
Abstract

Thursday, October 22, 2015
Thyroid & Development Thursday Oral Basic 3:40 PM
The thyroid develops independently of thyroid stimulating hormone (TSH). It is not until mid-gestation after organogenesis is finished that TSH contributes e.g. leading to fetal goiter in case of dyshormonogenic congenital hypothyroidism. Mechanisms that govern TSH-independent fetal thyroid growth are largely unknown. Sox9, a member of the SRY (sex-determining region Y)-related family of transcription factors, regulates fate determination and differentiation of cells from all three germ layers. Sox9 is required for pancreatic development of endocrine lineages from endoderm. In lung, interplaying with mesoderm-derived fibroblast growth factor 10 (Fgf10), Sox9 cell-autonomously promotes branching morphogenesis by controlling the balance between proliferation and differentiation. This led us to investigate a putative role of Sox9 in thyroid development.
Sox9 expression was investigated with immunofluorescence at different thyroid developmental stages (E9.5–18.5) of wildtype and Fgf10 KO embryos. Thyroid progenitors were identified with Nkx2.1. Cell proliferation was estimated with Ki67 staining. Fgf10 expressing cells were localized with in situ hybridization.
Nkx2.1+ thyroid progenitors ubiquitously co-expressed Sox9 from the bud stage onwards. As bi-lobation started at E13 Nkx2.1+/Sox9+ cells segregated in the distal tips of parenchymal cords conspicuous of a branching growth pattern (Fig. 1). Intriguingly, this coincided with the occurrence Ki67+ cells. Fgf1a0 KO embryos showed severe thyroid hypoplasia (<20% of wildtype size) with diminished branching growth during the lobulataion process. Sox9 expression sustained in Fgf10 KO thyroid precursor cells. Fgf10 was produced by stromal cells adjacent to branch endings.
These findings demonstrate a novel mechanism of embryonic thyroid growth reminiscent of a developmental program typical of branching organs with a ductal anatomy. Branching morphogenesis commences as the orthotopic thyroid gland is established after budding and descent of the primordium. In this process Sox9 likely works upstream of Fgf-mediated growth signals derived from surrounding mesenchyme. Conditional inactivation of Sox9flox in embryonic thyroid using Nkx2.1-Cre and Tg-Cre are in progress.

Branching pattern of growth in embryonic mouse thyroid. Cross-section of prospective right lobe at E14. Inset, with red light channel omitted, shows tip of branch indicated with arrow. th - thyroid; lc - laryngeal cartilage; me - mesenchyme.
Thyroid & Development Thursday Oral Basic 3:55 PM
Thyroid lineages are derived from mouse embryonic stem cells (mESCs) through brief BMP4/TGF-β signaling inhibition at the definitive endoderm stage leading to anterior foregut endoderm, followed by FGF2/BMP4 treatment. These cells are characterized by expression of Nkx2-1, a homeodomain transcription factor expressed in the developing lung, thyroid, and forebrain. Currently, little is known about the specification process and the yield of progenitors derived is low.
For this project, we utilized a mESC line double knock-in GFP-T/hCD4-Foxa2 with an inducible Nkx2-1 transgene, activated by addition of doxycycline (Tet-On).
Activation of the Nkx2-1 transgene for 24 hours at the anterior foregut endoderm (AFE) stage induces and maintains high levels of endogenous Nkx2-1 (up to 85% Nkx2-1+ cells) as well as thyroid-specific markers including Pax8 (up to 65% Nkx2-1+, Pax8+ cells), Tg, Foxe1, Hhex, Nis, and Tshr at later stages (day 22+) in our protocol. These cells can be cultured in three-dimensional culture, where they mature and organize into the distinctive follicle structure. Critical determinants of this thyroid lineage specification have been revealed by variations in developmental stage timing, signaling pathways, and sorting of subpopulations. Specifically, these experiments highlight a very narrow developmental time window of cellular competence to respond to exogenous Nkx2-1. They also show essential aspects including the derivation of anterior foregut endoderm populations with varied competence (marked and sorted by Foxa2 expression) and the necessity of dual FGF2/BMP4 signaling activation. To provide further insights into the mechanisms of this thyroid specification from AFE, we are analyzing RNA-Seq data sets acquired from relevant stages to identify potential targets of Nkx2-1 and changes in global gene expression.
The results demonstrate that Nkx2-1 can act as a stage-specific inductive signal during directed differentiation of mESCs to thyroid follicular cells. This method has provided novel insights into the thyroid specification process and exemplifies the potential of a more efficient system for deriving and studying thyroid cells, which can be used for in vitro modeling of development and disease.
Quantification of Nkx2-1+, Pax8+ populations at day 14 (post-overexpression of Nkx2-1) and day 30 immunostaining showing formation of follicle structures.

Thyroid Cancer Thursday Oral Translational 4:10 PM
Introduction Certain patients with papillary thyroid cancer (PTC) seem to be bound for a high PTC-specific mortality, but the genetic background is unclear. Our previous limited study suggested a unique role of coexisting BRAF V600E and TERT promoter mutations in PTC-related mortality, which remains to be firmly established in an extended large cohort.
Methods Correlative studies of BRAF V600E and TERT promoter mutations (chr5:1,295,228C>T and chr5:1,295,250C>T) and PTC-specific mortality in an expanded cohort of 1,051 patients (764 women and 287 men), aged 46 (interquartile range-IQR 36–57) years, with an extended follow-up time [median, 89 (IQR 48–142) months (7.4 years)].
Results On the entire PTC cohort analysis, coexisting BRAF V600E and TERT mutations were robustly associated with PTC-specific mortality, being 4/629 (0.6%) in patients with neither mutation, 7/292 (2.4%) in patients with BRAF V600E alone, 4/64 (6.3%) in patients with TERT mutation alone, and 15/66 (22.7%) in patients with both mutations, corresponding to deaths per 1000-person years (95% confidence interval-CI) of 0.80 (0.30–2.13), 3.08 (1.47–6.46), 6.62 (2.48–17.64), and 29.86 (18.00–49.52), respectively. Compared with patients harboring neither mutation, hazard ratios (95% CI) for mortality were 3.08 (0.87–10.84) with BRAF V600E alone, 8.18 (2.04–32.75) with TERT mutation alone, and 37.77 (12.50–114.09) with both mutations; the latter remained significant at 9.34 (95% CI 2.53–34.48) after adjustment for patient age and sex, tumor size, tumor multifocality, extrathyroidal invasion, vascular invasion, and cervical lymph node metastasis. Kaplan-Meier analyses revealed a modest decline in PTC-specific survival with either mutation alone but a sharp decline with coexisting mutations. There was a significant incremental effect of coexisting mutations over either mutation alone. Similar findings were made when only conventional-variant PTC or only the dominant TERT chr5:1,295,228C>T mutation was examined. No effect of the mutations on non-specific mortality was observed.
Conclusion We establish coexisting BRAF V600E and TERT promoter mutations as a powerful genetic background that robustly underpins the worst PTC-specific mortality.
Thyroid Cancer Thursday Oral Translational 4:25 PM
Papillary microcarcinoma of the thyroid gland (PMC) has a disease-specific mortality of <1% leading to suggestions that PMC may require no therapy. Yet the uncertainty of metastatic disease has led to relatively uniform management according to current guidelines. Thus rare cases of aggressive PMC may be “under-treated” with excessive morbidity at re-operation while the most patients with PMC may be “over-treated” risking unnecessary morbidity. Lacking are parameters to guide interventional management. To test the hypothesis that there are distinct molecular mechanisms underlying indolent and aggressive PMC, analysis of short noncoding (ncRNA) profiles was performed.
Comparative ncRNA analysis (Affymetrix GeneChip® miRNA 4.0 Array) was performed on RNA extracted from 17 cases of PMC (<45 y/o cohort: 7 cases - 3 indolent PMC, 4 aggressive PMC) (≥45 y/o cohort: 10 cases - 5 indolent, 5 aggressive). Bioinformatics analyses included multivariate Principal Component Analysis to identify sample-based differential expression and univariate linear modeling of sample groups to detect gene-based differential expression.
In indolent primary tumors (T), 18 ncRNAs are significantly altered compared with matched normal tissue (N); 34 ncRNAs are altered in aggressive primary tumors (AT) compared with normal (AN). Of those 52 ncRNAs, 9 are unique to T and 25 unique to AT (Panel A). Direct comparison of miR profiles in AT versus T revealed 12 miRs significantly altered which target 622 mRNAs associated with tumorigenesis. These include miR-16-5p, miR-1991-3p, miR-96-5p whose targets include MAPK, RAS, PI3K, WNT and pluripotency transcription factors including NANOG. Analysis of aggressive tumors revealed distinct profiles of AN vs AT vs AM. Of note, in AM (Panel B), 410 ncRNAs are significantly altered compared with the AT primary site indicating a distinct molecular profile in the metastatic site.
These findings reveal distinct molecular profiles characterizing indolent and aggressive PMCs which may provide the framework to aid in diagnosis and therapeutic interventions. Additional investigation of the molecular biology of PMC is needed to understand the differential behavior of this histologic entity.

Thyroid & Development Thursday Oral Clinical 4:40 PM
Suboptimal thyroid function in pregnancy is associated with adverse obstetric outcomes. However it is unclear whether levothyroxine treatment during pregnancy improves outcomes. We present a detailed analysis of obstetric outcomes in participants of the Controlled Antenatal Thyroid Screening (CATS) study
We utilized Welsh participants of the CATS study where women with TSH in the highest 2.5% and/or FT4 in the lowest 2.5% were randomized to receive levothyroxine or not between 11–16 weeks gestation. We obtained data on stillbirths, birth-weight and gestational age at delivery using the Secure Anonymised Information Linkage databank. 92% of participants were matched successfully (N = 14,332), comprising women with normal thyroid function (n = 13,659), untreated women with abnormal thyroid function (n = 361) and levothyroxine treated women with abnormal thyroid function (n = 312). We explored whether women with abnormal thyroid function had increased odds of adverse outcomes and whether treatment influenced this. Multivariate logistic regression was performed with analyses adjusted for maternal age, maternal weight, smoking status, parity and year of birth.
Stillbirths (in utero demise after 24 weeks gestation) occurred more frequently in untreated women with a high TSH than in women with normal thyroid function OR = 4.54 (95%CI 1.07, 19.2) p = 0.04. No stillbirths occurred in women receiving levothyroxine. Abnormal thyroid function was not associated with increased odds of small for gestational age or pre-term delivery. However low FT4 was associated with macrosomia OR = 1.46 (95%CI 1.03, 2.08) p = 0.04, although levothyroxine treatment did not appear to substantially alter this. Analysis in women with abnormal thyroid function showed that levothyroxine treated women had offspring with higher birth weight 3540g
Our results show that abnormal maternal thyroid function is associated with adverse outcomes. Levothyroxine treatment is associated with favourable effects on birth-weight and gestational age at delivery and may have some protective impact on stillbirths.
Thyroid Nodules & Goiter Thursday Oral Basic 4:55 PM
Autonomous thyroid adenomas (ATAs) are a frequent cause of hyperthyroidism. Genetic mutations in the genes coding for the TSH receptor (TSHR) or the Gs protein alpha subunit (GNAS) are found in approximately 60% of these tumors. The involvement of other pathways and the genetic alterations responsible for the remaining cases are presently unknown. Aim of this study was to obtain a comprehensive genetic characterization of ATAs and identify novel genes and pathways involved in thyroid tumorigenesis.
Whole exome sequencing in 19 ATAs and paired normal DNA samples, followed by candidate gene validation in a large cohort of thyroid samples (Total 304, of which 123 ATAs, 59 normal surrounding tissues of ATAs, 82 cold thyroid nodules, 16 follicular thyroid carcinomas and 24 papillary thyroid carcinomas) and functional characterization in vitro and in intact cells.
A total of 94 candidate somatic mutations were detected in the 19 ATAs with a median of 4 mutations per sample. A recurrent, hot-spot mutation in the enhancer of zeste homolog 1 (EZH1) gene (c.1712 A>G; p. Gln571Arg), which codes for the catalytic subunit of a non-canonical Polycomb repressive complex 2, was found in 4 tumors (21% of cases). Targeted screening in an independent cohort conformed a high frequency (27%) of this EZH1 mutation in ATAs. EZH1 mutations were strongly associated with known (TSHR, GNAS) or presumed (ADCY9) alterations in genes of the cAMP pathway. Functional studies revealed that the identified hot-spot mutation in EZH1 caused an increased tri-methylation of histone H3 as well as an increased proliferation of thyroid cells.
Our study reveals a hot spot mutation in EZH1 as the second most frequent genetic alteration in ATAs. The association between EZH1 and other mutations of the cAMP pathway suggests a two-hit model of the pathogenesis of these tumors, where constitutive activation of the cAMP pathway and EZH1 mutations might cooperate to induce deranged hormone production and proliferation of thyroid cells.
Thyroid & Development Thursday Oral Basic 5:15 PM
Congenital-hypothyroidism (CH) is the most common congenital endocrine disorder mainly due to thyroid dysgenesis. FoxE1 is a transcription factor required for survival of thyroid cells precursors and subsequent migration of the thyroid primordium to its final position. FoxE1 null mice have no thyroid gland or an atrophic sublingual thyroid and animals die at birth. In human, rare mutations found in FoxE1 results in CH due to athyreosis.
To understand the role of FoxE1 in thyroid development and its function in thyroid physiology in adult, we generated FoxE1-null mouse embryonic stem cells (mESC) lines with TALENs. Those edited cells where then engaged in a protocol of In vitro differentiation allowing the generation of functional thyroid follicles from mESC cells.
Thyroid follicles were obtained from FoxE1-null cells but the number was reduced compared to WT. IF and qPCr analysis showed an accumulation of Thyroglobulin but NIS expression appeared severely decreased and TPO and TSHR not detectable. A barely detectable iodine accumulation compared to WT and absence of organification were observed when the cells were exposed to I125. Because TSHR is regulating thyroid morphogenesis and NIS expression via activation of the cAMP pathway, we substituted TSH by a cAMP analogue (8-Br-cAMP) to compensate for the absence of TSHR. The results showed that thyroid maturation was not recovered by cAMP treatment.
Those results suggest that FoxE1 is required to generate fully differentiated thyroid cells or for maintenance of thyroid differentiation in mature cells. A transcriptome analysis will be performed to identify genes controlled by FoxE1 in this process. In addition our approach validates our In vitro model of thyroid differentiation for future studies aiming to functionally characterize new genes found mutated in patients with CH.
Thyroid Hormone Metabolism & Regulation Thursday Oral Basic 5:21 PM
Thyroid hormone signaling in the brain is mediated by T3 entering directly from the circulation and by T3 that is produced in astrocytes via the type-2 deiodinase (D2)-mediated T4-to-T3 conversion.
To find out the significance of locally produced T3 in the brain, mice with astrocyte-specific D2 inactivation (Astro-D2KO; flox-D2 x GFAP-cre), which lack 90–95% D2 activity in cerebral cortex (CC) and 70–90% in hippocampus (HC), were tested.
The HC of Astro-D2KO animals was the brain region most affected by Dio2 disruption given that genes upregulated by T3 were significantly decreased in Astro-D2KO mice, such as MBP (∼43%), Mag (∼34%), Hr (∼49%) and Aldh1a1 (∼61%), and genes repressed by T3 were enhanced such as Col6a1 (∼200%), Syce2 (∼26%) and Dgkg (∼17%). Notably, the expression of five depression-related genes was decreased, i.e. Dhdds (∼11%), Bdnf (∼18%), Nt-3 (∼43%), Vegf (∼14%) and Nmdar (∼26%), and C-Fos was increased by ∼58% when compared to Ctrl mice. Astro-D2KO animals travelled ∼27% less and exhibited ∼34% less rearing behavior when monitored continuously for 7 days. While no differences in mobility were observed in the open field, the Astro-D2KO animals spent ∼15% more time in the closed arms of the elevated plus maze, ∼120% more time in freezing behavior and exhibited ∼42% less head-dips. They also showed ∼37% greater immobility time during tail suspension and ∼40% in forced swim test (40–42%). These results indicate that absence of D2 in the brain promotes mood-disorders that resemble anxiety-depressive-like behavior.
These findings demonstrate the critical role played by D2 in thyroid hormone signaling in the brain, and recognize defects in the D2 pathway as a potential risk factor for development of mood disorders.
Thyroid & Development Thursday Oral Basic 5:27 PM
The differentiation program for human thyroid follicular cells (TFCs) relies on the interplay between sequence-specific transcription factors and transcriptional co-regulators. TAZ (transcriptional co-activator with PDZ-binding motif) is a co-activator that regulates several transcription factors including PAX8 and NKX2-1 (TTF1) which play a central role in thyroid-specific gene transcription. Both TAZ and PAX8/NKX2-1 are co-expressed in the nuclei of thyroid cells and TAZ interacts directly with both PAX8 and NKX2-1 leading to their enhanced transcriptional activity on the thyroglobulin (TG) promoter.
