
Abstract
Background:
The use of calcitonin screening for the rare medullary thyroid cancer (MTC) is controversial due to questions of efficacy, accuracy, and cost-effectiveness. This study reports the results of a large prospective validation using a machine-trained algorithm (MTC Classifier) to preoperatively identify MTC in fine-needle aspiration biopsies in lieu of calcitonin measurements.
Methods:
Cytology analysis on a prospective consecutive series of 50,430 thyroid nodule biopsies yielded a total of 7815 indeterminate (Bethesda categories III/IV) cases, which were tested with the MTC classifier. A prospective, consecutively submitted series of 2673 Bethesda III–VI cases with cytology determined locally was also evaluated. RNA was isolated and tested for the MTC Classifier using microarrays.
Results:
Forty-three cases were positive by the MTC Classifier among 10,488 tested nodules (0.4%), consistent with the low prevalence of MTC. Of these, all but one was histologically or biochemically confirmed as MTC, yielding a positive predictive value (PPV) of 98%. Of the positive cases, only 19 (44%) had been specifically suspected of MTC by cytology, highlighting the limitations of light microscopy to detect this disease. Three surgically confirmed MTC cases that were detected by the MTC Classifier had low basal serum calcitonin values, indicating these would have been missed by traditional calcitonin screening methods. A pooled analysis of three independent validation sets demonstrates high test sensitivity (97.9%), specificity (99.8%), PPV (97.9%), and negative predictive value (99.8%).
Conclusions:
A clinical paradigm is proposed, whereby cytologically indeterminate thyroid nodules being tested for common malignancies using gene expression can be simultaneously tested for MTC using the same genomic assay at no added cost.
Introduction
M
Challenges in interpreting cytology result in one-half of MTC cases being missed (5,6). A specific diagnosis of MTC is critical to planning the optimal surgery, which is more extensive than for thyroid nodules in which MTC is not specified.
Unfortunately, many sMTC patients undergo suboptimal preoperative evaluations and initial surgical interventions (6 –8), resulting in additional “completion” surgeries and/or compromised patient outcomes. Appropriate surgery results in fewer local reoperations and more frequent biochemical cure (9). In addition, when MTC is not suspected, more than one-quarter of patients with cytologically indeterminate fine-needle aspiration biopsies (FNABs) do not undergo surgical resection in the short term (10), an approach that would delay the diagnosis and treatment of MTCs missed by cytology (6). Conversely, a false diagnosis of MTC can lead to an overly aggressive surgery (6,11 –13).
Many approaches for improving the preoperative diagnosis of MTC have been suggested, and some implemented, with varying degrees of success. A negative result on a large mutation panel does not adequately exclude sporadic MTC (14,15). As medullary thyroid tumors often overproduce calcitonin, screening for its production, either by immunohistochemistry, or by measurement in the serum, has been a focus of diagnostic efforts. The presence of MTC across all six Bethesda cytopathology categories (6,12,16) requires that any testing paradigm take into account this distribution when testing for MTC, and must be considered against a backdrop of its rarity. Efforts to improve the diagnostic FNAB pathway could include making a cell block on every FNAB and performing immunohistochemical staining for calcitonin on those that are not cytologically benign. This approach is often challenged by insufficient residual cells for production of the cell block, as well as cost given the rarity of MTC. In addition, sMTC seem to be less frequently immunoreactive for calcitonin (74–79%) than familial cases are (100%) (17). Serum calcitonin screening is limited by lack of agreement on the calcitonin threshold to suspect MTC, no prospective randomized studies demonstrating improved patient outcome by calcitonin screening, and questions about cost-effectiveness not only given the rarity of MTC but also because of the downstream effects of false positive results (18 –22). While serum calcitonin screening is accepted in some countries such as Germany and Italy, it is not uniformly accepted in the United States and elsewhere, resulting partly from its high false positive rate (60–90%) and low positive predictive value (PPV) of 10–40% (23). Thus, serum calcitonin screening thresholds with high sensitivity may drive unnecessary MTC-related testing and surgery in patients who do not have MTC.
