care at outside facilities or are managed outside of the Division of Endocrinology. These patients are at risk for loss to follow-up. The ability to monitor and track follow-up, using non-clinicians, is, in part, dependent on clarity and detail of physician documentation within the EMR. At times, word choice was difficult for a non-clinician reviewer to interpret, and physician review of individual charts was necessary.
Although the process was implemented at a large academic medical center, the basic principles of this program are easy to employ within smaller community facilities and in other procedural centers aside from thyroid nodule clinics. Many EMR systems include functionality for results tracking, which can be optimized to track communication of results and automatically programmed to have results return to the queue within a specified amount of time. A reviewer can then audit the queue as a failsafe backup to the EMR. The use of a non-physician reviewer minimizes cost concerns, and with a smaller patient population, the review process should be fairly efficient, with minimal time commitment on the part of the reviewer. For practices without this EMR function, appointment schedules can be used to identify patients, though they would need to be manually tracked, which may require greater resources.
Conclusion
A quality assurance system with a QI focus has been successfully developed to ensure that we remain up-to-date and current with guidelines. This system would be applicable to other procedural findings and clinical services to ensure patient safety and monitoring of follow-up for a variety of diagnoses and procedures. By engaging actively in the QI process, a clear message is sent to patients that their well-being is of upmost importance. It is hoped that this report encourages others to adopt a more standardized approach for minimizing medical errors, increasing compliance with published guidelines, and reducing patient morbidity.
Footnotes
Acknowledgments
We would like to thank Joanne Schulze for her work in developing the initial monitoring system and her recommendations for optimizing data collection. We would also like to thank Fred Milgrim for his assistance with data analysis.
Author Disclosure Statement
No competing financial interests exist.