We now report the use of a newly identified TAZ activator, ethacridine, in the simple and direct induction of differentiation of thyroid cells from human embryonic stem (hES) cells. As previously, we first derived endoderm by activin A exposure of hES cells (line H9) followed by induction of differentiation into thyroid epithelium directed by ethacridine and thyrotropin (TSH) over ∼21 days.
The expression of TAZ was increased by ethacridine, in the activin A derived and confirmed endoderm, in a dose-dependent manner. Further analyses of these cells, for PAX8 and NKX2-1 mRNA by real time PCR, and for protein expression by direct immunostaining, showed upregulation of these dormant, endogenous, transcription factors in the hES cells. When followed further with exposure to TSH the thyroid specific genes - TG, TSHR and NIS - were induced in these differentiated hES cells.
These data show that ethacridine, a TAZ activator, induced thyroid-specific gene expression and promoted thyroid cell differentiation from hES cells allowing the development of a simple technique for thyroid cell production in vitro.
Thyroid Cancer Thursday Oral Translational 5:33 PM
The interaction between Programmed death 1 (PD-1), a T cell co-inhibitory receptor, with the Programmed death ligand 1 (PD-L1), is a widely studied immune target in cancer. Monoclonal antibodies blocking these molecules have had recent phenomenal success. Little is known about these in thyroid cancer.
We compared RNA and protein expression of PD-L1 at baseline and during treatment with IFNγ, BRAF inhibitor (BRAFi) PLX4720, or MEK inhibitor (MEKi) PD03250901 in a panel of thyroid cancer cell lines. In vivo validation was performed in a novel immunocompetent orthotropic mouse model of anaplastic thyroid cancer (ATC). One week after tumor implantation with murine BRAFV600E ATC cells, 24 B6129SF1/J mice were randomized to treatment with either control, PLX4720, anti PD-L1 antibody (Ab.), or a combination of PLX4720 and anti PD-L1 Ab. On day 14 mice were euthanized and tissue processed.
BRAFV600E cells showed a significantly higher baseline expression of PD-L1 at mRNA and protein levels compared to BRAFWT cells (median Log2 fold 3.39 ± 0.6 vs. -0.87 ± 2.4, P < 0.05). MEKi treatment resulted in a decrease of PD-L1 expression across all cell lines while BRAFi treatment decreased PD-L1 expression in BRAFV600E cells, and paradoxically increased its expression in BRAFWT cells. In our immunocompetent model of aggressive thyroid cancer, control tumor volume reached 782.3 ± 174.6mm3 at two weeks. Combinations of PLX4720 and anti PD-L1 Ab. dramatically reduced tumor volume to 147.3 ± 60.8, which was much better than PLX4720 (439.3 ± 188.4 mm3, P < 0.001) or anti PDL-1 Ab. (716.7 ± 62.1, P ≤ 0.05) alone. Combination treatment resulted in intense CD8+ T lymphocyte infiltration into the tumor, along with higher expression of T cell exhaustion markers.
PD-L1 is over expressed in BRAFV600E tumors and its expression is associated with MAPkinase activity. Anti PD-L1 treatment potentiates the effect of BRAFi on tumor regression and results in intensified anti tumor immune response in an immunocompetent model of ATC.
Thyroid Cancer Thursday Oral Clinical 5:39 PM
Management of anaplastic thyroid cancer (ATC) is difficult due to aggressiveness and resistance to therapeutic efforts. The median survival is reported less than half-a-year. The standardized effective chemotherapeutic strategy has not yet been settled, because of the lack in reliable objective information. We conducted a nation-wide clinical study.
A prospective multicenter, non-randomized, open label, single-arm, study to investigate the feasibility, safeness, and efficacy of weekly paclitaxel administration (80mg/m2 once an week) for patients with pathologically confirmed ATC (UMIN 000008574) was conducted with enrollment of 71 patients from 14 institutes. The primary end points to investigate were feasibility, as well as response rate in patients having evaluable lesion.
Fifty-six patients (M:F = 16:40, median 71.3 (47–84) years-old, stage IVA:B:C:X = 10:18:24:4) were eligible for analysis. Up to 23 (median 2) cycles of treatment was undergone. AEs more than grade 3 were found in 28.6% of the patients. There was no severe AE, nor treatment related death. Forty-three patients died of disease, one died of an accident, one was lost, and 11 still alive at the time of data cut-off. Median overall survival (OS) was estimated as 227 (95% CI: 148.2 to 305.8) days in all. The efficacy was able to be evaluated in 39 patients. CR, PR, SD and PD were observed in 0, 9, 22 and 8 patients. The objective response rate, and the clinical benefit rate were 23.1 and 79.5%, respectively. Fourteen patients underwent surgical removal of the primary lesion after chemotherapy, resulted in 9 complete- and 5 incomplete resections, respectively. These patients survived from 112 to 788 (median 365) days.
We have demonstrated an objective outcome of standardized chemotherapeutic treatment in patients with ATC for the first time in the world. Although the probability of response seemed fur from satisfactory, weekly paclitaxel could be a feasible standardized chemotherapeutic regimen for ATC at present. Possible application in combination with surgery was suggested.
Thyroid Cancer Thursday Oral Translational 5:45 PM
Recent studies have shown that a significant part of the genome is transcribed into the class of long non-coding RNAs (LncRNAs) and that LncRNAs have important functions in cancer initiation and or progression. There has been, however, no comprehensive analysis of LncRNAs in thyroid neoplasms. The aim of this study was to provide a comprehensive analysis of LncRNA expression profile in normal, benign (FA, HCA) and malignant thyroid neoplasms (PTC, FTC, HCC, ATC); and to determine the biological role of differentially expressed LncRNAs in thyroid cancer.
Using LncRNA PCR expression profile arrays, we found 3 LncRNA (p < 0.05) to be upregulated and 2 LncRNAs (p < 0.05) to be downregulated in thyroid cancer compared to benign and normal thyroid tissue. 13 LncRNAs were found to have higher expression levels (p < 0.05) in ATC. We validated the most differently expressed LncRNA in an independent cohort of 13 normal, 23 PTC, 7 TC-PTC, 14 PDTC and 8 ATC samples. The roles of identified LncRNA in thyroid cancer were studied in different thyroid cancer cell lines using protein and PCR arrays, RT-PCR, western blot, cell motility and cell cycle assays.
Among these LncRNAs, LUCAT-1 was found to be significantly upregulated in thyroid cancer (p = 0.0004). LUCAT-1 silencing reduced cellular proliferation and resulted in G1/S cell cycle arrest, while inducing apoptosis and decreased cellular invasion and migration in thyroid cancer cell lines. Given these functional effects of LUCAT-1 in thyroid cancer cells, we next determined if LUCAT-1 modulates the expression of epithelial-to-mesenchymal transition (EMT) regulatory genes and whether it alters phospho-kinase signaling pathways, commonly altered in thyroid cancer, using an EMT and phosphor-kinase arrays, respectively. We found that LUCAT-1 knockdown downregulated CaV2 mRNA expression and that CaV2 was upregulated in human thyroid cancer samples (p < 0.0001). Moreover, LUCAT-1 knockdown also reduced P-p38 levels in thyroid cancer cell lines.
Our results show that Lnc-RNAs are dysregulated in thyroid cancer and that LUCAT-1 may regulate thyroid cancer initiation and/ or progression.
Autoimmunity Thursday Oral Translational 5:51 PM
Thyroid associated orbitopathy (TAO) is a complex and debilitating autoimmune inflammatory disorder. While the exact pathophysiology remains elusive, orbital fibroblasts have been implicated to play a key role in the underlying inflammatory process. Prior studies have shown that prostaglandin analogues (PAs) inhibit adipogenesis in normal human orbital fibroblasts; however, there is limited data on their effects on adipogenesis in TAO. Herein, we sought to investigate the anti-adipogenic effects of the PA bimatoprost in orbital fibroblasts from patients with TAO. Orbital adipose samples were obtained from TAO patients (n = 6) and normal controls (n = 6). Orbital fibroblasts were then selectively cultured from each sample. During differentiation, cultures were exposed to bimatoprost or left untreated. Cell lines were then snap frozen and harvested at days 7 and 14 for gene expression analysis by real-time reverse transcription polymerase chain reaction (RT-PCR). Expression levels of thyrotropin receptor (TSHr), peroxisome proliferator-activated receptor gamma (PPARγ), CCAAT-enhancer binding protein α (C/EBPα), and lipoprotein lipase (LPL) were analyzed to evaluate the effects of treatment on adipogenesis.
Histologically, treatment with bimatoprost inhibited adipocyte differentiation with treated cells retaining their fibroblastic morphology with decreased intracellular lipid accumulation. These anti-adipogenic effects were confirmed on a genetic level by our RT-PCR results, which showed a significant decrease in the expression levels of TSHr (p = 0.002), C/EBPα (p = 0.003), and LPL (p < 0.001) in treated samples. Treatment also decreased PPARγ expression, but not to a statistically significant degree (p = 0.054). The effect of bimatoprost treatment did not differ between TAO and control samples (p > 0.05), nor did it change over time from day 7 to 14 (p > 0.05).
The results of our study demonstrate that bimatoprost treatment inhibits adipogenesis in TAO-derived orbital fibroblasts, suggesting a potential role for bimatoprost as a promising new therapeutic agent in the management of TAO.

The effects of bimatoprost treatment on the expression levels of adipogenesis associated genes as determined by real-time reverse transcription polymerase chain reaction (RT-PCR). Data presented as average normalized expression relative to a housekeeping gene. Statistically significant differences between treated and untreated samples as indicated by p-values. LPL, lipoprotein lipase. C/EBPα, CCAAT-enhancer binding protein α. PPARγ, peroxisome proliferator-activated receptor gamma. TSHr, thyroptropin receptor.
Withdrawn
Monday, October 19–Tuesday, October 20, 2015
Autoimmunity Monday & Tuesday Short Call Posters Clinical
Graves' disease (GD) is caused by thyroid stimulating autoantibodies (TSI) targeting the thyrotropin receptor (TSHR). The novel chimeric TRAb assay, which directly measures these autoantibodies by double epitope recognition (sTRAb; Horm Metab Res. 2015 Jun 16), was evaluated via comparison with the stimulatory index (SI) of a bioassay (bTRAb; ITC Paris 2010, P-0020) and serum T4 and for its clinical significance.
In the sTRAb assay a human chimeric TSHR fixed to microtiter plates binds one arm of the sTRAb. The second arm bridges to a human TSHR (aa 21–261) fused with secretory alkaline phosphatase (SEAP) for chemiluminescence. In bTRAb assay using wildtype TSHR cAMP stimulation was measured as SI by SEAP /CRE reporter gene construct. Also TRAb (TRAK human assay, Brahms) and total T4 assay (Ortho clinical diagnostics) were tested. Relations between continuous values were quantified with linear regression analysis of log-transformed values.
Correlation studies: Untreated GD patients: sTRAb titers vs. bTRAb SI: n = 32, r = 0,66, p < 0,0001; sTRAb titers vs. serum T4: n = 47, r = 0,77, p < 0,0001; bTRAb SI vs. serum T4 (n = 32, r = 0,38, p < 0,03). Treated GD patients: sTRAb titers vs. bTRAb SI values (r = 0,71, p < 0,001). Features in special cases: Positive TRAb values persisted in 3 GD cases in remission in contrast to negative sTRAb values (present among 37 cases: 8%). In 3 hypothyroid patients presented during usual transfer practice (PDUTP) of 468 GD patients (0.62%) to thyroid clinics sera were positive in the TRAb assay, whereas autoantibodies were not detected by the sTRAb assay. One euthyroid subject (PDUTP of 252 GD patients: 0,4%) was TRAK positive (22 IU/L) but sTRAb and bTRAb negative. sTRAb titers further differentiate between GD and GD with active and inactive endocrine orbitopathy (EO): medians±SD: n = 150, 2,96 ± 9,37; n = 24, 22,77 ± 15,46 and n = 77, 6,6 ± 15,23 IU/L, p < 1e-5. The chimeric sTRAb assay, introducing Bridge technology, measures TSI evidenced by bTRAb SI and thyroid secretion product serum T4 levels. It delivers high diagnostic accuracy for GD, may clarify special cases and assist in monitoring EO.
Autoimmunity Monday & Tuesday Short Call Posters Clinical
Thyroid autoimmune disease is associated with reproductive challenges. Screening for thyroid dysfunction is recommended before initiating fertility treatment. The mechanisms behind this association are still unclear.
Baseline data from 547 women referred to fertility treatment in a hospital clinic from Sep 2011 to Oct 2013. On cycle day 2–5, prior to stimulation, antral follicle count (AFC), anti-Müllerian Hormone (AMH), FSH, LH, TSH, thyroxine (T4), free-T4, and thyroid peroxidase autoantibodies (TPOAbs) were assessed. TPOAb-levels were measured with Kryptor immunoflourescent assay (BRAHMS, Hennigsdorf, Germany; functional sensitivity 50 U/mL, TPOAb-positivity if TPOAbs ≥60 U/mL). Laboratory TSH-reference range: 0.4–4.0 mIU/L. Linear or binary logistic regression analyses were applied as appropriate with covariates: Age, AFC, cycle length, and FSH.
Of the 547 women, 56 (10.2%) had TPOAbs >60 U/mL and 31 (5.7%) had TSH >4.0 mIU/L; among these women L-T4 had been started before admission in 19 (23.2%) and 22 (26.8%) were previously diagnosed with thyroid disease. Mean age(SD) was 32.8(4.0) years. Low AMH-levels (<5 pmol/l) were significantly associated with higher TSH-levels (p = 0.03), higher age (p < 0.00), higher FSH-levels (p < 0.00), lower AFC (p < 0.00), and shorter menstrual cycle (p = 0.02). TSH remained significantly associated with low AMH-levels in adjusted analyses (p = 0.02, aOR = 1.03 95%CI: 1.0–3.3). Adjusting for age, TPOAb-positivity was predictive of higher AMH-levels (p = 0.01, B = 1.3 95%CI: 1.1–1.7). These results could indicate that while high TSH-levels may affect ovarian function directly, infertility in TPOAb-positive women could be due to a general autoimmunity affecting both thyroid and reproductive organs, rather than a low egg reserve.
Only 26.8% of women with TPOAbs or TSH-levels >4mIU/L had a previous diagnosis of thyroid disease. High TSH-levels were associated with low AMH-levels, while TPOAb-positive infertile women had higher AMH-levels. Our results illustrate the importance of thyroid screening in infertility treatment to elucidate possible mechanisms behind the individual cause of infertility and to target treatment strategies.

Disorders of Thyroid Function Monday & Tuesday Short Call Posters
Myxedema coma (MC) in childhood is primarily a relic to a time predating widespread availability of thyroid-stimulating hormone (TSH) assays and universal newborn screening. Optimal MC treatment is controversial and scarcely described in pediatrics. We report a boy with congenital hypopituitarism who presented in hypotensive shock refractory to stress doses of corticosteroids.
Case report
A 14-year old cognitively delayed boy with congenital hypopituitarism (GH, ACTH, TSH, LH/FSH deficiencies), presented to the Emergency Department (ED) after being found unresponsive and hypoglycemic (BG 37mg/dL). In the ED, he was obtunded, hypothermic (96.7deg F), bradycardic (50bpm), hypotensive (88/48 mm Hg), and tachypneic (24bpm). He was given aggressive hydration and two 100mg doses of Hydrocortisone, followed by a Hydrocortisone infusion, and then Epinephrine and Dopamine. His initial evaluation revealed hyponatemia (133mmol/L), hypokalemia (3.3mmol/L), and leukopenia (WBC 3.4 m/uL). Over the next 2 days, pulse was 45–82 bpm and blood pressure 69–143/38–92. Further results suggested chronic under-treatment with rGH and Levothyroxine (Free T4 0.31ng/dL, TSH 0.83ng/dL, IGF-1 < 16 ng/mL). On the 3rd day, MC treatment was initiated: Levothyroxine was raised to 200 mcg IV daily, in conjunction with 5mcg loading dose of Liothyronine followed by 2.5 mcg every 8 hourly for 2 days. In the following 24 hours, he became alert and interactive, and vasopressors were stopped. His mother had a recent social crisis resulting in economic deprivation and social isolation, and despite past meticulous care she had stopped giving his medications.
We report a pediatric patient with hypopituitarism who presented in hypotensive shock refractory to stress dosed corticosteroids; he remained in critical condition until high dose thyroid hormone replacement was implemented. This case demonstrated that MC must be considered, even in pediatric patients, particularly in the context of refractory adrenal crisis in patients with known or possible co-existent hypothyroidism. Treatment recommendations in pediatrics are limited, and so it is critical to report cases such that colleagues may glean from the rationales, treatment approaches and outcomes.