It was reasoned that if there were a paradigm for testing FNAs from indeterminate nodules, an additional classifier could be incorporated to test for MTC without incurring the expense and effort of a separate test. Recently, machine learning was used to develop an algorithm that uses mRNA gene expression data from thyroid FNAB samples to reclassify cytologically indeterminate nodules as benign or suspicious, with high sensitivity and negative predictive value (NPV). This classification algorithm (Afirma® Gene Expression Classifier [GEC]) uses 142 genes to separate benign and suspicious nodules, but the presence of nearly 3000 genes on the microarray allows future tests to be added by developing algorithms on different gene sets for different diagnostic purposes. This approach was used to develop a classifier for MTC (24,25), and as all genes are measured with one assay on one microarray, the MTC result is generated concurrently with the GEC result at no added cost. The MTC portion of the classifier was trained by analyzing expression data on 22 known MTC cases from 220 surgical tissues, confirmed by histopathology. Using machine learning and feature selection on 283,927 gene transcripts measured in training, a group of five genes was selected (CALCA, CEACAM5, SCG3, SCN9A, and SYT4), which together have high accuracy for detecting MTC (Table 1) (24,25).
The Chudova et al. (25) supplement briefly describes the MTC Classifier training methodology.
Multicenter study utilizing 220 banked surgical tissue samples with local histopathology truth. Pathologists masked to molecular results. Leave-one-out cross-validation. Previously unpublished data. The Alexander et al. (24) supplement lists the genes included in the MTC Classifier.
MTC, medullary thyroid cancer; PPV, positive predictive value; NPV, negative predictive value.
After the MTC Classifier was trained and locked, two independent FNAB sample sets with a combined total of 489 samples were tested to establish clinical validation (Tables 2 and 3) (24,25). Those studies showed high specificity and high NPV of the MTC Classifier. Here, the MTC Classifier is tested on 10,488 thyroid nodule FNAB samples referred for GEC testing from a large prospective clinical series of 53,103 consecutively received thyroid nodule FNABs, the largest cohort tested to date (Fig. 1 and Table 4). A pooled analysis combining all three studies demonstrates exceptionally high diagnostic accuracy (Table 5).
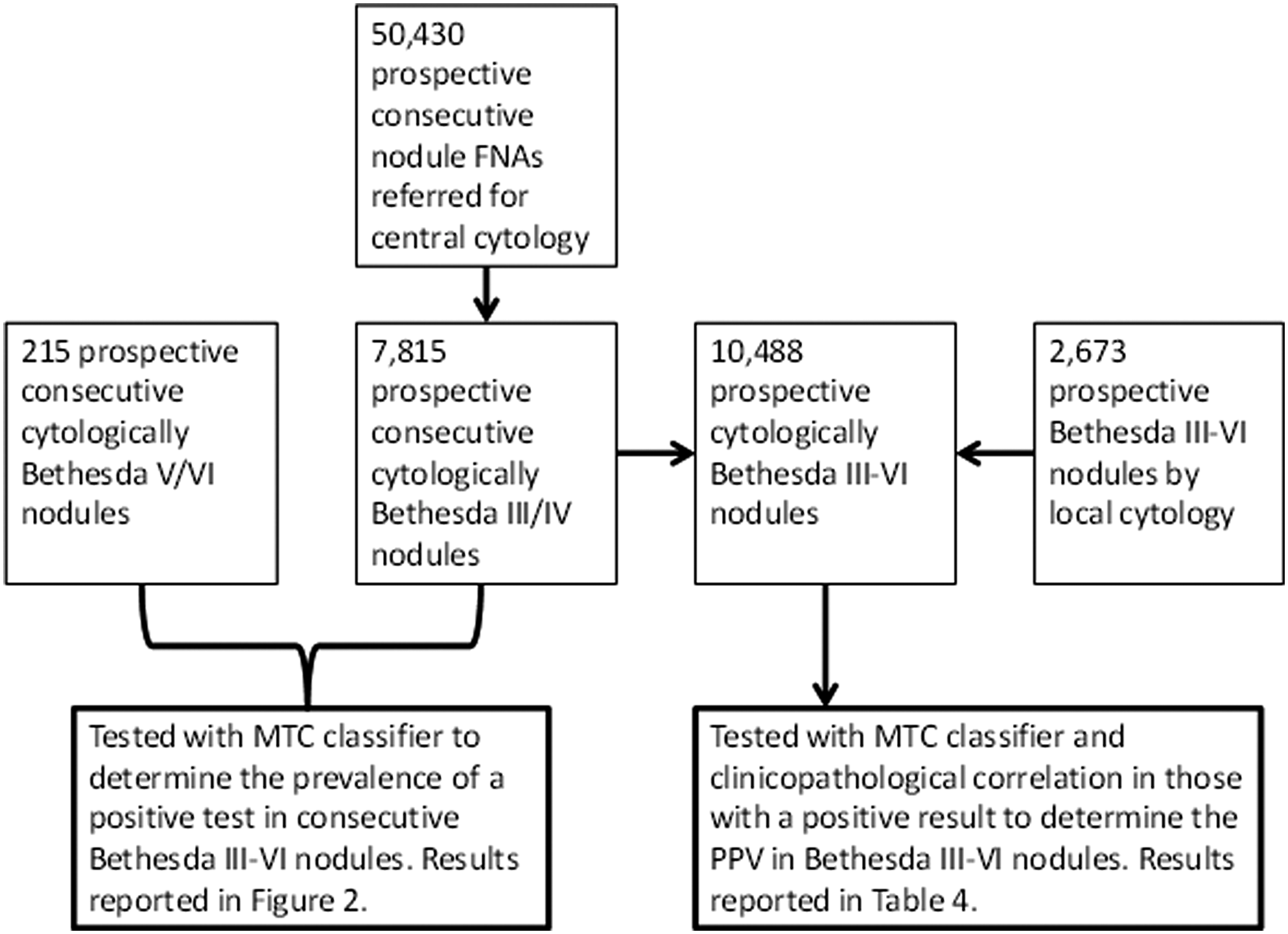
Study design flow diagram.