Disorders of Thyroid Function Monday & Tuesday Short Call Posters Clinical
Previous study found that thyrotropin levels were increased in gestational diabetes mellitus (GDM) suggesting its close relationship with hypothyroidism during pregnancy (HDP). The combined effects of GDM and HDP on pregnancy outcomes have not been fully studied.
We recruited a large maternal and neonatal cohort from 71,757 pregnant women from 2008 to 2014 from Nanjing Maternity and Child Health Care Hospital Affiliated to Nanjing Medical University. Pregnant women without GDM and HDP were set as controls. We studied the prevalence of isolated GDM, isolated HDP, and GDP combined with HDP. The pregnancy outcomes in these groups were compared.
The overall prevalence of hypothyroidism was 1.2%, while the prevalence of GDM was 11.9%. The prevalence of both diseases increased gradually from 2008 to 2014. Notably, the prevalence of GDM and HDP were all higher in elderly primipara than in primipara with normal age (2.9% vs. 1.1%, 22.2% vs. 11.4%). The bodyweight of the neonates was lower in HDP group as compared to controls (3275.8 ± 493.0g vs. 3328.76 ± 484.1g), while GDM group had higher bodyweight (3346.4 ± 520.5g). Growth retardation was seen more often in HDP group compared to controls (3.7% vs. 0.9%). The prevalence of macrosomia was higher in GDM group compared to controls (8.6% vs. 6.9%). The birth weight in GDM combined with HDP was similar to any other group. The prevalence of postpartum bleeding was similar in HDP, GDM and HDP combined with GDM, all higher than controls. The prevalence of postpartum infection was 3.6% in GDM groups higher than the other three groups. The prevalence of abnormal development and stillbirth was higher in GDM combined HDP than the other three groups (1.1% vs. 0.1–0.3%, P = 0.035; 1.1% vs. 0.1–0.2%, P = 0.021).
The prevalence of HDP and GDM increased in recent years, especially in elderly primipara. There were higher prevalence of fetus development abnormality and stillbirth in groups with HDP combined with GDM. So close follow-up of these patients and prevention of HDP and strict glycemic control might decease abnormal pregnancy outcome in these high risk patients.
Disorders of Thyroid Function Monday & Tuesday Short Call Posters Clinical
Subclinical hypothyroidism is a common subclinical endocrine disease, given the prevalence in the general population in various countries is 4% to 10% in reported, the current diagnosis is based on elevated serum thyroid stimulating hormone (Thyrotropin, TSH) levels and normal serum FT4. Adverse consequences of subclinical hypothyroidism is that it leading clinical harm cause hypothyroidism and promote ischemic heart disease, Therefore, accurate serological examination for clinical diagnosis and therapy is very important. The main purpose of our study is to estimate the difference in results detected with subclinical hypothyroidism serum by four clinical routine TSH immunoassays, and impact on clinical diagnosis and treatment.
To take laboratory Roche Cobase6000 test results as a reference, selected 105 serum samples included patients with subclinical hypothyroidism. Used Roche Cobase6000, Siemens Immulite2000, Siemens ADVIA Centaur XP and Abbott I2000 automatic biochemical analyzer to measure TSH concentrations of the 105 serum samples at same time.
The results showed that individual serum TSH level varied significantly from one assay to another (P < 0.05). The correlation between Roche Cobase6000 and Immulite2000, ADVIA Centaur XP, Abbott I2000 respectively were relatively low (r ranged from 0.48 to 0.49), Pairwise correlation of TSH levels got from the remaining three assay were higher (r of 0.86 ∼ 0.93), However values of the difference among the four automatic immunoassays range from -14% to 44% ; 93 cases of the sample detected by Cobase6000 were positive, with the other three Ways test results were positive for only 4, 16 and 23 cases respectively, Significant differences existed in the french part of the four detection for clinical diagnosis.
The results of different automatic immunoassay analyzers in patients with subclinical hypothyroidism varied widely, physicians and manufacturers need to recognize these differences, it is still a difficult and challenge task for laboratory community to establish standardization of reference system to achieve comparability of measurement results between methods.
Disorders of Thyroid Function Monday & Tuesday Short Call Posters Clinical
Hypothyroidism is usually treated with once daily levothyroxine which restores euthyroidism in most cases. However, a minority of patients remains hypothyroid despite adequate replacement. In this cohort of poor responder's non-compliance with levothyroxine is the most common cause for failure to attain clinical and biochemical euthyroidism. In this study we looked into the effectiveness of once or twice weekly levothyroxine treatment on thyroid function tests (TFT's) in patients who remained hypothyroid due to poor compliance with once daily levothyroxine.
A retrospective review of case notes and biochemical results of hypothyroid patients who were on supervised once or twice weekly oral levothyroxine treatment for the period of 3 years (March 2009 to September 2012). Wilcoxon matched-pairs sign rank test was used to compare TSH levels over time.
13 hypothyroid patients who were non compliant with once daily levothyroxine treatment were given once/twice weekly-supervised levothyroxine in the endocrinology department. Initially, daily requirement of levothyroxine in 6 patients was <150 microgram and seven patients had a requirement of >150 microgram. Eleven patients were commenced on a twice weekly regime with doses ranging from 400–1200 microgram and 2 patients were on once weekly regime with the dose range of 300–700 microgram. Five patients (38.5%) were on medications which could potentially interfere with the absorption of levothyroxine. Coeliac screen was positive in one patient. Every patient tolerated the regimes well. Median TSH on standard levothyroxine replacement was 40.6 mU/l (IQR 20.6 - 100 mU/l) at 3–6 months this was lower 2.89 mu/l (IQR 0.46- 8.38 mu/l) p = 0.002 and was still lower at 12 months TSH 4.98 mu/l (IQR 0.1–17.9 mU/l) p = 0.008. Similar improvements were seen for FT4.
Our study shows that supervised once or twice weekly oral levothyroxine is a safe and well-tolerated treatment strategy to normalize TFT's and achieves biochemical euthyroidism with improved clinical outcome in patients who have been non-compliant with their medications. Further studies with large number of patients and longer duration of follow up are required to clarify the long term outcome of this strategy.
Disorders of Thyroid Function Monday & Tuesday Short Call Posters Clinical
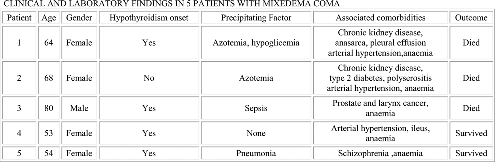
Myxedema coma (MC) is a severe life threatening condition of decompensated hypothyroidism, associated with a high mortality. Intravenous (IV) thyroid replacement (TR) should be initiated as early as possible, however IV Levothyroxine (LT4) is not available in many developing countries, so oral LT4 is use as an alternative treatment. We report five patients treated with high dose of oral LT4.
Clinical charts of five patients with MC were reviewed.
Cases reports: Five patients with MC diagnosed based on altered sensorium, hypothermia, a precipitating illness, and thyroid hormone tests. Age ranged from 53 to 80 years old. Four of them were onset of primary hypothyroidism. Infection was present in two patients. TSH ranged from 87 to 204 mU/L (NR:0.3–5) and free T4 from indetectable to 0.3 ng/dl (NR 0.8–1.8). All patients received stress dose of hydrocortisone followed by 300 μg every 8 hours of oral LT4 as initial loading dose; maintenance dose ranged from 100 to 300 μg per day. Supraventricular tachycardia was evidenced as complication in one patient. Outcome was fatal in three of them. Survivors were younger than non-survivors (see table).
Discussion: The main considerations with TR in MC are the absorption and distribution of TR preparation, the onset of action, efficacy, and safety. It remains uncertain whether it should be as T4, T3, or both. Usually parenteral T4 is recommended in 300–500 μg as initial dose1, but a single dose of 500–800 μg serves to replete the peripheral hormone pool 2. We use a high dose of oral of LT4 because of mixedema ileus interferes and delays absortion of LT4 in MC. Conclusion: Alternative treatment scheme may be high dose of oral LT4 as loading dose when parenteral LT4 is unavailable. Mortality was similar than other reports. Bibliography 1. Vivek Mathew, et al. Journal of Thyroid Research 2011;2011;2011:493462. doi: 10.4061/2011/493462. Epub 2011 Sep 15 2. Brent GA, et al. Williams textbook of Endocrinology 2009, 11th ed, p 41.
Iodine Uptake & Metabolism Monday & Tuesday Short Call Posters Clinical
Iodination of table salt is mandatory in Brazil. Over the past decades, several adjustments have been made to the iodine concentration in table salt in the country in an attempt to prevent the diseases that result from inadequate intake of this nutrient. However, a study in 2003 showeding an excessive iodine intake in schoolchildren in the state of São Paulo-Brazil, with an average urinary iodine concentration >400 mcg/L (normal 100–299 mcg/L). Following the results of this study, resulted in a decrease in the iodine concentration in table salt was decreased from 40–100 to 20–60 mg/kg. The aim of the currentis study was to determine the current iodine nutritional status in the metropolitan area of São Paulo-Brazil. The thyroglobulin (TG) is a protein synthesized exclusively by the thyroid and a biological marker of the gland's function over weeks or months. Due to that, TG levels have been recently used as a reliable indication of iodine intake in population studies. Levels of TG are increased in circumstances of both deficient and excessive iodine intake. The urinary iodine concentration, in turn, reflects the intake of iodine over the previous 24 hours. To be considered iodine sufficient, a population must have a median TG level below 13 ng/mL.
We evaluated the iodine nutritional status of 202 children between the ages of 7–14 years, measuring the urinary iodine concentration in a spot urine sample (Sandell-kolthoff, modified by Pino et al) and serum TG level (chemiluminescence - immulite 2000, Siemens)
The median urinary iodine concentration was 170 mcg/L (range 100–200 mcg/L) and the median TG concentration was 12.8 ng/mL (range 0.5–63.6 ng/mL).
These results reflecting a proper iodine nutritional status in the studied population. Considering the optimal iodine nutritional status in our sample, what will be the impact of the reduction in iodine concentration in table salt (from 20–60 mg/kg to 15–45 mg/kg) implemented after we collected our data, particularly in high-risk populations?
Iodine Uptake & Metabolism Monday & Tuesday Short Call Posters
Turkey has mild endemic iodide deficiency. Adequate iodine intake is important during pregnancy and early life as it is a component of the thyroid hormones, thyroxine and triiodothyronine, crucial for fetal brain and neurological development. It is still not known does the combination of low iodine intake, thiocyanate exposure from smoke, nitrate and relatively low levels of perchlorate exposure in the environment cause a decreased iodide transport in both thyroid and lactating breast and possibly lead to reduced thyroid function, hypothyroidism and impaired mental and physical development of offspring.
Thyroid status was measured in lactating women and neonate postpartum. Maternal urinary perchlorate, thiocyanate, nitrate, iodide levels, serum TSH, FT3, FT4, Anti-TPO, Anti-TG and newborn TSH (heel prick test) measured.
The median and IQR for TSH, FT4, F T3 and, urinary perchlorate were 2.07 (1.32–2.98), 4.3 (4.01–4.65), 11.9(10.72–13.23), similar to those previously reported reference levels. The IQR for neonate TSH of median levels was 4.2 (2.9–6.70) μIU/mL. The median and IQR urine perchlorate level in pregnant women was 3.64 (2.17–6.19) μg/L. Infant TSH was positively correlated not only with urinary perchlorate concentration but also with age of mother and FT3 of the mother. The maternal urinary perchlorate levels were significantly higher in the neonates with TSH levels higher than 10 μIU/mL (p = 0.038).
Lactating Women in Turkey have higher perchlorate levels (both for Cr adjusted and non adjusted) when compared to the women in the USA. Turkey is a mild iodine deficient country, also exposure to NIS inhibitors is high; thus thyroid health is very critical for this population.
Thyroid Cancer Monday & Tuesday Short Call Posters Basic
Genomic structural variations (SVs), including insertions, deletions, and translocations, may drive malignant transformation in the thyroid gland and other tissues. However, sequencing reads of 50–200 bp used by many next-generation sequencing technologies may miss SVs because the sequences are too short to identify SVs and/or map putative SVs to a particular genomic locus. The Irys system, manufactured by BioNano Genomics (San Diego, CA), assembles de novo genome maps by imaging single DNA molecules ranging in length from 150,000 bp to >1,000,000 bp that have been fluorophore-labeled at specific 7-bp sequences. The resulting label pattern, combined with long DNA molecules, allows SVs to be accurately identified and mapped in the genome assembly. To identify SVs in thyroid cancer we used Irys to map blood (germline), thyroid tumor, and adjacent normal tissue genomes from a patient with follicular variant papillary thyroid cancer.
DNA molecules up to >1,000,000 bp in length were extracted the from blood, thyroid tumor, and adjacent normal tissue of a single patient. Fluorophore-labeled DNA molecules >150,000 bp were imaged using the Irys system. De novo maps were assembled at 88X coverage for germline, 72X coverage for normal tissue, and 102X coverage for tumor tissue using the Irys analysis pipeline. To identify SVs, patient maps were aligned to an hg19 reference map generated in silico.
Relative to the hg19 reference map we identified 720 putative insertions and 377 putative deletions in the patient germline map; 752 putative insertions and 395 putative deletions in the patient normal tissue map; and 744 putative insertions and 387 putative deletions in the patient tumor map. Further analysis revealed that 124 (17%) of the putative insertions and 69 (18%) of the putative deletions in the tumor map were not present in either the germline or adjacent normal tissue maps.
These data represent the first attempt to generate de novo maps of a solid tumor genome and suggest that genomic structural variations may be an important feature of malignant transformation in thyroid cells. Additional work is underway to validate the putative structural variations and characterize their functional significance.
Thyroid Cancer Monday & Tuesday Short Call Posters Basic
Extracellular vesicles (EVs) are released from cells into extracellular space, and are capable of carrying protein, mRNA and miRNA. Numerous studies have found that tumor-derived EVs (tEVs) transferring oncogenic activity and promoting tumor progression. Despite intense research in the field, there have been only few studies on EV distribution in vivo animal model with bioluminescence imaging (BLI) reporter. This study investigates the visualization and biodistribution of tEVs in mice using generated bioluminescent EVs in vivo.
Human anaplastic thyroid cancer cells (CAL62) were transduced with a lentivirus expressing Rennila luciferase (Rluc). CAL62 cell culture media was harvested and EVs were isolated by ultracentrifugation. EVs were analyzed by TEM and ELS. Rluc expression in EVs was determined by western blotting(WB) and BLI. To visualize and track the distribution of EVs in vivo, EVs or PBS was I. V injected into mice. The coelenterazine was injected over different time points and organ distribution of EVs was determined, imaged under IVIS imaging system. CAL62/Rluc cells were cultured with the EVs, change of cell proliferation were analyzed.
CAL62 cells were stably transfected with Rluc. BLI and WB confirmed Rluc reporter. EVs structure, size and protein markers were confirmed by TEM, ELS and WB respectively. In vitro, WB and BLI revealed the EV exhibits reporter. BLI revealed a significant amount of Rluc signal in the region of lung, liver and spleen in EV injected mice, but not the controls. Ex vivo BLI of organs revealed high signals from the liver, lung, and spleen and kidney which was corresponding to in vivo BLI imaging. The EVs enhanced CAL62 proliferation.
We successfully developed EV reporter system that enables in vivo imaging. In vivo and ex vivo imaging revealed that the tEVs distributed to organs. This is the first distribution study of EVs of thyroid cancer cells having Rluc reporter gene.

Thyroid Cancer Monday & Tuesday Short Call Posters Clinical
Infiltrative follicular variant of PTC (IFVPTC) and Encapsulated Follicular variant of PTC (EFVPTC) are known subtypes of Follicular variant of Papillary Thyroid Carcinoma (FVPTC). The EFVPTC is known to have a good clinical behavior whereas IFVPTC sometimes behaves like PTC and sometimes like FTC which exhibits aggressive clinical behavior. Thus, the precise clinico-pathological behavior of IFVPTC remains inexact and elusive. We therefore analyzed the clinico-pathological behavior of IFVPTC and compared it with clinico-pathologic behavior of FTC variants. This unpredictable and uncertain behavior of IFVPTC creates a dilemma for clinicians as to how best to manage it.
The clinico-pathologic characteristics of 45 cases of FVPTC (19 cases of IFVPTC and 26 cases of EFVPTC) and 70 cases of FTC (40 cases of Minimally invasive FTC and 30 cases of Widely invasive FTC i.e. WIFTC) who underwent surgery from 2007–2010 at the Dept. of Endocrine Surgery, SGPGIMS Lucknow; were retrospectively analyzed and compared. SPSS software version 17.0 and non parametric tests were used for statistical analysis.