Prospective, multicenter fine-needle aspiration biopsy (FNAB) samples. Local cytopathology assigned Bethesda I–VI. Truth based on expert by central histopathology expert(s) or local pathologist. Pathologists masked to molecular results. Previously unpublished data.
Prospective, consecutive, multicenter FNAB samples. Local cytopathology assigned Bethesda III–VI by expert cytopathology review of local reports, truth based on expert central histopathology panel review. Pathologists masked to molecular results. Two of the four histologically confirmed MTC cases were excluded from the final analysis in Alexander et al. due to pre-specified exclusions (one for deviation in storage conditions, and one because a contralateral nodule was used for Classifier training) but are included here.
Prospective, consecutively received, multicenter FNAB samples. Local or central cytopathology Bethesda III-VI, truth based on local histopathology (not masked to molecular results or serum calcitonin). As truth was not obtainable on all MTC test negative patients, only PPV is reported.
One false negative case described in this study included the pooled analysis.
Materials and Methods
The Bethesda System for Reporting Thyroid Cytopathology
The six categories in the Bethesda System for Reporting Thyroid Cytopathology are: Bethesda I (non-diagnostic or unsatisfactory); Bethesda II (benign); Bethesda III (atypia or follicular lesion of undetermined significance [AUS/FLUS]); Bethesda IV (suspicious for follicular or Hürthle cell neoplasm [SFN/SHCN]), Bethesda V (suspicious for malignancy), and Bethesda VI (malignant) (26).
Experimental design
This protocol was reviewed and granted Institutional Review Board exempt status (Liberty IRB, DeLand, FL). Patients were prospectively derived from two diagnostic pathways (Fig. 1). The first was centralized cytological evaluation of thyroid nodule FNABs with routine GEC testing for Bethesda III/IV nodules, and testing for Bethesda V/VI nodules only upon physician's request. This process accrued 50,430 thyroid nodules between December 1, 2010, and June 26, 2013, and included 5883 Bethesda III and 1932 Bethesda IV nodules. Second, an additional 2673 GEC samples, mostly from Bethesda III/IV and a smaller fraction from Bethesda V/VI nodules, were submitted mainly from academic centers where cytology was performed locally. All samples from either pathway were prospectively and consecutively tested with the MTC Classifier. The testing was conducted in a blinded manner, with the laboratory personnel unaware of clinical patient information and final histopathologic diagnosis.
Clinical details were collected on all patients who were tested with the GEC, and who either had cytological results suspicious for MTC or diagnostic for MTC, or who tested positive with the MTC Classifier. All clinical information was obtained in compliance with the Health Insurance Portability and Accountability Act from treating physicians by Veracyte Medical Directors under the Clinical Laboratory Improvement Amendments mandate of test result quality assurance. Three patients were found to have Bethesda V/VI cytology with suspicion for MTC, but they did not undergo GEC testing and were excluded from further analysis.
As Bethesda V and VI FNAB samples are not automatically reflexed to GEC testing, the prevalence of positive MTC Classifier results in these two cytopathology categories were examined in a consecutive series of de-identified FNAB samples with Bethesda V (n = 104) and Bethesda VI (n = 111) cytopathology (Figs. 1 and 2).
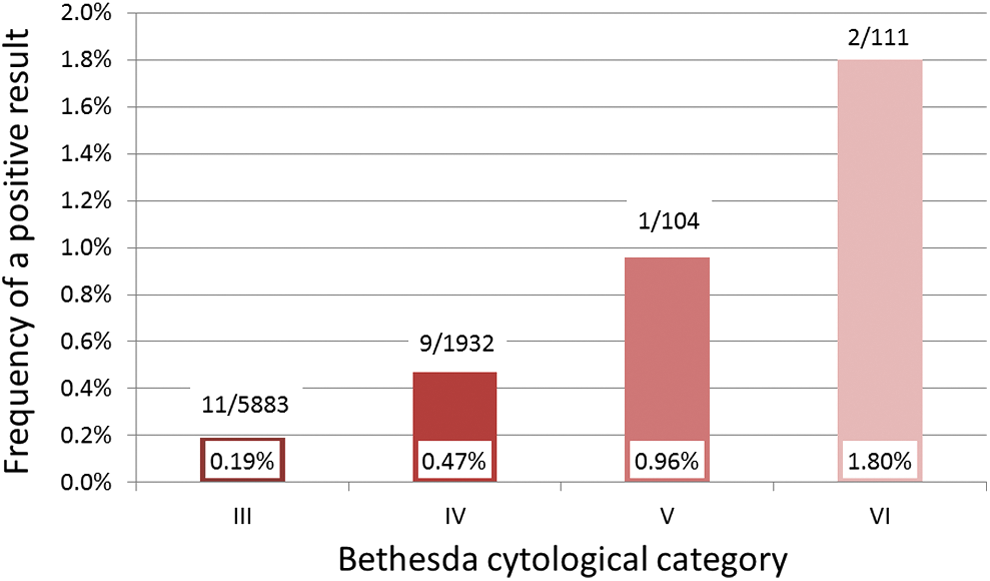
Frequency of an mRNA expression signature suggestive of medullary thyroid carcinoma (MTC) among prospective consecutive nodules by Bethesda category. Values above the bars are those with positive MTC Classifier results over the total number of consecutively tested nodules in that Bethesda category.
Reference standards
Biochemical and rearranged during transfection (RET) proto-oncogene mutation analyses were performed according to local clinical practice. Calcitonin was most often measured with the Siemens (DPC) Immulite 2000 assay with a reported reference range of approximately <2–5 ng/L for women and <2–8.4 ng/L for men. Relevant MTC testing (including measurement of serum calcitonin) was routinely recommended by (a) Veracyte medical director(s) when the MTC Classifier detected the MTC signature. Local surgical pathology served as the gold standard for confirmation of MTC when it was obtained. When surgical pathology was not obtained (three cases), patients with serum basal calcitonin levels >80 ng/L were considered to have MTC, given the high PPV at this cutoff (27 –29). This approach allowed an outcome to be assigned to patients with positive MTC Classifier results. However, an outcome was not assigned to the overwhelming majority of patients with negative MTC Classifier results. Thus, sensitivity could not be calculated on this cohort. Elsewhere, MTC Classifier sensitivity was reported on MTC tissue samples with histologically confirmed truth as 96.3% [confidence interval (CI) 81.0–99.9%] (30). The upper reference range of serum calcitonin in adult women and men is approximately 5.2 ng/L and 11.7 ng/L, respectively (31).