Clinico-pathological features of IFVPTC and WIFTC patients resembled each other more closely than the other variants of PTC and FTC. Patients of IFVPTC and WIFTC more commonly presented as Multinodular goiters, had higher incidence of Extra-thyroidal extension (p < 0.001). Histologically, these variants also exhibited higher incidence of capsular invasion (p < 0.001) and vascular invasion (p < 0.001). Additionally, IFVPTC presented more commonly in males. Incidentally, widely invasive and minimally invasive FTC patients had larger tumor size and tumor weight when compared with IFVPTC and EFVPTC. Pre-op TSH levels among all the variants were statistically not significant.
IFVPTC resembles more with WIFTC both clinically as well as histologically in terms of capsular and vascular invasion leading to distant metastases but resembles more with PTC in terms of lymph node metastasis. Thus, IFVPTC has an unpredictable behavior and should to be managed more aggressively.
Thyroid Cancer Monday & Tuesday Short Call Posters Translational
It is well accepted that 70% of thyroid tumors exhibit unregulated signaling through the RAS-ERK pathway. Thyroid cancer patients have a good clinical outcome, however about 10% of them progress to radioactive iodine-refractory disease, emphasizing the importance of developing novel effective therapies. Recently, significant advances have been accomplished by developing pharmacological agents directed against the kinases of the RAS-ERK pathway. However, most of the molecules tested have undesired side effects and promote drug resistance. Consequently it is imperative to find alternative RAS-ERK pathway inhibitory therapies. Activated ERK dimerize, which plays an essential role in ERK's cytoplasmic but not nuclear functions. It has been shown that inhibiting ERKs dimerization suppresses tumor progression. Very recently, a small molecule inhibitor for ERK dimerization (DEL22379) has been identified that, without affecting ERK phosphorylation and activity, impedes the growth of melanoma tumor cells driven by RAS-ERK pathway oncogenes (Cancer Cell 28:170–82 2015). Thus the objective of our work was to study whether the inhibition of ERK dimerization in thyroid cancer results in an antitumor effect.
We have used as a model system thyroid tumor cells harboring oncogenic drivers (RAS, BRAF, RET/PTC) and an orthotopic mouse model.
We show that DEL22379 inhibits ERK dimerization induced by EGF in thyroid tumor cells. In general, BRAF mutant cells are more sensitive to the inhibitor than RAS mutant cells. Interestingly, the inhibition of ERK dimerization results in actin fibers depolymerization which could lead to inhibition of cell migration. In addition, in vivo analyses using an orthotopic mouse model, show a drop in tumor growth rate in the K-RAS mutant anaplastic tumor derived-cell line Cal62 when ERK dimerization was impaired after DEL22379 treatment.
These results describe a new molecule that could be effectively used as therapy in thyroid cancers harboring RAS-ERK pathway oncogenes. Future initiatives are aimed at studying in more detail the antitumor effect of this compound as well as if it is affected by a resistance mechanism as BRAF/MEK inhibitors are.
Thyroid Hormone Action Monday & Tuesday Short Call Posters
To determine the correlation between the usage of sugar substitutes (Artificial Sweeteners) in human subjects and development of HT.
Review of electronic medical records, a total of 100 patients with a diagnosis of HT, (positive Thyroid Peroxidase (TPO) antibodies) were included in the study. The patients were interviewed in person or over the telephone and they were asked to respond to a questionnaire, pertaining to the use of artificial sweeteners in their diet. Gender, ethnicity, TSH, free T4 levels, weight, LT4 dose and a family history of thyroid disease were included. Control Group: a total of 125 patients without TPO antibodies (euthyroid), were included in the study.
Of the 100 patients, a total of 53 patients (53%) took artificial sweeteners while 47 patients (47%) did not take any. In the control group 15 patients were sweetener users compared to 110 patients non users. Statistical analysis done with Pearson correlation test between the average number of packs of artificial sweeteners consumed daily, and TSH values showed a positive correlation of 0.23 with a p-value of 0.05. Fisher's Exact Test showed statistical significant association (interdependency) between use of sweeteners and hypothyroidism anti-TPO antibody (p < 0.01). Sugar substitutes have been reported to cause autoimmune disorders in animals. Aspartame, Sucralose and Saccharin; ingredients of artificial sweeteners, are known to cause side effects in animals. Aspartame gets metabolized to formaldehyde and been associated with Type IV delayed hypersensitivity reactions. In rats fed with sucralose a decrease in the size of thymus and spleen and lymphopenia has been noted, implying that it could have a negative effect on immune system. This study show a high prevalence (53%) of HT in patients consuming artificial sweeteners.
This study emphasizes that in patients with HT, a history of intake of artificial sweeteners should be obtained and an attempt should be made to discontinue artificial sweeteners from their diet with follow up of TSH level.
Thyroid Nodules & Goiter Monday & Tuesday Short Call Posters Basic
We have previously shown that the regulation of NIS function during goitrogenesis is affected by the size of the goiter. Herein, we aimed to evaluate thyroid H2O2 generation in different stages of goiter and the correlation with NIS, TGFb-1, TGFβ receptor (TGFβR) and NOX4 mRNA expression.
Adult Wistar rats were treated with 0.03% MMI for 5 (M5) or 21 (M21) days to induce different stages of goiter. In order to evaluate the effect of the resumption of iodine organification, MMI was withdrawn one day before sacrifice (M5R1 and M21R1). NIS, TGFβ-1, TGFβR and NOX4 mRNA levels were evaluated by RT PCR and H2O2 generation was assessed by Amplex red method.
MMI withdrawal one day before the sacrifice led to a great reduction of NIS mRNA in the two stages of goiter development (C = 1.00 ± 0.15, M5 = 4.2 ± 1.37*, M5R1 = 0.50 ± 0.06, M21 = 6.13 ± 1.26*, M21R1 = 1.15 ± 0.07; *p < 0.05 vs. C). TGFβ-1 mRNA increased in most groups that received MMI (C = 1.00 ± 0.11, M5 = 1.90 ± 0.42*, M5R1 = 2.04 ± 0.19*, M21 = 1.60 ± 0.24, M21R1 = 2.18 ± 0.27*; *p < 0.05 vs. C). TGFβR mRNA levels only increased in late stages of goiter (C = 1.00 ± 0.05, M5 = 0.85 ± 0.04, M5R1 = 0.87 ± 0.02, M21 = 1.33 ± 0.05*, M21R1 = 1.27 ± 0.15*; *p < 0.05 vs. C). NOX4 mRNA levels increased in all MMI groups, except M5 (C = 1.00 ± 0.17, M5 = 1.32 ± 0.10, M5R1 = 1.88 ± 0.10*, M21 = 2.01 ± 0.26*, M21R1 = 2.52 ± 0.25*; *p < 0.05 vs. C). H2O2 generation was increased in both M5 and M21R1 groups (C = 1.00 ± 0.08, M5 = 1.70 ± 0.18*, M5R1 = 1.37 ± 0.22, M21 = 1.05 ± 0.13, M21R1 = 1.80 ± 0.23* nmol H2O2. h-1. mg-1 protein; *p < 0.05 vs. C).
Our study shows that NIS mRNA is down-regulated 1 day after MMI withdrawal, independently of the size of the goiter, differently from NIS function. Moreover, we have found the greatest H2O2 generation along with the highest NOX4 expression in M21R1. This group also showed increased TGFβ-1 and TGFβR mRNA expression. Since TGFβ has been shown to stimulate NOX4 expression in different cell types, one can speculate that the increased TGFβ signaling after MMI removal might stimulate NOX4 expression in the thyroid, leading to increased H2O2 production, which could in turn down-regulate NIS. Thus, our data suggest that TGFβ is involved in ROS production and NIS expression regulation during goitrogenesis.
Thyroid Nodules & Goiter Monday & Tuesday Short Call Posters Clinical
We evaluated the clinical utility, long-term management patterns and surgical rates between matched cohorts of patients with Afirma gene expression classifier (GEC) benign and cytopathology benign diagnoses in the HealthCore Integrated Research Database (HIRD). Patients whose thyroid fine needle aspiration (FNA) sample was sent to Veracyte, Inc. for cytopathology and GEC testing between January 1, 2011 and August 31, 2013 were included if their nodule was least 1 cm in size and they had continuous health plan enrollment for at least 6 months pre-FNA and 12 months post-FNA. Patients with cytopathology benign diagnoses were matched (3:1) to patients with GEC benign results on year of biopsy, gender, nodule size (-/+1 cm) and age (-/+5 years). The matched cohorts were evaluated for clinical follow-up including ultrasound exams and thyroid surgery.
1,259 patients with a cytopathology benign diagnosis and 218 patients with a GEC benign diagnosis were identified in the HIRD database and met the continuous enrollment criteria. 603 cytology benign patients were matched to 201 GEC benign patients. Mean nodule size was 2.2 cm (SD 1.0) and 2.3 cm (SD 1.0) for the cytopathology benign and GEC benign groups, respectively (p = 0.38). In both groups mean post-test follow up was 20 months (SD 5.5), mean age was 51 years (SD 12) and 83.1% were female. 61.7% and 60.2% of patients with cytopathology benign and GEC benign diagnoses respectively underwent a follow-up ultrasound exam (p = 0.707). The proportion of cytopathology benign (n = 61, 10.1%) and GEC benign (n = 23, 11.4%) patients that underwent thyroid surgery was not significantly different (p = 0.594).
In this national health plan database the GEC benign diagnosis is durable with an operative rate equivalent to that of a cytopathology benign diagnosis. An equivalent majority of patients in both groups were managed with ultrasound exams throughout an average follow-up of 20 months consistent with recommendations for benign nodules. This observed surgical and ultrasonography follow-up patterns suggest very similar management protocols of GEC benign and cytology benign patients.
Wednesday, October 21–Thursday, October 22, 2015
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters
Radioimmunological assays are utilized for the most hormonal measurements including serum Thyrotropin(TSH), Free T4 and Free T3 assays. Challenges arise when entirely different measurements are obtained at two different laboratories or discordant thyroid function tests are obtained not keeping with the clinical picture.
We present two case reports. The first Case is a 66-year-old woman was referred for poorly controlled hypothyroidism. She had a history of hyperthyroidism and received RAI treatment and became hypothyroid. She has been on Levothyroxine treatment since. She had developed elevated TSH, Free T4 and Free T3 both at private and hospital laboratories on multiple occassions. The second case is regarding a 60-year-old woman was referred for hyperthyroidism. Her TSH was suppressed and fT4 elevated at the hospital laboratory. The radioiodine uptake scan showed mild increased uptake. She was started on Propylthiouracil, intially at high doses and the dose was gradually reduced. In subsequent months, patient showed clinical improvement but TSH level remained suppressed and Free 4 and Free T3 levels remained high. Her TFTs were repeated at a private laboratory on different occassions and they were completely different from the hospital laboratory results.
These two cases exemplify the challenges of interpreting TFTs. In Case 1, the most likely cause is interference with TST assays.1,2 Thyroid hormone autoantibodies as well as heterophilic antibodies are known to interfere with the VITROS TSH test3, performed at our centre, as well as fT4 RIAs. In Case 2, the disparity of the TFT test results were demonstrated by comparison of hospital-based and private laboratories. TFTs measured at a private laboratory, which utilized a different RIA, showed discordance with hospital lab-acquired values.
Thyroid hormone assay problem is likely in both of these patients. Serum heterophile antibodies interfere with radioimmunological assays. Hospital and private laboratories use different radioimmunological assays. Awareness of that is important to ensure patients do not receive unnecessary treatment.
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters Clinical
Iodinated contrast media (ICM), routinely used in imaging studies, contains several hundred-fold times the recommended daily allowance of iodine. Iodine excess predisposes to thyroid dysfunction, and normal thyroid hormone levels are crucial during neurodevelopment and growth. We hypothesized that children exposed to ICM have an increased risk of iodine-induced thyroid dysfunction.
This was a case-control study of UCLA patients aged <18 years from 2001–2015. Cases were defined as those with thyroid dysfunction (by ICD-9 codes and/or 2 consecutive abnormal serum TSH values <6 months apart) and 1:1 matched to euthyroid controls by age, sex, and race (White vs. non-White). Using conditional logistic regression, we estimated the association between ICM exposure and incident thyroid dysfunction occurring within 2 years of exposure.
870 cases were matched to 870 controls (36% male; 51% White). Sixty-nine patients received ICM (53 [6.1%] of cases (mean±SD age, 8.4 ± 6.1 yrs) and 16 [1.8%] of controls (mean±SD age, 7.3 ± 7.3 yrs)). The risk of incident hypothyroidism was significantly increased following ICM use (OR 2.60; 95% CI 1.43–4.72; p < 0.0017), with 11.7 ± 7.1 months as the mean ± SD time between ICM administration and hypothyroidism (median serum TSH concentration 7.8 mIU/L [6–14.7, IQR]).
ICM exposure significantly increases the risk of incident thyroid dysfunction in pediatric patients. Children receiving ICM should be monitored for iodine-induced thyroid dysfunction, particularly in the first year following an excess iodine load.
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters
Thyroid storm (TS) is characterized by exacerbated manifestations of thyrotoxicosis. Although aggressive medical therapy is the first line treatment, there is few data available regarding the optimal therapy for refractory cases. In such situations, plasmapheresis should be considered. The aim of this study was to assess the efficacy of plasmapheresis in refractory TS.
We retrospectively evaluated all cases of refractory TS (Burch and Wartofsky score >45), treated with plasmapheresis between 1991 and 2014 in a tertiary hospital. To compensate for different assays, hormone results are presented as elevation above the upper limit of normal (ULN). Statistical analysis was performed with Wilcoxon test (SPSS v.21).
Ten cases were recorded. The median age was 51.5 years and 8 patients were female. Five TS patients were secondary to exogenous thyroid hormone intake, 3 had amiodarone induced thyrotoxicosis, 1 Graves Disease and 1 a thyrotrophinoma. Four infections, 1 drug withdraw and 1 131Iodine treatment were identified as triggers. The Burch-Watshofky score ranged from 50 to 105: 7 had severe central nervous system disturbance, 3 acute heart failure and 10 had tachycardia. All patients were treated with thionamides, iodine, glucocorticoids, beta-blockers and cholestyramine. Plasmapheresis sessions ranged from 3 to 5 and lasted between 3 to 10 days. Before plasmapheresis, median TT4 was 2,7x ULN, FT4 7,2x ULN, TT3 2,7x ULN and FT3 3,9x ULN. The first plasmapheresis induced a significant decrease in median TT4 (37%, p = 0,008), FT4 (45%, p = 0,018) and TT3 (48% p = 0,012). After the last plasmapheresis a significant decrease in all thyroid hormone levels was observed: TT4-66%, FT4-67%, TT3-82% and FT3-70%. (Z = -2,7, P = 0,0008, r = 0,6). On follow-up 9 patients were discharged (4 after total thyroidectomy) and the thyrotrophinoma patient died.
Our study showed that plasmapheresis allowed 90% of the patients to recover, spontaneously or after total thyroidectomy. It should be strongly considered as a second line therapy for refractory TS.
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters Clinical
Autoimmune Hashimotos Thyroiditis is the most common cause of Hypothyroidism in iodine sufficient population. Goitre, Dyshormonogenesis and hypothyroidism are the hallmark of the disease. Presently the treatment is aimed at biochemical correction of hypothyroidism with normalising ft4. TSH levels without addressing Dyshormonogenetic Goire. This has resulted in increasing Goitre andThyroid Carcinomas. The study highlights the use of Levo Thyroxine (T 4) in supraphysiological doses and resultant TSH suppression, goitre reduction and Euthyroidism with physiological levels of T3.
One hundred patients who attended Thyroid Centre during january 2014 with goitre and hypothyroidism and followed up with supressive thyroxine therapy till july 2015 constituted the study. The selection criteria included a) hypothyroid symptoms b) Goitre The patients were subjected to detailed clinical examinations. including physical examinations of thyroid, Thyroid hormones, TSH, Thyroidantibodies The patients were treated with suppressive doses of Levo thyroxine (T4) 1.5 to 2mcg/Kg BW so as to achieve suppressed levels of TSH less than 0.01miu/ml with normal or marginally increased T4 levels 5–12 mcg/ml and normal T3 /FT3 levels 0.7–2.1 ng /ml. Patients were followed at 3 to 6 monthly interval and progress noted on goitre and symptoms reduction.
Patients in the age group of 20 to 50 years constituted 76% with female predominance 0f 84 :16. T3 levels 120±20ng/dl(60–200), T4 levels 11± 2.3 mcg/dl (4.5–12) and TSH 0.01 ±0.05 miu/ml (0.30–5.5). All patients with weight gain, lethargy, body aches, joint pains, hairfall, increased sleep, foreign body sensation throat and memory loss had marked improvement in symptoms. Goitres markedly regressed in size. There were no toxic symptoms.
Levo thyroxine in marginal supraphysiological doses suppress TSH levels. This results in goitre regression and reduces the incidence of papillary carcinoma thyroid. T3 is converted from T4 at 80%efficency and thus physiological levels and euthyroidism are maintained. The study highlights the urgency of adopting this treatment in management of Hashimotos Hypothyroidism and preventing DTC.
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters Translational
The TRH receptor (TRHR) is a G-protein coupled receptor activated by hypothalamic TRH. In thyrotropes, TRH-TRHR signaling controls synthesis, secretion and bioactivity of TSH. Human TRHR gene defects are extremely rare, and only two cases are known showing central hypothyroidism and short stature as presenting features. Objective Phenotypical characterization of a family with suspected central hypothyroidism and investigation of the molecular mechanism underlying the disorder.
Patients & Methods Mutation screening of the TRH, TRHR and TSHB genes in seven individuals of a consanguineous pedigree. Determination of membrane expression, ligand affinity and transactivation properties of a TRHR mutant using ELISA, ligand ([3H]MeTRH) binding and luciferase reporter assays, respectively.
A homozygous missense mutation in TRHR was identified (c.392T>C; p. I131T) in a 7 year old boy with mild central hypothyroidism (TSH: 2.61 mIU/mL, FT4: 0.74 ng/dl) and overweight, but normal stature (122 cm; -0.58 SD). TRH test showed borderline-low TSH response, consistent with pituitary hypothyroidism. The parents, two siblings and grandmother of the index patient were heterozygotes for the mutation, and showed isolated TSH elevation (4.6–8 mIU/L). The mutation localises in the 2nd intracellular loop of the TRHR, adjacent to the D/ERY motif involved in G protein activation. The I131T TRHR mutant impairs transactivation of an AP1-containing promoter by TRH (wild type EC50 = 2.8 ± 0.9 nM vs. mutant EC50 = 20.4 ± 0.8 nM), showing its pathogenicity. The mutant does not interfere receptor trafficking to the membrane, but impairs signal transduction by decreasing its affinity to TRH (wild type = 9.1 ± 0.4 nM vs. mutant = 3.1 ± 0.3 nM)).
A novel defect in TRHR causes mild central hypothyroidism in the homozygous state but leads to hyperthyrotropinemia in heterozygotes, suggesting compensatory elevation of TSH with reduced biopotency. The mutation impairs TRH-TRHR signalling by decreasing the affinity to high doses of TRH, and suggests incomplete activation of G-proteins by dysfunction of the D/ERY motif.
Disorders of Thyroid Function Wednesday & Thursday Short Call Posters Translational
Has been described an association between thyroid disease and cardiovascular disease mortality. The metabolic syndrome (MetS) has been linked as the potential biological mechanism. In Mexico, cardiovascular disease is the first cause of mortality, 49.8% of adults have MetS and 12% of the population is classified as risk of thyroid disease. However, there is not information available to describe this association in Mexico. Therefore, the aim of this study is to describe the association between thyroid disease (alterations in the serum concentrations of TSH, T3 and T4) and MetS in a national representative sample of Mexican adults who participated in the Mexican National Health and Nutrition Survey 2012 (MNHNS-2012).
We include a sample size of 3,800 participants ≥20 years of age representing 69’245,519 adults. For the diagnosis of MetS, we used the classification from the International Diabetes Federation. Blood pressure, body weight, waist circumference (WC), fasting blood glucose, fasting insulin, total cholesterol, c-HDL, c-VLDL, triglycerides (TG), C-reactive protein, thyroid-stimulating hormone (TSH), triiodothyronine (T3), and thyroxine (T4) were measured.
The mean serum TSH concentration was 2.3 μUI/ml [95% IC 1.8, 2.4], mean serum T3 was 1.2 μUI/ml [95% IC 1.1, 1.3], and mean serum T4 6.4 μUI/ml [95% IC 6.1, 6.8]. Almost 12% of the population presented hyperthyroidism (subclinical or clinical) and 12.8% have subclinical hypothyroidism. This represents almost 10 million Mexicans with elevates TSH (≥4.5 μUI/ml]) and 3 million with low TSH (<0.45 μUI/ml). Forty-eight percent of the adults had MetS. The mean serum concentration of TSH in adults with obesity was highest (2.44 μUI/ml [95% CI 2.07–2.81] than in adults with BMI normal (2.24 μUI/ml [95% CI 2.20–2.37]. After adjusting for age, sex, and physical activity TSH levels were positively associated to WC, TG and c-HDL. T4 was positively associated to blood pressure and WC. In the comparison between individuals with and without MetS there was no statistically significant difference (p > 0.05) in TSH concentrations.
There is a relationship between thyroid function (TSH, T4) and some components of MetS such as WC, TG and c-HDL, but not with all syndrome.
Thyroid & Development Wednesday & Thursday Short Call Posters Clinical
In addition to the recurrent laryngeal nerve injury, postoperative hypoparathyroidism is a common complication of thyroidectomy. Up to date, there is no direct evidence to indicate parathyroid glands (PGs), which were preserved in situ, survived. We hypothesized that the postoperative serum calcium, serum parathyroid hormone (sPTH) and especially the drainage parathyroid hormone (dPTH) are significant prognostic parameters of parathyroid glands which were preserved in situ.
90 patients who received initial surgical treatment at our institution between April 2012 and August 2012 were enrolled in this study. Patients were divided into four study groups: Group 1, total thyroidectomy (TT); Group 2, TT and bilateral central neck dissection (CND); Group 3, TT and functional neck dissection; Group 4, unilateral thyroidectomy. Postoperatively, serum calcium, sPTH, and dPTH were tested every morning for 4 consecutive days. The levels of serum calcium, sPTH and dPTH were analyzed by repetitive measure analysis of variance (ANOVA).
Mean postoperative serum calcium was highest in Group 4, indicating that unilateral thyroidectomy is associated with a lower rate of postoperative hypocalcaemia. The average sPTH was highest in Group 4 and was lowest in Group 2 and 3 after surgery. This implies both bilateral CND and functional neck dissection were associated with low postoperative sPTH. Analysis of data showed no statistical difference in postoperative dPTH between the four study groups. However, it decreased with time gradually in all groups. After surgery, 35 patients experienced transient hypocalcaemia. No permanent hypocalcaemia was observed in this study.
Our results indicate that the level of postoperative dPTH is a direct evidence that the PGs, which were preserved in situ, survived. The low sPTH, but high dPTH after surgery indicate the surgery influenced the PTH secretion, but the PGs are still functioning. sPTH will increase gradually with the reconstruction of microcirculation. By contrast, persistent low sPTH and dPTH after surgery suggest that PGs were seriously damaged and more than one PG were affected. Postoperative parathyroid dysfunction will result.
Thyroid Cancer Wednesday & Thursday Short Call Posters Basic
Subsets of well-differentiated thyroid carcinoma patients suffer significant morbidity and mortality from recurrence and progression, underlying a need for new therapeutic approaches. Adoptive transfer of T cells engineered to express chimeric antigen receptor (CAR) specific to tumor-associated antigen have shown impressive clinical outcomes in hematologic cancers. The expression of a cell surface molecule known as the intercellular adhesion molecule 1 (ICAM-1) was significantly associated with the malignancy, drug resistance, and metastatic status of thyroid tumors and was correlated with the BRAFV600E mutation.
We analyzed the surface ICAM-1 expression levels in untreated and BRAFV600E inhibitor vemurafenib-treated PTC line BPAP and anaplastic thyroid cancer cells (ATC) FRO and 8505C by flow cytometry. Vemurafenib-resistant thyroid cancer cells were established by increasing the drug dose weekly. Western blot analysis showed the expression and phosphorylation levels of ERK protein.
More than 94% of cells in BCPAP and over 63% of ATC expressed ICAM-1 (Fig.1A). ICAM-1 expression was significantly increased in thyroid cancer cells after vemurafenib treatment (Fig. 1C, D). Majority of ATC became ICAM-1-positive after drug treatment, indicating a correlation between ICAM-1 expression and drug resistance. We isolated a vemurafenib-resistant FRO clone, which exhibit less decreased level of ERK phosphorylation with vemurafenib treatment. The entire population of this vemurafenib-resistant FRO cells expressed ICAM-1. We isolated the single-chain fragment variable from R6.5 mouse monoclonal antibody against human ICAM-1 and inserted into a CAR lentiviral construct. Currently, we are testing the cytotoxic effect of ICAM-1-targeting CAR T cells on thyroid tumors and the combined effect of ICAM-1 CAR T cells and vemurafenib.
Nearly all of the thyroid tumors cell lines tested were ICAM-1-positive after vemurafenib treatment, demonstrating ICAM-1-targeting therapeutics as a new modality for drug-resistant cancer treatment. This approach of combination of targeted drug and immunotherapy is promising for metastatic and recurrent thyroid cancer patients with few therapeutic options.
ICAM1 induction in thyroid tumors. (A) Flow cytometryic analysis showing ICAM1 expression in thyroid cancer cell lines (B) MTT assay to determine IC50 for vemurafenib (C) ICAM1 surface expression level induction in vemurafenib-treated cells (D) Mean fluorescence intensities (MFI) of vemurafenib-treated cells after 24hr and 72hr treatment.

Thyroid Cancer Wednesday & Thursday Short Call Posters Basic
Validated cancer cell lines are critical models to study the development and progression of cancer, as well as the identification of new therapeutic targets. We have recently reported a comprehensive analysis of human thyroid cancer cell lines and shown that nearly 50% of these cell lines were redundant and many were not of thyroid cancer origin (Schweppe et al 2008). To better understand disease pathogenesis, we have developed two novel cell lines derived from two different patients with PTC pleural effusions, CUTC5 and CUTC48.
Two cell lines were generated using in vitro approaches, and considered permanent after >6 months in culture, >20 passages, and the ability to freeze down and recover. Cells were characterized using in vitro and in vivo approaches. A screen with kinase inhibitors targeting ∼400 kinases was performed to map key kinase dependencies.
Short tandem repeat profiling showed that each cell line is unique and identical to the original patient tissue samples. Genotyping using the MSK IMPACT panel (Cheng et al 2015) revealed the CUTC5 cells harbor the BRAF V600E mutation. qRT-PCR analysis showed the CUTC48 cell line expresses the RET/PTC1 rearrangement, which was confirmed by the MSK IMPACT panel and Western blotting. Moderate to high levels of Pax-8 and Nkx2.1 were detected by qRT-PCR for each cell line. The kinase dependency screen showed the CUTC5 cells are highly sensitive to BRAF inhibitors (IC50 = 24 nM and 356 nM for dabrafenib and vemurafenib, respectively) and MEK inhibitors (IC50 = 60 nM and 5 nM for selumetinib and trametinib, respectively). Drugs targeting RET showed activity against CUTC48 cells (IC50 = 2–3 μM for lenvatinib, vandetanib, and cabozantinib). The CUTC5 cell line forms colonies in soft agar, tumors in an orthotopic model, and metastases in an intracardiac injection model. The CUTC48 cell line does not form colonies in soft agar or tumors in nude or SCID mice.
We have developed the second RET/PTC1-expressing PTC cell line in the world, which is a major advance in studying RET signaling in DTC. We have further linked both cell lines to the originating patients, providing a set of novel, authenticated PTC cell lines to study advanced thyroid cancer and response to therapy.
Thyroid Cancer Wednesday & Thursday Short Call Posters
A 33 year old female with no significant medical history presented with new onset seizures. MRI brain revealed a 2cm falcine presumptive meningioma and patient underwent craniotomy. Surgical pathology was consistent with metastatic thyroid cancer. ThyroSeq performed on the brain metastasis showed ETV6/NTRK3 gene fusion mutation.
Thyroid ultrasound revealed a 5cm suspicious thyroid nodule. Patient underwent a total thyroidectomy with pathology consistent with infiltrative follicular variant papillary carcinoma. She had no history of head or neck radiation or family history of thyroid cancer. A Thyrogen stimulated whole body scan showed uptake in bilateral lungs, neck and right humerus. Patient received 248 mCi of radioactive iodine with close medical follow up given the aggressive progression of the cancer. She was referred to an outside facility for external beam radiation and possible targeted systemic therapy.
Molecular genetics is an advancing field that can aid in distinguishing more aggressive forms of thyroid cancer. ETV6-NTRK3, which is a fusion of the oncogene ETS Variant Gene 6 (ETV6) to the receptor tyrosine kinase growth factor receptor gene Neurotropin Receptor 3 (NTRK3), is a novel mutation previously described in fibrosarcomas of the breast. ETV6-NTRK3 up regulates MAP kinase which potentially drives the malignancy. The occurrence of ETVK/NTRK3 rearrangement in thyroid cancer is described in post Chernobyl surveillance and in vitro studies where ionizing radiation can induce this mutation in thyroid cells. More recently it has been noted in classical and follicular variant papillary thyroid cancers. Specific knowledge of the gene abnormality leads to the possibility of targeted therapy such as tyrosine kinase inhibitors. Advancing knowledge of genetic markers and driver mutations is an emerging field which can potentially aid in the management of aggressive thyroid cancers.
Thyroid Cancer Wednesday & Thursday Short Call Posters
Thyroid carcinoma is the most common pediatric endocrine tumor, constituting 0.5–3% of all childhood malignancies. Papillary thyroid cancer (PTC) accounts for 90% or more of all childhood cases. The occurrence rate of diffuse sclerosing variant of pediatric papillary carcinoma (DSVPC) reach up to 41%. Also the management of DSVPC looks a challenge and needs a special consideration.
a case report
A 14-year-old girl presented with a six-month history of a right sided neck mass without hoarsenessor intermittent dysphagia. Examination revealed a thyroid nodule on the right lobe of the thyroid gland measures two cm with few scattered bilateral cervical lymphadenopathy. Thyroid ultrasound showed a heterogeneous nodule measuring 1.8cm with microcalcification. Fine needle aspiration of right thyroid nodule revealed Suspicious for papillary thyroid carcinoma in a background of autoimmune thyroiditis. She had total thyroidectomy with bilateral central neck dissection and the pathology showed DSVPC involving both lobes (largest tumor 2.4 cm) with extracapsular extension and metastatic lymph nodes (Perithyroidal 12/17, right central 2/7 and left central 7/9). Her risk was classified as ATA Pediatric Intermediate-Risk. Five months later, she had radioactive iodine remnant ablation dose of 100 mCi. Six months after RAI, she had stimulated Thyroglobulin level of 39 μg/L with Thyroglobulin Antibody 329 IU/ml and neck ultrasound revealed right level IV suspicious LN with 2 foci of abnormal increased tracer uptake in whole body scan(WBS). She had right lateral neck dissection with eleven normal LN and negative left LND sampling. Five months later, she had negative WBS and stimulated Tg 7.4 with significant decreasing level of Tg Abs 48 IU/ml and normal lung CT scan.
On literature review, DSVPC patients present with bilateral thyroid involvement, extrathyroidal extension and LN metastasis when compared to non- DSVPC. Also the recurrence rate and lung metastasis are more frequent. There is no consensus on the prognosis of DSVPC. Unfortunately, the recent American Thyroid Association Guidelines Task Force did not address the pathological subtype of PTC. Pediatric DSVPC requires aggressive treatment and close follow-up.
Thyroid Cancer Wednesday & Thursday Short Call Posters
Thyrotoxicosis following thyroidectomy for thyroid cancer is unusual. This case was consulted a teriary health center at Vizag, India.
Case Presentation: We report a 31 year old man who had a thyroid nodule in the left lobe; it was solid on ultrasound and cold on 131I scan. Biopsy of a left hemithyroidectomy showed an encapsulated mass with papillary processes lined by tall columnar cells having atypical nuclei. It was suggestive of papillary carcinoma of thyroid. Thyroxine was started (150 μg/day) to lower the TSH below 0.5 uiu/ml. He was asymptomatic except for transient ectopic beats 13 years after surgery, when thyroxine was reduced to 100 μg/d; T4 was 10.6 μg/dl and TSH 0.05 uiu/ml. However he continued to lose weight over 7 months and had signs of toxicosis: pulse 110 beats a min, hyperkinesis and eye stare. Thyroxine was stopped but toxic features persisted when he was started on carbimazole 20 mg/day. A month later his tachycardia resolved, he gained 2.2 kg weight and had no toxic signs or symptoms. He is being worked up for the cause of toxicosis and definitive treatment.
Comment: This patient had two features: it shows the possibility of malignancy in a hemithyrectomised gland; and toxicosis following surgery. Current guidelines of total thyroidectomy preceded by imaging, flow cytometry and genetic studies could have prevented the former and perhaps the latter Conclusion: A man developed thyrotoxicosis long after hemithyroidectomy for retrospective diagnosis of papillary cell thyroid carcinoma.
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
Because of the potential prognostic impairment and the difficulties in detection of central lymph node metastasis (CLNM), benefits of prophylactic central neck dissection (pCND) were suggested in clinically node-negative (cN0) papillary thyroid carcinoma (PTC) patients. However, some studies argued that pCND showed no significant reduction in recurrence only paying higher morbidities as a consequence.