Statistical analysis
The two-sided CI of a proportion was calculated with continuity correction (32).
Results
Bethesda III cytopathology
Among 5883 consecutive prospective thyroid nodules with Bethesda III cytopathology, the MTC Classifier identified 11 cases (0.19%; Fig. 2) as MTC. MTC was confirmed histologically in all cases, except for a 54-year-old female whose surgical histology demonstrated a 1.4 cm intrathyroidal paraganglioma arising within an intrathyroidal parathyroid gland. In another case, a 62-year-old female with a baseline serum calcitonin of 122 ng/L was initially considered to have Hürthle cell carcinoma that was reclassified as an oncocytic variant of MTC with a mixed follicular component upon independent expert histopathology review and ultimately considered an MTC Classifier true positive. Of the 10 histologically confirmed MTC cases, nine had preoperative serum calcitonin results (M = 2018 ng/L; range 122–10,702 ng/L; Fig. 3).

Preoperative basal serum calcitonin values in 40 patients with MTC confirmed by surgical pathology (37 cases) or calcitonin >80 ng/L without surgery. The dashed line at 2 on the log10 scale represents a serum calcitonin value of 100 ng/L, a threshold above which most agree that surgery for suspected MTC is indicated (6,23,33). Red circles encompass the three MTC with preoperative serum Ct <20 ng/L, a threshold commonly considered negative for MTC screening (16,34 –36). Total patients by Bethesda category III–VI were 9, 12, 13, and 6, respectively. The upper reference range of serum calcitonin in adult women and men is approximately 5.2 ng/L (log10 = 0.72) and 11.7 ng/L (log10 = 1.07), respectively (31).
In one Bethesda III case, the cytological description specifically noted that MTC could not be excluded. The GEC result was suspicious, but the MTC Classifier did not detect MTC. Final surgical pathology demonstrated papillary thyroid carcinoma (PTC) surrounded by Hashimoto's thyroiditis.
Bethesda IV cytopathology
Among the 1932 consecutive prospective thyroid nodules with Bethesda IV cytology, the MTC Classifier identified nine cases (0.47%; Fig. 2) as MTC. An additional six cases were prospectively identified by the MTC Classifier from the 2673 specimens whose cytopathology was read locally. Of these 15 patients, one patient refused surgery and had no laboratory testing, and one patient demonstrated sex discordance from that of the reference nodule. These two cases are included in MTC signature prevalence calculations, but are excluded from PPV calculations, given the uncertainty in final surgical pathology. The remaining 13 cases were all confirmed to be MTC with either surgical pathology (12 cases) or calcitonin (one case). Of the 12 patients with surgically confirmed MTC, 11 had preoperative serum calcitonin values (M = 1949 ng/L; range 8–6866 ng/L; Fig. 3). The one patient considered to have MTC without surgical pathology had marked elevations of basal serum calcitonin (11,272 ng/L) and CEA (745.7 μg/L).
Bethesda V cytopathology
Among 104 consecutive prospective and blinded thyroid nodules with Bethesda V cytology, the MTC Classifier was positive in one case (0.96%; Fig. 2). In clinical practice, Bethesda V cases are not routinely tested with the GEC or MTC Classifier. Among Bethesda V cases whose physician requested MTC Classifier testing, 13 cases were positive, and all were confirmed to be MTC with surgical pathology (12 cases) or calcitonin (a 57-year-old female with a serum calcitonin of 88 ng/L without thyroid surgery). In 11/13 cases, the cytology description included suspicion for MTC, while no cytological suspicion was present in two cases. In one of these two cases, a 45-year-old female had a preoperative serum calcitonin level of 5 ng/L, and the biopsied nodule was 1 cm MTC on surgical pathology. In the second case, a 36-year-old female with a preoperative serum calcitonin level of 34 ng/L had a 7 mm MTC on surgical pathology of the biopsied nodule. All 12 patients with surgically confirmed MTC had preoperative serum calcitonin values obtained (M = 1921 ng/L; range 5–6912 ng/L; Fig. 3).