A total of 11597 cN0 PTC patients who underwent thyroidectomy with or without pCND between Jan 1997 and Jun 2015 were included. The prognostic impact of pCND including subset analyses according to the clinicopathological characteristics was performed retrospectively.
Of the 11597 cN0 PTC patients, 8752 (75.5%) underwent pCND and 2845 (24.5%) did not underwent pCND. The 5-year, 10-year, 15-year recurrence free survival (RFS) rates in no pCND group were 97.0%, 95.1%, 93.4% and in pCND group were 97.7%, 95.7%, 93.0% (Figure 1). By cox proportional hazard models, overall pCND did not significantly decrease the risk of loco-regional recurrence (LRR) in cN0 PTC patients [adjusted hazard ratio (HR) = 0.874, p = 0.392]. Unilateral pCND did not influence on LRR in cN0 PTC patients with lobectomy (adjusted HR = 0.636, p = 0.131) and bilateral pCND also did not influence on LRR in cN0 PTC patients with total thyroidectomy (adjusted HR = 1.041, p = 0.827). Moreover, pCND did not significantly decrease the risk of LRR in cN0 PTC patients with age <45 yr (adjusted HR = 0.813, p = 0.275), age >45yr (adjusted HR = 0.963, p = 0.852), conventional variant (adjusted HR = 0.845, p = 0.201), BRAF mutation (adjusted HR = 1.006, p = 0.985), tumor size >1cm (adjusted HR = 1.003, p = 0.987), multifocality (adjusted HR = 1.025, p = 0.914), and ETE (adjusted HR = 1.028, p = 0.875). However, complications such as temporary vocal cord palsy (5.9% vs. 2.6%, p = 0.037), temporary hypoparathyroidism (31.1% vs. 12.9%, p < 0.001), and permanent hypoparathyroidism (3.9% vs. 2.0%, p < 0.001) were significantly more frequent in pCND group.
Given the lack of proven benefits and clear evidence of morbidities, pCND should not be recommended as a mandatory procedure. CND are to be reserved for therapeutic situation.
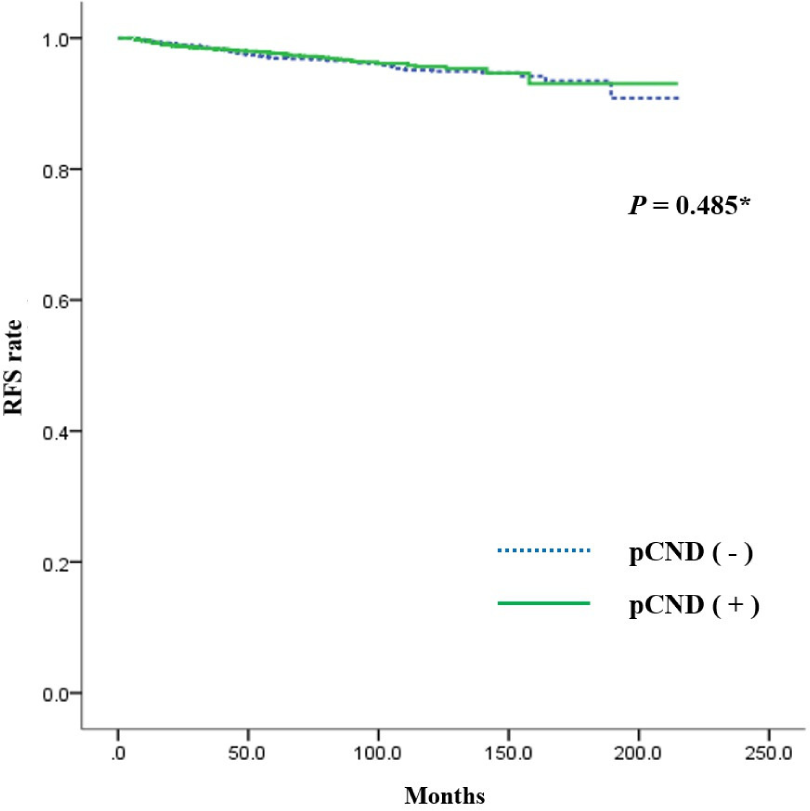
Unadjusted RFS for cN0 PTC patients according to pCND. RFS, recurrence free survival; cN0, absence of clinically detectable lymph node metastasis; pCND, prophylactic central neck dissection.
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
Papillary thyroid carcinoma (PTC) is increasing in incidence while mortality is unchanged. The tall cell variant of papillary thyroid carcinoma (TCVPTC) is associated with aggressive features and a poor prognosis. We explored the genetic profile of a case series of TCVPTC and correlated this profile with the cancer's presentation, pathologic features and clinical course.
Retrospective analysis of our institution's surgical pathologic database (2009–2013) was performed and clinicopathologic data were collected on all patients carrying the diagnosis of TCVPTC. Next generation sequencing was run on all TCVPTC samples, which included analysis of twenty-four related thyroid genes.
Twenty-four patients with TCVPTC were identified and analyzed by next generation sequencing. Thirteen patients (54.2%) were female and average age was 51.3±17.9 years. Thirteen patients (54.2%) were AJCC Stage III or IV at presentation. Tumors were large (2.66±1.85 cm), multifocal (66.7%), and frequently had extrathyroidal extension (62.5%), lymphovascular invasion (58.3%), and lymph node metastasis (79.2%). 87% of tumors undergoing next generation sequencing had the BRAF V600E mutation. TERT promoter mutations were detected in six patients, all of which harbored a BRAF mutation. One tumor had an NRAS mutation. No other known thyroid cancer mutations were identified on mutational analysis. At median follow-up of 24.5 months, eight patients had recurrent disease. Three patients died from complications not related to their thyroid cancer.
The reasons behind the aggressive behavior and poorer prognosis of TCVPTC have yet to be elucidated. Nearly all tumors in our series demonstrated a BRAF V600E mutation which was frequently co-mutated with a TERT promoter mutation. A novel finding was a TCVPTC with a NRAS mutation. Strategies for stratifying risk in TCVPTC patients could potentially include the proportion of mutant versus wild type BRAF genes and the presence of the TERT promoter mutation.
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
Thyroid carcinoma (TC) is rare in young children, but increases during adolescence and young adulthood (AYA). This study sought to describe, at a true population-level, diagnostic, treatment and demographic trends over an 18-year period in Ontario, Canada.
Ontario is a single-payer health system, with centralized billing of physician services and diagnostic testing. We accessed administrative data to derive a retrospective population-based cohort, using the Ontario Cancer Data Linkage (CD-LINK) project. All incident cases of TC from the Ontario Cancer Registry (OCR) are linked to administrative data using a unique encrypted number assigned to each person eligible for health insurance in Ontario. Thus, these data represent comprehensive, unbiased, population-level data. TC diagnoses were identified using ICD-10 code 193. Cases were limited to those diagnosed before 30 years of age, from January 1st 1992 to December 31st 2010, and with the highest level of diagnostic certainty confirmed by either a Regional Cancer Centre Registration or by Pathology report.
We identified 2,552 incident cases of TC. Female: Male ratios for young children (0–12 years) and AYA (13–29 years) were 1.5: 1 and 4.56: 1, respectively. In 1.8% of cases, thyroid cancer was not the primary oncologic diagnosis. The median interval between the primary malignancy and TC was 11.55 years, with females 2.1 times more likely to be diagnosed with TC following a primary malignancy. Subsequent malignancies following TC diagnosis occurred in 0.88% of cases: 73% of these cases were female and 63.63% of cases received therapeutic radioiodine. There were 15 deaths. There were twice as many deaths among males versus females. Age-specific TC incidence rose in all age categories. Total thyroidectomy followed by staged thyroidectomy was the most frequently performed procedures, 62% and 22%, respectively. Among those undergoing thyroid surgery 24% also underwent parathyroid re-implantation.
Thyroid cancer incidence is rising in Ontario particularly among young children and young adults. Further research is needed to explain the rise in TC incidence and associations with other malignancies.
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
The detection of BRAF V600E mutation in papillary thyroid cancer (PTC) may predict radioiodine responsiveness, potentially guide genotype-targeted therapy, and has been associated with a worse outcome in some studies. PCR-based testing modalities might be less cost-effective and less readily available than IHC tests. Recent studies had utilized BRAF V600E immunohistochemistry (IHC) with varying semi-quantitative criteria to detect the mutation in PTC. We aim to validate a BRAF IHC score that predicts mutational status.
BRAF V600E mutation was tested in archival tissue from classical PTC from 49 patients (size >1cm), using both Sanger sequencing and IHC. Cytoplasmic BRAF staining intensity was graded 0–3 and staining proportion 0–100%. The IHC staining was evaluated independently by 2 pathologists after which an average value was obtained. The BRAF IHC score was derived by multiplying IHC staining intensity by the average staining proportion. The ROC curve analysis was utilized to establish the IHC score cut-off. Clinicopathologic features at presentation were correlation with BRAF mutational status.
BRAF V600E mutation was present in 69% (34/49) of patients in this cohort when tested using Sanger sequencing, and it was present in 80% (39/49) when tested using IHC score. Taking a BRAF IHC cut-off score of 200 (with area under ROC curve as 0.859), the test sensitivity is 100%, specificity is 67%, negative predictive value is 100%, and positive predictive value is 87%. The BRAF mutational status (tested by PCR or IHC technique) was not associated with larger tumoral size, lymph node metastases, extrathyroidal extension, or lymphovascular invasion in this cohort.
The BRAF IHC score is sensitive and relatively specific in predicting BRAF V600E mutational status in classical PTC. The high BRAF V600E mutation rate in our study is consistent with that reported in other Asian studies (80%) compared to studies with Caucasian patients (45%). BRAF mutational status was not associated with worse clinicopathologic features at presentation in this study.
Correlation between BRAF V600E mutation IHC staining & PCR

Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
Pathological examination occasionally reveals incidental positive central lymph nodes (N1a) after thyroidectomy in patients with papillary thyroid cancer (PTC). Incidental N1a is defined as perithyroidal lymph nodes (LN) with metastatic cancer on final pathology in the absence of a formal lymph node dissection. The anticipated 2015 ATA guidelines will likely classify N1a metastases (detected via formal central LN dissection) that are small in size, limited in number, and without extranodal extension as having a low risk of recurrence. We aimed to investigate whether this is true for patients with incidental N1a.
We conducted a retrospective review of consecutive patients undergoing total thyroidectomy for PTC in a high-volume tertiary referral center. Patients with distant metastases, central or lateral neck dissection, pre-operative suspicious LN by ultrasound or intra-operative suspicious LN were excluded. Univariate and multivariate analyses were used to identify factors associated with recurrent disease.
Of 877 patients undergoing thyroidectomy for PTC, 225 had incidental LN within the surgical specimen. Final pathology revealed 183 (81%) patients with N0 and 42 (19%) patients with N1a disease. The average number of resected LN was 2.3, with a mean size of 2.6 mm. Patients with incidental N1a disease were younger (mean 40 vs. 47 years), had larger primary tumors (mean 18 vs. 13 mm), and were more likely to have extrathyroidal extension (31% vs. 8%) and receive RAI (69% vs. 41%). With a mean follow up of 44 months, disease recurred in 8 of 183 (4.4%) with N0 disease compared to 7 of 42 (16.6%) with incidental N1a (p < 0.01). In multivariate analysis, incidental N1a disease was an independent predictor of recurrent disease with an odds ratio of 3.6.
Patients with PTC and incidentally lymph node metastases have a significantly increased risk of recurrent disease, even with low risk primary tumors. These patients may need to be treated more aggressively with RAI or increased surveillance.
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
During follow up, DTC patients after TT with Periodic serum Tg or anti-thyroglobulin antibody levels rising, but negative imaging, always confuse to determine whether to further operate or RIA. To assess the value of the biochemical response and neck ultrasound to predict the recurrence of DTC by 5 years follow-up.
120 DTC patients, who were treated with total thyroidectomy with or without neck dissection.55.83% were treated with postoperative radioiodine therapy. Periodic serum TSH, FT3, FT4, Tg, anti-thyroglobulin antibody levels were measured and neck ultrasound scan for 5 years follow-up after total thyroidectomy.
There is no evidence of recurrence or metastasis from neck ultrasound scan for the 120 DTC patients at the 5 years follow-up after TT. Periodic serum Tg level were measured and distributed, according to the risk stratification system in 2014 ATA guidelines (DRAFT). 44.17% were low-risk patients, 24.53% (n = 13) were treated with RIA, Tg ≥1ng/mL (76.92%), Tg <0.1ng/mL (23.08%); other 75.47% (n = 40), Tg ≥1ng/mL (12.5%), Tg ≥0.1ng/mL but <1ng/mL (30%) and Tg <0.1ng/mL (57.5%). 41.67% were intermediate-risk patients, 80.39% (n = 40) were treated with RIA, Tg ≥1ng/mL (2.5%), Tg ≥0.1ng/mL but <1ng/mL (17.5%) and Tg <0.1ng/mL (80%); other 24.39% (n = 10), Tg ≥0.1ng/mL but <1ng/mL (80%) and Tg <0.1ng/mL (20%). 14.17% were high-risk patients, 82.35% (n = 14) were treated with RIA, Tg ≥1ng/mL (7.14%), Tg ≥0.1ng/mL but <1ng/mL (28.57%) and Tg <0.1ng/mL (64.29%); other 17.65% (n = 3), Tg ≥1ng/mL (33.33%) and Tg <0.1ng/mL (66.66%). 25% patients (n = 30, 90% in low-risk, 3.3% in intermediate-risk and 6.7% in high-risk) with Tg = 0.04ng/mL, but anti-thyroglobulin antibody levels range from 118 to 3014IU/mL (mean, 537.5IU/mL). Another 1 patient in low-risk with Tg = 0.34ng/mL and Tg-Ab = 139.2IU/mL. While the anti-thyroglobulin antibody level decreased during the follow-up without any treatment in 3 patients.
Total thyroidectomy and lymph node dissection might improve the prognosis of DTC. Even there is 15% patient with Tg ≥1ng/mL, and other 25% with rising antibody levels, but no evidence of recurrence or metastasis from neck ultrasound scan at the final follow-up, so no recommend for further operation or RIA intervention to the biochemical incomplete response with negative imaging patients.
Tg level in DTC patients 5years after TT w/o RIA
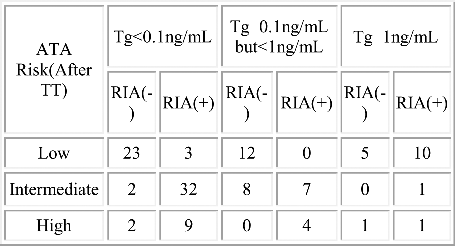
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
The intra-and postoperative complications resulting from giant thyroid gland tumors(Diameter >10cm)surgeries present serious challenges to patient restoration. Although numerous methods can be used, they all have their own limitations. In this paper, we present our experience with several complications of operation treatment on giant thyroid gland tumors to help expand the awareness and prevention of how these complications happened. 143 consecutive patients who underwent operation treatment in Henan Tumor Hospital from 2001 to 2015 were retrospectively analyzed. Statistics pertaining to the patients' clinical factors were gathered.
We found that the most common surgical complications were recurrent laryngeal nerve (RLN) injury and symptomatic hypoparathyroidism. Other complications included incision site infections, bleeding, infection and chyle fistula, the incidence of which increased significantly with increasing extent of surgery from group I (near-total thyroidectomy) to group V (total thyroidectomy plus lateral neck dissection).
Low complication rates may be achieved with more accurate knowledge of the surgical anatomy, skilled surgical treatment and experience. More extensive surgery results in a greater number of complications.