In five Bethesda V cases, the cytological description specifically noted suspicion for MTC, but the mRNA signature did not suggest MTC. None demonstrated MTC on surgical pathology. Surgical pathology demonstrated PTC in one, follicular adenomas in two, and adenomatous nodules in two. Hürthle cell changes were reported in three of the cases. Preoperative serum calcitonin levels, measured in four cases, ranged from <2 to 22 ng/L.
Bethesda VI cytopathology
Among 111 consecutive prospective thyroid nodules with Bethesda VI cytology evaluated in a blinded fashion, the MTC Classifier was positive in two cases (1.80%; Fig. 2). In clinical practice, Bethesda VI cases are not routinely tested with the GEC or MTC Classifier. Among Bethesda V cases, for which the treating physician requested MTC Classifier testing, six cases were positive, and all were confirmed to be MTC by either surgical pathology (five cases) or calcitonin in one case of a 73-year-old female with a serum calcitonin of 7721 ng/L. This latter patient did not undergo thyroid surgery but had MRI findings suggestive of osseous metastases. Additionally, primary hyperparathyroidism suggested the possibility of multiple endocrine neoplasia (MEN) 2A (RET proto-oncogene mutation analysis not available). In all six cases, the cytology description suspected or diagnosed MTC. The five patients with surgically confirmed MTC had preoperative serum calcitonin values obtained (M = 1759 ng/L; range 26–5805 ng/L; Fig. 3).
In three Bethesda VI cases, the cytological description favored MTC, and the GEC was suspicious, but the MTC Classifier was negative. In two of the cases, preoperative serum calcitonin was undetectable, and PTC was found on surgical histology. In the third case, the preoperative basal calcitonin was 4880 ng/L, and surgical pathology demonstrated a 2 cm MTC; this case had the only false negative MTC Classifier result identified in this study of 10,488 tests.
Baseline serum calcitonin
Preoperative basal serum calcitonin values were available for 40 MTC patients identified by the MTC Classifier, including 37 with MTC confirmed on surgical pathology, while three were considered MTC based on a serum calcitonin >80 ng/L without surgery (Supplementary Table S1; Supplementary Data are available online at
Multiple endocrine neoplasia type 2
Among patients with surgically or biochemically confirmed MTC and Bethesda III/IV cytology, one of the 17 (5.9%) RET proto-oncogene tested patients was newly found to harbor a germline DNA mutation (Supplementary Table S1). Among tested Bethesda V/VI patients with positive MTC Classifier results, a germline RET mutation was present in 2/13 (15.4%).
Discussion
The limitation of thyroid FNAB cytopathology for the preoperative diagnosis of MTC has driven the search for alternative methods to diagnose MTC with greater efficacy (6,11,16,23,27,28,34,37 –45). Unfortunately, none have achieved international consensus for routine use. The most widely studied biomarker has been serum calcitonin, which demonstrates high diagnostic sensitivity but also a high false positive rate. Combined with the rarity of MTC, this results in a low PPV such that the majority of patients undergoing surgery due to high calcitonin levels do not have MTC on surgical pathology (23,40). To limit false positives, one could limit calcitonin screening to those with cytologically indeterminate nodules rather than testing all patients with nodules (Fig. 4, Paradigm C), but these approaches would require a second patient visit (or serum sample storage pending the cytology result), and would not identify MTCs with serum calcitonin values below the chosen cutoff, which may occur in both differentiated and poorly differentiated tumors (6,46,48). Most importantly, however, these approaches still result in an excess of false positive patients who undergo unnecessary preoperative MTC-specific evaluations and extensive MTC-specific surgery. Ironically, these false positive cases are more frequent than the actual number of true MTC cases found (Fig. 4, Paradigms B and C). While many advocate that an elevated baseline serum calcitonin should be followed by confirmatory stimulated serum calcitonin testing, the evidence that this improves diagnostic accuracy is not clear (27,40,46), and the possibility of serious adverse effects (even if rare) needs to be considered (49). Further, pentagastrin, which is used for the measurement of stimulated calcitonin concentrations, is not available for human use in the United States, Canada, and some other countries (18). Because of the very low false positive rate and high sensitivity of the MTC Classifier, an alternative diagnostic algorithm is proposed where the MTC Classifier is used at the initial FNAB (Fig. 4, Paradigm A). This approach is cost-effective when the GEC is already being used to reclassify cytologically indeterminate thyroid nodules as genomically suspicious or benign because the MTC Classifier result is automatically generated at the same time. Together, the GEC and the MTC Classifier provide actionable information on every patient tested. Almost all patients with Bethesda V/VI cytology undergo thyroid surgery without use of the GEC. For them, establishing the cost-effectiveness of preoperative MTC Classifier testing would require more formal investigation that considers the risks, benefits, costs (direct and indirect), complications of false positive and false negative results, alternative approaches such as serum or needle wash-out calcitonin measurement, and quality of life. Still, about one-quarter of MTC patients in these higher Bethesda categories would not be specifically identified as MTC by cytology (50). Yet, virtually all would be identified by the MTC Classifier.

Three paradigms for cytologically indeterminate (Bethesda III/IV) nodules to test for MTC. Paradigm A utilizes the Afirma GEC and MTC Classifiers in a single test. Paradigm B utilizes the Afirma GEC Classifier but not the MTC Classifier, and then screens GEC suspicious patients with serum calcitonin. Paradigm C utilizes only serum calcitonin. The paradigms utilizing calcitonin assumed no benefit of stimulated calcitonin testing due to similar test performance or unavailability (27,40,46). GEC, Gene Expression Classifier; ROM, risk of malignancy; PPV, positive predictive value. *Alexander et al. (47). †Frequency of a positive MTC Classifier in this series per Figure 2. ‡Alexander et al. (24). §1.15% prevalence of calcitonin ≥20 ng/L (16,34 –36). ‖81.8% operative rate for GEC suspicious nodules (47). ¶Operative rates of 64% and 72% for Bethesda III and IV, respectively (10). #20 positive MTC Classifier results (Fig. 2) and 7.5% of MTC cases have serum calcitonin <20 ng/L in this series.
High sensitivity, specificity, PPV, and NPV of the MTC Classifier were previously demonstrated in the prospectively collected, multicenter, and blinded validation study by Alexander et al. (Table 3) (24). That study was derived from a total enrollment of 4812 FNABs, of which 441 operated patients underwent GEC testing, including four histologically confirmed MTCs (Table 3). None of the 437 nodules with non-MTC histology were positive for the MTC Classifier, demonstrating exceptionally high specificity (100% [CI 99–100%]). All four MTCs were identified by the MTC Classifier (0, 2, and 2 MTCs among 61, 315, and 65 cytological Bethesda II, III–V, and VI categories, respectively), resulting in a perfect sensitivity (100%). This large dataset yielded a high and narrow confidence interval of the NPV (98.9–100%). That work has been extended by testing a large series of prospectively collected indeterminate FNABs to determine the prevalence of MTC positive results. To date, the current study represents the largest thyroid FNAB study evaluating the prevalence of MTC in routine clinical use. In this study, positive MTC Classifier results were found in each tested Bethesda category (III–VI), with the prevalence increasing in each successive category (Fig. 2). The prevalence of MTC among individual Bethesda categories III–VI has not been previously reported.
Out of 10,488 FNABs tested with the GEC, 43 cases tested positive by the MTC Classifier, with only one of these being a false positive, an intrathyroidal paraganglioma, an entity that is even rarer than MTC. As surgical resection is the standard treatment for paraganglioma, clinical utility of the MTC Classifier was not diminished. A plausible explanation for the positive MTC Classifier result is that both MTC and pheochromocytoma (intra-adrenal paraganglioma) are strongly positive for the granin family protein chromogranin A by immunohistochemistry (51). One of the MTC Classifier genes encodes another granin family protein, secretogranin III, present in association with chromogranin A in the secretory granules of neuroendocrine cells and known to show focal reactivity in pheochromocytomas (51). Of note, recently a post hoc analysis of a 15-gene subset of a 92-gene molecular classifier for tumor origin showed promise to distinguish pheochromocytoma and paraganglioma from MTC when using formalin-fixed, paraffin-embedded tissue samples and tumor enrichment (52). Feasibility or performance of this classifier on FNAB samples has not been reported.