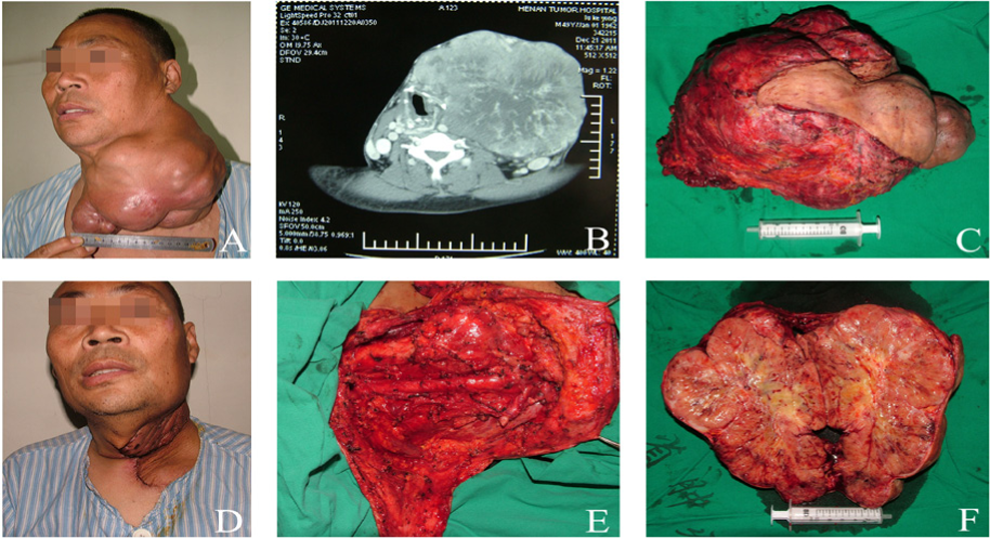
Giant thyroid papillary carcinoma (History, 11 years; diameter of tumor, 21 cm; weight of tumor, 4,200 g; hospital stay, 12 days; surgery time, 185 min). (A) Preoperative giant thyroid papillary carcinoma, causing dyspnea and limitation of movement. (B) Preoperative computerized tomography scans showing oppressed trachea. (C and F) Specimen of giant thyroid papillary carcinoma was solid. (D) Stitches after 8 days showing flap edema with no significant contour deformity. (E) Neck dissection was completed with internal jugular vein ligation.
Thyroid Cancer Wednesday & Thursday Short Call Posters Translational
Papillary thyroid cancer (PTC) presents a recurrence rate of 15–25%, increasing the risk of morbidity and mortality. The use of the BRAFV600E and RET/PTC1 as biomarkers to predict recurrence is still controversial, where the lack of consistent evidence may be due limitations of the analysis approaches. Conditional Bivariate Analysis (CBVA) and Linear Discriminant Analysis (LDA) are data mining strategies that provide an alternative approach to analyze continuous independent variables, identifying subgroups of patients which may have greater recurrence risk. We present a BRAFV600E - RET/PTC1 gene classifier that predicts the M-2009-RSS in patients with PTC.
A total of 112 samples from patients with PTC were prospectively collected. The presence and expression of BRAFV600E and RET/PTC1 were analyzed by HRM and qPCR, respectively. The association of these biomarkers with lymph node metastases (LNM), extrathyroidal extension (ETE) and recurrence risk based on the M-2009-RSS was determined by univariate (UVA), CBVA and multivariate analysis (MVA). Data from high-risk subgroups identified by CBVA was used to develop a gene classifier by LDA.
In UVA and MVA, the presence or expression levels of BRAFV600E and RET/PTC1 were not associated to increased risk of LNM, ETE or being intermediate/high risk according to the M-2009-RSS. CBVA identified select subgroups of patients with high risk for central LNM and tumor size >2cm (OR 10.5 and 12.0, respectively, p < 0.05,) (Table 1). Additionally, specific molecular subgroups showed an increased risk for being intermediate/high risk according to the M-2009-RSS (OR 16.8 for all, respectively, p < 0.05) (Table 1). In a training set, a gene classifier identified intermediate/high risk patients with AUC 0.96, sensitivity of 93% and specificity of 80%, which was reproduced in the independent testing set with AUC of 0.95, sensitivity of 93% and specificity of 76%.
CBVA identifies select subgroups with increased probability of intermediate/high risk of recurrence based on the presence and expression of BRAFV600E and RET/PTC1. A gene classifier trained with this data is able to accurately identify intermediate/high risk patients by analyzing sex, age, BRAFV600E and RET/PTC1.

Thyroid Cancer Wednesday & Thursday Short Call Posters Translational
Mutant BRAF cell lines derived from poorly differentiated thyroid carcinoma variants have been shown to have alterations in Snail and E-cadherin, molecules relevant in epithelial- mesenchymal transition (EMT). Studies on the interaction between BRAF and these molecules in vivo in papillary thyroid carcinoma (PTC), the most common histopathologic variant, are limited. Given this, we sought to elucidate the relationship between BRAF, Snail, E-cadherin and established histopathologic prognosticators in PTC.
In this IRB approved cross-sectional study, archived PTC tissue samples were retrieved. A total of 50 cases (25 BRAF mutant and 25 BRAFWT) met criteria for inclusion in the study. All cases were immunohistochemically stained for Snail and E-cadherin protein expression. A semi-quantitative scoring system (incorporating proportion and intensity) was utilized. To ascertain the clinical correlates of BRAF mutational status, Snail expression, and E-cadherin expression, separate (bivariate analyses) chi-square tests of independence were used if expected cell counts were greater than 5.
Snail and E-cadherin expression were noted in 44% and 84% of BRAF mutant and, in 29% and 95% of BRAFWT samples, respectively. No statistically significant correlations were noted between Snail, E-cadherin and histopathologic prognosticators. However, a trend was noted between Snail expression and tumor size <5 cm (p = 0.07). Statistically significant differences between BRAF mutant and BRAFWT samples were noted in the tall cell histopathologic variant (32% vs. 0%), extrathyroidal extension (32% vs. 5%), infiltrative growth pattern (80% vs. 48%), presence of desmoplasia (72% vs. 29%), psammona bodies (48% vs. 10%), and cystic change (32% vs. 5%). Compared to BRAF mutant samples, BRAFWT samples were more commonly of the encapsulated follicular variant of PTC (52% vs. 4%) (p < 0.001).
Our findings, confirming the association between adverse prognosticators and BRAF mutations in PTC, suggest that the interaction between BRAF and EMT in PTC is not through induction of the Snail/E-cadherin pathway. Investigation of other molecules in the tumor microenvironment might provide further insights into the relationship between BRAF and EMT.
Thyroid Cancer Wednesday & Thursday Short Call Posters Translational
TERT promoter mutations have been recently described in adult thyroid cancer (TC) but not yet in the uncommonly occurring pediatric TC. Also, the role of BRAFV600E mutation in the clinical outcome of pediatric TC is unknown. We investigated the two reported TERT promoter mutations C228T and C250T and BRAFV600E mutation in a relatively large pediatric TC cohort and compared the results with those of a large adult TC cohort from the same population.
The study included 55 pediatric and 210 adult TC patients from the same ethnic background in the same time period. The demographic, clinicopathological features and mutation status are summerized in Table 1. Genomic DNA was isolated from formalin-fixed paraffin-embedded TC tissues, amplified by PCR and subjected to direct sequencing for TERT promoter and BRAFV600E mutations. Genetic-clinicopathological correlations were analyzed using the Chi-Square and Fisher Exact test for categorical variables and T test for numerical variables (Table 1).
Only a single case of pediatric TC was found to harbor the C228T TERT promoter mutation (1.8%). C228T and C250T mutations were not detected in any of the remaining 54 pediatric TC (Table 1). In contrast, there was a significantly higher rate of TERT promoter mutations in the adult patients (15.7%, 33/210) compared with the pediatric patients (P = 0.003). Comparing tumors harboring BRAFV600E mutation with those harboring wild-type BRAF in the 55 pediatric patients revealed no difference in tumor size, multifocality, extrathyroidal invasion, lymph node metastasis and distant metastasis. However, persistent/recurrent TC was seen in 8/12 (66.7%) pediatric patients harboring the BRAFV600E mutation versus 14/43 (32.6%) patients harboring the wild-type BRAF (P=0.047) and, when only conventional papillary TC was examined, in 7/9 (77.8%) cases harboring BRAFV600E mutation versus 11/33 (33.3%) cases harboring wild type BRAF (P = 0.025).
This is the first study on TERT promoter mutations in pediatric TC, which revealed an exceedingly low prevalence, suggesting a limited role of these mutations in pediatric TC. This study also for the first time demonstrates an association of BRAFV600E mutation with TC recurrence in the pediatric patients.
Histopathological features and mutation status of 55 pediatric and 210 adult TC

Thyroid Hormone Action Wednesday & Thursday Short Call Posters Basic
Thyroid gland stimulation in response to food availability occurs via leptin induction of thyrotropin releasing hormone (TRH) and thyroid stimulating hormone (TSH). Herein, we have shown that food availability also upreguates type II deiodinase (D2) thereby increasing thyroid hormone action as measured through the conversion of T4-T3.
Using mouse skeletal muscle and a mesothelioma cell line (MSTO211H) as models, we show that D2 is transcriptionally upregulated when transitioning from fasting to refeeding or switching from 0.1 to 10% FBS, respectively.
The underlying mechanism is the transcriptional de-repression of DIO2 through the mammalian target of rapamycin complex 2 (mTORC2) signaling pathway as defined through lentiviral knockdown of its essential component, rictor. FOXO1, a downstream target of mTORC2, transcriptionally represses DIO2; this was determined using its specific inhibitor AS1842856 and through adenoviral infection of constitutively active FOXO1. These results were confirmed by ChIP studies indicating that 4h after exposing MSTO211H cells to 10% FBS-containing media, FOXO1 binding markedly decreases and the DIO2 promoter is activated. Studies in the insulin-receptor FOXO1 KO mouse indicate that insulin is a key signaling molecule in this process, yet, similar results were found using IGF-1 as a stimulant.
We conclude that FOXO1 represses DIO2 during fasting and de-repression occurs via nutritional activation of the PI3K-mTORC2-Akt-FOXO1 pathway.
Thyroid Hormone Metabolism & Regulation Wednesday & Thursday Short Call Posters Clinical
The U.S. Food and Drug Administration requires that manufacturers of over-the-counter (OTC) supplements ensure the safety of their products. In this paradigm, nonprescription weight loss products have become increasingly popular and include products with potentially misleading claims to target obesity. Notably, thyroid hormone, a prescription medication, has previously been identified in several nonprescription supplements marketed for “thyroid support.” Exogenous thyroid hormone is a medication prescribed to individuals with hypothyroidism that, in excess, may result in thyrotoxicosis, the effects of which include weight loss, cardiac arrhythmias, and bone loss. In this study, we tested the hypothesis that OTC dietary supplements marketed for weight loss also contain measurable quantities of thyroid hormone (thyroxine (T4) and/or triiodothyronine (T3)) that may be clinically significant.
We performed a survey of popular OTC weight loss supplements available at large-volume U.S. retailers, focusing on products that were popular either by online consumer ratings or shelf placement in stores. Twenty-nine OTC weight loss supplements were purchased for the quantification of T4 and T3 content by high performance liquid chromatography. T3 and T4 were measured in duplicate, with all measurements differing by <15% for each product. The reported content is the mean of these paired measurements and reported at the manufacturer's recommended daily dose.
Nine of 29 (31%) of the products contained thyroid hormone. Five products (17%) contained only T3, four (14%) contained both T4 and T3, and no products contained only T4. Of the nine products containing thyroid hormone, mean T4 content was 20.2 ± 9.0 mcg/day (n = 4; range 9.6–29.6), and mean T3 content was 22.4 ± 21 mcg/day (n = 9; range 2.8–66.6) based on manufacturers' recommended dosing.
Nearly one-third of the sampled nonprescription U.S. weight loss products contain unlabeled thyroid hormone content in doses that may result in clinically significant thyrotoxicosis. Increased regulation is needed to ensure the safety of consumers ingesting nonprescription weight loss aids.
Thyroid Hormone Metabolism & Regulation Wednesday & Thursday Short Call Posters Clinical
Subtle alterations in thyroid homeostasis indices, namely increased Thyroid Stimulating Hormone (TSH), triiodothyronine (T3), and T3: thyroxine (T4) ratio, have been associated with cardiometabolic risk factors such as obesity, lipid status, and blood pressure in euthyroid adults, but these relations are less established in youth. We assessed whether TSH, free T3 (fT3), and fT3: free T4 (fT4) ratio correlate with these same risk factors in a large, representative sample of euthyroid adolescents in the U.S.
Participants aged 12–19 years in the cross-sectional NHANES database, 2007–2010, were studied. Inclusion criteria: normal TSH (reference range, 0.35–5.6uIU/ml) and negative thyroid peroxidase antibodies (≤9.0 IU/ml); exclusion criteria: history of thyroid disease; pharmacologic treatment for hypertension or dyslipidemia; HgA1c ≥ 6.5%, fasting serum glucose ≥126 mg/dl, or serum glucose ≥200 mg/dl two hours after an oral glucose load. Univariate and multivariate analyses were performed on TSH and thyroid hormones vs. BMI Z-score, blood pressure, serum lipids, and glucose homeostasis indices, with a stated significance level of <0.001 to account for multiple comparisons. In the multivariate analysis, data were corrected for age, sex, and race.
1167 euthyroid adolescents (mean age 15.0 ± 1.91 years, 53.0% male) were included in the analysis; means for TSH = 1.60 ± 0.83 uIU/ml, fT3 = 3.65 ± 0.45pg/dl, and fT4 = 0.79 ± 0.12 ng/dl. Compared with healthy weight and overweight adolescents, adolescents with obesity had higher fT3:fT4 ratio (F-ratio 10.75, p < 0.0001). Univariate analyses showed significant positive linear associations between fT3:fT4 ratio and BMI Z-score, triglycerides, fasting insulin, blood glucose 2 hours after a 75 gram (or adjusted dose, for subjects weighing ≤40.9kg) oral glucose tolerance test, and insulin resistance as assessed by HOMA-IR. Subsequent multivariate analyses indicated that relations between fT3:fT4 ratios and fasting glucose and HOMA-IR remained significant after controlling for age, sex, race, and BMI.
In euthyroid U.S. adolescents, higher fT3:fT4 ratios are positively correlated with multiple cardiometabolic risk factors, even independent of age, sex, race, and degree of obesity.
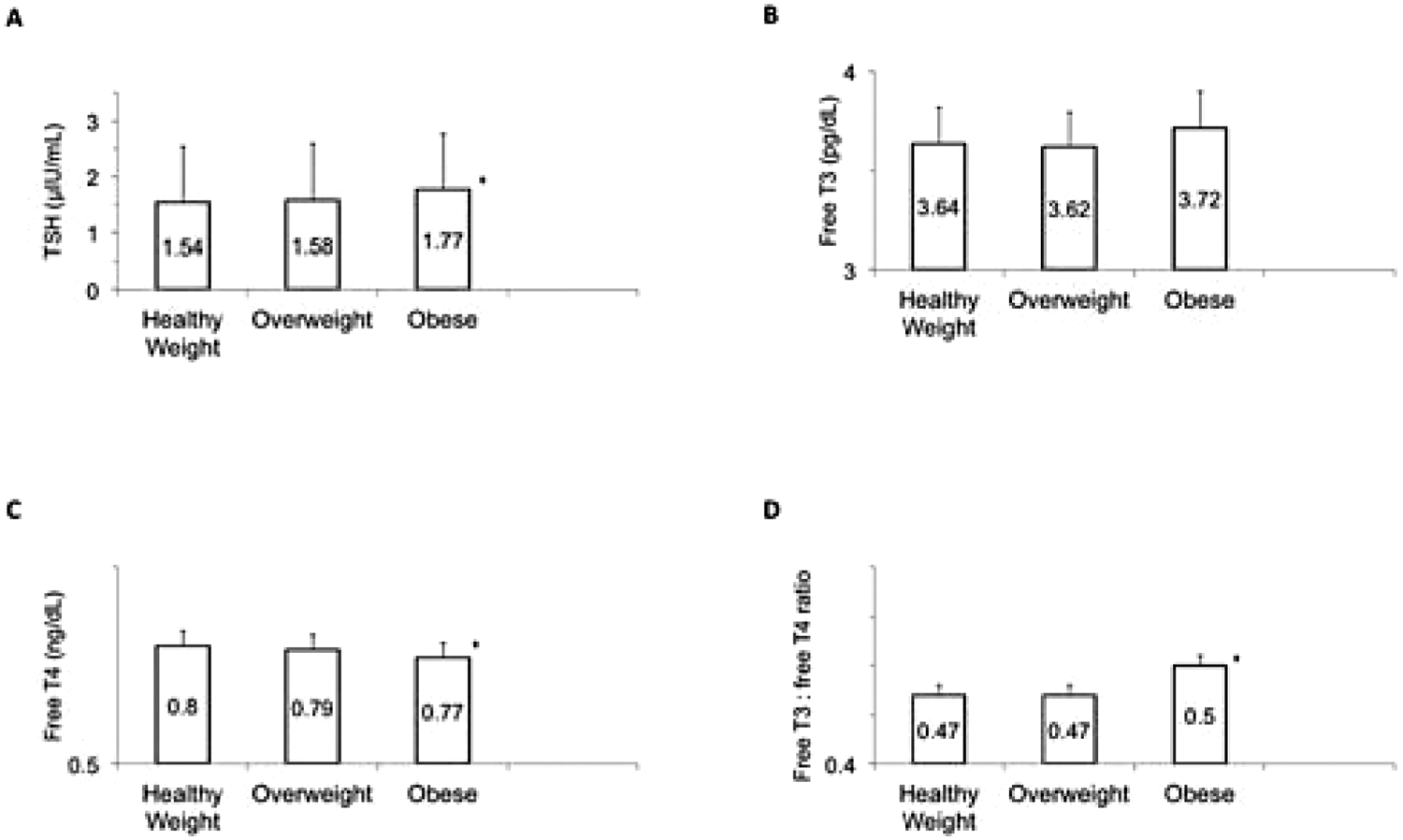
Thyroid homeostasis indices by category of healthy weight, overweight (BMI from 85th to 94th percentile for age and sex), or obese (≥ 95th percentile for age and sex); mean value for each category is reported in the columns. A. TSH was significantly higher in adolescents with obesity, when compared with both healthy weight and overweight subjects (F-ratio 7.04, p = 0.0009) B. There was no difference in free T3 levels by weight category. C. Mean free T4 levels were significantly lower in obese than in healthy or overweight subjects (F-ratio 6.22, p = 0.0019). D. Obese adolescents had a higher free T3: freeT4 ratio than healthy weight or overweight adolescents (F-ratio 7.81, p = 0.0004).