Among the nine cases where cytopathology suggested MTC but the MTC Classifier was negative, only one of these cases proved to be MTC on surgical pathology, confirming a high NPV for this test. This is the only known false negative case among the 10,488 tested cases. In contrast to the high sensitivity of the MTC Classifier, cytology only suspected 19/43 cases (44%) as MTC. This latter finding is consistent with the recent large international multicenter study where cytology made the specific diagnosis of MTC in 46% of cases (50).
Limitations of this study are that calcitonin, chromogranin, CEA, or thyroglobulin immunohistochemistry, or calcitonin levels in the needle washout in each case (53), were not studied. In routine practice, these would each add significant cost. Among cytologically indeterminate nodules, even if one of these methods excluded MTC, the possibility of a more common thyroid malignancy would remain. In contrast, the MTC Classifier result is generated concurrent with the GEC result at no added cost. The MTC Classifier sensitivity or NPV were also not computed on this cohort. To do so would require that all 10,445 MTC Classifier negative patients undergo surgical resection, despite the fact that many of them had genomically benign GEC results that likely allowed them to avoid diagnostic surgery—a clearly impractical study design. Despite this limitation, true and false positive cases were identified to compute the PPV for this cohort, given that “truth” (via surgical pathology in most, or serum calcitonin) was assigned to nearly all MTC Classifier positive cases. Only one false positive MTC Classifier result was identified among 7815 prospective consecutive cytologically Bethesda III/IV nodules tested with the Classifier (0.013%). Specificity (true negatives/[true negatives + false positives]) is likely to be very high, given that only one false positive result was identified, and the rarity of MTC makes it highly likely that all (or nearly all) MTC Classifier negative cases are true negatives.
Clinical utility is established when a test improves the net health benefit for the patients and/or population in which it is used. Many believe that the benefit of screening for sporadic MTC with serum calcitonin has not been established because many of the tumors found are microcarcinomas with an unknown natural history (53). The MTC Classifier avoids this limitation by informing only on the specific nodule intentionally biopsied by the clinician. MTC is the only thyroid cancer where a total thyroidectomy and prophylactic central neck dissection is routinely recommended (33,53). As half of MTC cases are not specifically identified by cytology alone (5,6), a finding confirmed here, the preoperative identification of these malignancies by the MTC Classifier via a single test (Fig. 4) would allow an optimal initial surgical approach for MTC avoiding second “completion” surgeries, in addition to prompting the preoperative evaluation for MEN2.
Contrary to guideline recommendations, only 30/43 MTC patients identified in this series underwent RET proto-oncogene mutation testing (33,53). This finding highlights a gap in clinical practice and suggests an opportunity for physician education. Of the 30 tested MTC patients, three (10% [CI 3–28%]) were found to harbor a germline RET mutation, which carries significant implications for the patient's family (Supplementary Table S1).
Here, the accuracy of MTC Classifier positive results is demonstrated among samples tested prospectively in routine, real-world clinical practice. The MTC Classifier identifies clinically relevant MTC in cytology specimens where MTC is often missed, allowing patients to receive the appropriate surgery at the first intervention, while simultaneously avoiding false positives that lead to unnecessary surgeries on patients without MTC. The MTC Classifier advances the ability to detect and correctly treat MTC earlier, and is an improvement over current methods.
Footnotes
Acknowledgments
The authors would like to thank the many physicians and healthcare professionals who provided information regarding patients in this study. We gratefully acknowledge Zhanzhi Hu, PhD, and Mei Wong of Veracyte for assistance in establishing prevalence of MTC mRNA signatures among Bethesda cytology categories not routinely reflexed to the GEC.
Author Disclosure Statement
R.T.K., G.C.K., R.J.M., and R.B.L. are, or were, Veracyte employees. R.T.K., G.C.K., R.J.M., S.T.T., and R.B.L. are equity owners in Veracyte. GCK has U.S. Patent 8,541,170 issued. R.T.K. is a consultant to Novo Nordisk.