Thyroid Cancer Wednesday & Thursday Short Call Posters Clinical
Although previous studies suggested a potential value of preablative stimulated Tg (ps-Tg) on predicting recurrent and persistent diseases of differentiated thyroid cancer (DTC), its correlations with radioiodine therapeutic response remain uncertain. We aim to correlate the ps-Tg level with therapeutic response after a median follow-up of 38 months after initial therapy, and analyze a cut-off ps-Tg threshold for indicating a poor response.
A total of 452 DTC patients were followed for a minimum follow-up of 2 years after total thyroidectomy and RRA. After 2-year follow-up, clinical outcomes were assessed based on Memorial Sloan Kettering Cancer Center (MSKCC) response (excellent, acceptable, incomplete), and those patients were divided into four groups in terms of their ps-Tg level: Group1: ps-Tg<1ng/ml (n = 82), Group2: 1ng/ml≤ps-Tg<5ng/ml (n = 119), Group3: 5ng/ml≤ps-Tg<10ng/ml (n = 55), Group4: ps-Tg ≥10ng/ml (n = 196).
Patients with lower ps-Tg level (<10 ng/ml) had better response, especially for those with ps-Tg<1 ng/ml, none of whom had incomplete response. In addition, 100% of Group1, 93.28% of Group 2, 83.64% of Group 3 and 33.16% of Group 4 had either excellent or acceptable response (χ2 = 185.073, p < 0.001) (Fig. A). Clinical outcome of Group 3 was poorer than that of Group 2 (χ2 = 3.966, p = 0.046). A cut-off value of ps-Tg at 13.35 ng/ml was obtained by receiver operating characteristic (ROC) curve for differentiating incomplete response from excellent or acceptable response, with corresponding specificity of 0.868, sensitivity of 0.858, area under curve (AUC) of 0.922, positive predictive value (PPV) of 76.05% and negative predictive value (NPV) of 92.63% (Fig. B). Ps-Tg was an independent predictive variable of incomplete response (OR: 33.281, p < 0.001).
Ps-Tg has a great performance in predicting therapeutic response after 2-year follow-up and provides incremental value for radioiodine decision making.

Thyroid Hormone Metabolism & Regulation Wednesday & Thursday Short Call Posters Clinical
To investigate the rate of TSH change and its variation tendency following thyroxine withdrawal (THW) in patients with distant metastatic differentiated thyroid cancer (DTC) before radioiodine therapy (RIT) or scintigraphy.
A total of 97 patients with successful thyroid ablation were divided into M1 (n = 30) and M0 (n = 67) according to the presence of distant metastasis (DM) or not. TSH levels were obtained at three time points for each patient: once before THW(TSH0) and twice at 20d and 27d after THW(TSH1, TSH2), respectively. The changing rate from TSH0 to TSH1 and TSH1 to TSH2 were denoted as V1 and V2, respectively. The changing ratio between V1 and V2 was marked as R (R = (V2-V1)/V1) and compared between M0 and M1.
M0 and M1 did not differ in V1 (P > 0.05), while M1 showed a significantly lower V2 than M0 (3.68 ± 4.33 vs 7.67 ± 3.66; P = 0.001). M1 and M0 demonstrated completely different variation tendencies in TSH changing after THW, with significantly different R values (Z = -4.17>P <0.05)(Fig.1). TSH increased doubly in most patients of M0 (90.7%) compared with only 41.2% of M1. Furthermore, TSH level tended to decrease in 23.5% of M1, while none of M0 presented such decreasing manner.
Compared with patients without distant metastases, those with distant metastatic DTC displayed a slower TSH increasin or even decreasing tendency over time after THW. More attention should be paid to the variation of TSH after THW in patients with distant metastases, to avoid probable inefficiency of RIT induced by the decrease of TSH.
Thyroid Imaging Wednesday & Thursday Short Call Posters Clinical
Whole body 18F-FDG PET/CT (PET/CT) is an accepted tool for investigation of Differentiated Thyroid Cancer (DTC) with high thyroglobulin (Tg) levels and negative whole body iodine scan (IWS). The rational is that undifferentiated tumors loose the capacity of iodine uptake, but remain producing Tg that work as an specific tumoral marker. At the same time, these tumors tend to me more aggressive and have increased glucose metabolism. Several papers have showed that stimulation with recombinant human TSH (TSHhr) may increase the sensibility of the PET/CT scan.
We studied retrospectively 25 patients with DTC (23 Papillary and 2 Follicular) submitted to TSHhr stimulated PET/CT and Tg measurement. All patients had negative IWS and were free of Tg antibodies. In 24 patients, stimulated Tg levels were elevated (above 1ng/dl).
PET/CT showed uptake at the thyroid bed In 4 patients (14,3%), at cervical lymph nodes in 17 patients (60,7%) and at distant sites in 7 (25%). The distant sites of uptake were at lymph nodes (4 mediastinal, 1 axillar and 1 abdominal), and bone in 1 individual. None of the PET/CT studies resulted negative. Tg levels varied from 0,2 to 965 ng/dl (mean 52,7 ng/dl). The SUV max (Maximum Standardized Uptake Value) at the lesions varied from 1,7 and 4,8 (mean 2,8).
We conclude that TSHhr PET/CT is a valuable tool in finding suspicious lesions in patients with high thyroglobulin levels and negative IWS.
Thyroid Imaging Wednesday & Thursday Short Call Posters Clinical
Normal thyroid gland usually does not show significant FDG uptake. Therefore, any increase of glucose metabolism is considered abnormal. Incidental thyroid FDG uptake on routine 18F-FDG PET/CT (PET/CT) is found on 2% of the cases, representing inflammatory or tumoral disease.
We retrospectively identified 100 patients (22 M, 78 F, age from 29 to 91, mean 64,2 Y) in a total of 4562 (2,2%) submitted to PET/CT in our institution from 2009 to 2015, with incidental findings on the thyroid classified on two categories: diffuse uptake (38%) and focal uptake (62%), with detectable nodules (38%) or without anatomic correlation on non contrast CT (24%).
All patients with diffuse uptake had clinical and laboratorial diagnosis of thyroiditis. In the group with focal uptake, 18% correlated with thyroiditis, 21% had confirmed diagnosis of differentiated thyroid cancer (DTC) as a second primary malignancy and in 23%, benign thyroid nodules were identified. In our casuistic, all 21 patients with malignancy were diagnosed with primary DTC, but it is important to emphasize that thyroid tumor, primary or metastatic can also present with a diffuse uptake pattern.
We conclude that incidental findings of hypermetabolism on thyroid should be investigated due to the high incidence of malignancy.
Thyroid Nodules & Goiter Wednesday & Thursday Short Call Posters Basic
To study the morphological change, pathologic diagnosis and curative effect evaluation in radiofrequency ablation of thyroid nodules.
The patients with thyroid nodules from May 2015 to June 2015 in our hospital. Preoperative routine examination and clinical laboratory tests to check the diagnosis of thyroid nodules with a diameter of about 30–40mm. Through our hospital ethics committee, the patients' thyroid nodules were removed or thyroid gland lobectomy. Then the specimens were treated with radiofrequency ablation: half of the routine pathological tissue sections were prepared, and half of the specimens were made from the transmission electron microscope (TEM).
1. Routine pathological (HE staining) display: Along the radiofrequency ablation needle(Fig.1: Arrow) has obvious cell necrosis area, eosin staining, and the nucleus of the follicular epithelium was absent, and a large number of lymphocytes infiltrated. Gradually outward from the needle path we found the morphology of thyroid follicular epithelial cells was observed to be normal. The morphology of the follicular cells was small, and other was no differences. 2. TEM(Fig2): Along the ablation needle to the outside, two adjacent follicular epithelial cells line can't recognize; Discovery of follicular epithelial cell nuclear pyknosis dissolved, nuclear membrane rupture, euchromatin(Four angle star)disintegrating, heterochromatin(Five-pointed star)clumps. Rough endoplasmic reticulum(Pentagon) was empty pool shaped degeneration and expansion. Intracellular organelles (Mitochondria(Arrow), Golgi body, etc.) fuzzy cannot identify, mesenchymal stromal cells disintegrating, collagen fibers swelling, collapse, fracture or liquefaction. Rarely see lysosomal and lysosome devouring organization become autophagosome dead cells.
First after radiofrequency ablation of thyroid pathological tissue structure and cell morphology is also the basic existence, the pathological diagnosis of thyroid diseases will not be affected. Second the structure of thyroid follicular cells was severely damaged by the transmission electron microscope, and the 3 stage necrosis was achieved. It shows that the effectiveness of radiofrequency ablation surgical treatment of thyroid nodule.
Routine Pathological and Transmission Electron Microscope

Thyroid Nodules & Goiter Wednesday & Thursday Short Call Posters Clinical
Molecular testing (MT) of nodules classified as Bethesda category IV follicular neoplasm (FN) can refine cancer risk estimation. Currently 3 MT modalities have clinical utility in FN nodules: gene expression classifier (GEC), 7-gene molecular panel (7G-MP), and next-generation sequencing based ThyroSeq 2.0 (NGS). Depending on cancer prevalence and test performance, MT results can be used to guide extent of initial surgery and/or facilitate active surveillance. Our study aim was to compare the costs of nodule management using molecular-guided algorithms to the costs of standard of care (SC) without MT.
To estimate the costs of nodule management per ATA guidelines using SC, GEC, 7G-MP, or NGS, a decision tree model was constructed for adult patients who had a solitary nodule ≥1 cm with FN cytology. Cancer prevalence, test sensitivities and specificities were based on comprehensive review of recent literature. Costs of surgery included inpatient hospital costs from the Healthcare Costs and Utilization Project and accounted for a proportion of outpatient surgeries as well as for costs of surgical complications. Estimates for postoperative care and active surveillance were based on median 2015 Medicare Reimbursement rates and included physician fees, outpatient tests, and medications. The main outcome measure was cumulative per patient cost extending 10 years from FN diagnosis.
In the base-case analysis, the average per patient cost of SC was $11,505 (range $10,676-$12,347). An increase in the average per patient cost of nodule management was observed with both GEC ($13,027, range $12,373-$13,666) and 7G-MP ($12,029, range $11,254-$12,823). However, NGS-guided care was associated with a substantially lower cost (average per patient $7,683, range $7,174-$8,333). After varying FN malignancy rate, test costs, and test parameters in sensitivity analysis, no changes were seen in the cumulative cost reduction observed with NGS compared to SC, GEC, and 7G-MP.
Due to high test sensitivity (90%) and specificity (93%), NGS-guided algorithm for FN nodules are predicted to result in an estimated 30% reduction in the average per patient cost of nodule management.
Thyroid Nodules & Goiter Wednesday & Thursday Short Call Posters Clinical
TIRADS and BSRTC have been widely used for interpretation of ultrasound and FNAC results. BRAFV600E analysis is a new molecular tool in diagnosing thyroid malignant nodules. This study was to compare the diagnostic value of the three methods in differentiating thyroid nodules and evaluate the diagnostic efficiency of different combinations.
220 nodules of 220 patients that underwent FNAB were enrolled in this prospective study. All patients underwent ultrasound examination, FNAC and BRAFV600E analysis. The interpretation of ultrasound and FNAC were based on TIRADS classification and BSRTC accordingly. BRAFV600E detection was analyzed with the amplification refractory mutation system (ARMS) technique. Receiver operating characteristic curves were conducted to compare the diagnostic value.
220 patients were included with 177 females and 43 males. The mean age was 44.91 ± 13.65. Those nodules with positive cytology (BSRTC IV, V, VI) or BRAFV600E mutation, presence of compressive symptoms, or negative cytology but with increase in size or changes in ultrasound features during follow-up were treated with surgery and validated pathologically. The remaining 61 nodules were included in the observation group. According to final histopathology or follow-up results, the sensitivity, specificity and area under curve (AUC) of TIRADS were 73.1%, 88.4%, 0.808. BSRTC had higher specificity (97.7%) and similar sensitivity (77.6%) compared with TIRADS. The sensitivity, specificity and AUC of BRAFV600E (85.1%, 100%, 0.925) were the highest among the three methods. Combinations of different methods could increase the diagnostic sensitivity and accuracy. The combination of BSRTC and BRAFV600E significantly increased the diagnostic efficiency, with 97.8% sensitivity, 97.7% specificity and 0.977 AUC. In patients with negative cytology results (BSRTC I-III), the mutation rate of BRAFV600E was 64.5% in US-positive nodules compared with 8.4% in US-negative nodules (P < 0.001).
The combination of BSRTC and BRAFV600E bears a great value in differentiating thyroid nodules. The TIRADS classification is useful in selecting patients for FNAB and patients with negative cytology results for BRAFV600E analysis.
Thyroid Nodules & Goiter Wednesday & Thursday Short Call Posters Clinical
The accurate diagnosis of thyroid nodules continues to challenge physicians managing patients with thyroid disease. Patients with cytologically indeterminate nodules are often referred for diagnostic surgery, though most of these nodules prove to be benign. This limitation of FNA cytology underscores a clinical need for reliable pre-operative molecular markers to distinguish benign from malignant thyroid nodules. MicroRNAs constitute a class of short, non-coding RNAs that play key roles in the regulation of gene expression. MicroRNA expression profiling has been shown to be a reliable method for cancer subtype classification. We present here the development and validation of a microRNA- based test that can stratify thyroid lesions as “benign” or “suspicious for malignancy” in pre-operative Fine Needle Aspirate (FNA) stained smears.
Over five hundred thyroid FNA samples preserved as stained smears, representing various histological subtypes, were used for the assay training and validation. Using proprietary protocols, high-quality RNA was extracted from the samples and the expression levels of a set of 24 microRNAs, discovered through microarray studies, were measured using qRT-PCR. A classifier was developed to utilize the information of the microRNA expression patterns for distinguishing benign from malignant thyroid nodules. The performance of this assay was assessed in an independent, blinded validation set.
The developed assay accurately differentiates benign from malignant thyroid nodules in indeterminate FNA smears, based on the expression of 15 microRNAs. The results of a comprehensive clinical validation study using an independent, blinded set of over 200 samples will be presented, including inter-laboratory concordance data.
Previous studies have demonstrated the potential use of microRNAs for the classification of thyroid nodules. A first-of-its-kind assay utilizing microRNA expression in FNA from smears for distinguishing benign from malignant thyroid nodules was developed. This assay displays high levels of accuracy and will provide an important reliable diagnostic test for the classification of pre-operative thyroid samples.
Thyroid Nodules & Goiter Wednesday & Thursday Short Call Posters Clinical
Thyroid nodules radiofrequency ablation is more and more used in clinical. Heat injury of recurrent laryngeal nerve is one of bottlenecks of the technology promotion.
There are 120 cases of thyroid benign nodules, monitor used 90 pts. and no 30 pts. Local infiltration anesthesia, the no-monitor group were been treated use conventional puncture technique to protect the recurrent laryngeal nerve in thyroid nodules radiofrequency ablation guided by ultrasound. The temperature puncture probe firstly was placed trachea esophagus nearby the recurrent laryngeal nerve and monitors real-time temperature during thyroid nodules radiofrequency ablation in monitor group.
In the no-monitor group, there are 4 patients the recurrent laryngeal nerve palsy occurred and all had recovered from 1 to 3 months. The monitor group 2 patients had, 1 patient from monitor probe to the ablation needle less than 3mm, the measured temperature was 100°C another patient was less than 5mm, 84°C. In other study, the thermal damage of sciatic nerve in rats was found to be changed at 45°C, and the signal was gradually attenuated with increasing temperature, and the signal was completely disappeared at 74°C.
The temperature sensitive detection device can be used for the real-time monitoring of the tissue temperature in thyroid nodule radiofrequency ablation. It should be showed lower than 74°C that the temperature of trachea esophageal groove placed in the temperature sensitive puncture probe, and the needle of radiofrequency ablation should be greater than 5mm, can ensure the recurrent laryngeal nerve from heat damage.