
Abstract
Background:
Iatrogenic trauma induced by thyroid surgery is the most common etiology of unilateral vocal fold paralysis (UVFP). UVFP after thyroid surgery may lead to profound physical and psychosocial distress. This study comprehensively evaluated UVFP caused by thyroid surgery, and compared the results with those caused by other surgical trauma.
Methods:
Patients with surgery-related UVFP were evaluated using quantitative laryngeal electromyography, videolaryngostroboscopy, voice acoustic analysis, the Voice Outcome Survey, and the Short Form-36 Health Survey quality-of-life questionnaire. Patients with thyroid surgery and other surgeries were compared.
Results:
A total of 105 patients were recruited, of whom 52 and 53 were assigned to the thyroid surgery and the other surgery group, respectively. Patients in the thyroid surgery group had a higher proportion of external branch of superior laryngeal nerve (eSLN) involvement, longer duration from disease onset to the first laryngeal electromyography examination, lower jitter, higher harmonic-to-noise ratio, and better quality of life compared with the other surgery group. Specifically for patients in the thyroid surgery group, those with eSLN involvement tended to have more pronounced impairment in jitter and shimmer compared with patients without eSLN involvement.
Conclusion:
UVFP caused by thyroid surgery has a distinct clinical presentation with relatively high involvement in the eSLN, better voice acoustics, longer waiting time before asking for evaluation, and less impact on quality of life. The involvement of eSLN in these patients further impaired their voice. Early referral is suggested for these patients, especially with suspected eSLN injury.
Introduction
I
According to previous studies, the incidence of vocal fold palsy caused by TS is 1.5–5.3% (7 –9), with most cases recovering within 12 months and 15–17% showing permanent vocal fold palsy (7,8). Compared with vocal fold palsy induced by TS, the incidence of vocal fold palsy was even higher in OS, with 15% in surgery for esophageal cancer (10), 31% in pulmonary surgery (11), and 5–32% in aortic surgery (12 –15), further increasing the incidence of pneumonia, hospital stay, intensive care unit stay, and the mortality rate (12 –14). Further, vocal cord palsy induced by OS was more likely to be permanent (15,16). However, a comprehensive comparison between UVFP induced by TS and OS has not been performed.
Almost all cases of UVFP involve injury of the recurrent laryngeal nerve (RLN), while injury of the external branch of superior laryngeal nerve (eSLN) can also occur (17,18). RLN damage results in weakness in the thyroarytenoid-lateral cricoarytenoid (TA-LCA) muscle complex, making vocal fold adduction difficult. By contrast, eSLN damage can impair the cricothyroid (CT) muscle, affecting the control of voice tone (19,20).
Quantitative laryngeal electromyography (LEMG) was recently developed to evaluate the severity of neuromuscular impairment caused by denervation changes in UVFP (21). Quantitative LEMG has good diagnostic, functional, and prognostic values, and is extremely useful to evaluate TS-related UVFP (6,17,21). In the present study, we performed a retrospective analysis of patients with surgery-induced UVFP examined by quantitative LEMG together versus other anatomical and functional evaluation methods. The specific aim of this study was to characterize the differences in disease presentation and functional impairment between UVFP caused by TS and OS. These findings may help determine the most appropriate treatment for patients with surgery-related UVFP.
Materials and Methods
Human subjects
Subjects were recruited from the otolaryngology outpatient clinic at a medical center (Lin-Kou Chang Gung Memorial Hospital, Taiwan) from September 2011 to March 2015. Inclusion criteria were adult patients (>20 years old) with symptoms and signs of UVFP occurring immediately after surgery. The diagnosis was confirmed by videolaryngostroboscopy and needle LEMG. The exclusion criteria were patients with (i) symptoms and signs of UVFP before surgery, (ii) brain surgery that caused bulbar palsy with suspect laryngeal sensory deficit, (iii) bilateral vocal fold palsy confirmed by LEMG, and (iv) a history of invasive interventions to correct the paralyzed vocal fold position, such as intracordal injection or laryngoplasty. All aspects of the study were approved by the Human Studies Research Committee of Chang Gung Medical Foundation. Written informed consent was obtained from each participant.
Procedures
Patients underwent assessments, including LEMG with quantitative analysis, videolaryngostroboscopy, the Voice Outcome Survey (VOS) questionnaire, voice acoustic analysis, and the Short Form-36 (SF-36) Health Survey quality-of-life questionnaire. These assessments were performed within two weeks of the day of LEMG assessment. The interval between the date of the surgery and the date of LEMG was calculated.
LEMG examination
The standard protocol for needle LEMG was performed by a board-certified otolaryngologist (T.-J.F.) and physiatrist (Y.-C.P.). A Nicolet Viking Select (Cardinal Health, Dublin, OH) was used with a band-pass filter set between 20 and 10 khz. The patients had a LEMG examination with neck extension posture, supported by an adjustable neck–head rest, seated on a reclining chair specifically designed for laryngeal examinations. At the beginning of the exam, approximately 1 mL of 2% lidocaine hydrochloride was injected into the subcutaneous tissue at the LEMG needle-insertion sites by the otolaryngologist. LEMG signals on bilateral TA-LCA muscle complexes and CT muscles were obtained using a concentric needle electrode with the surface-ground electrode on the skin of the forehead.
With the concentric needle electrode in the TA-LCA muscle complex, the patient produced three series of /e/ sounds at three different intensities (low, moderate, and as high as possible), with each /e/ lasting at least 400 ms and each inter-/e/ interval approximately 200 ms. To evaluate CT function, the patients were asked to produce a glissando upward /e/ at normal loudness.
For each muscle, insertional activity and spontaneous activity were first evaluated. Semi-quantitative motor unit analysis and recruitment analysis were then performed, specifically when the rise time of a motor unit action potential was <0.6 ms, indicating a close proximity to the recorded motor unit. Abnormal LEMG was defined as the existence of spontaneous activities (such as fibrillation, positive sharp wave, and complex repetitive discharge), >30% polyphasia, or decreased interference pattern (reduced, discrete, or no interference pattern). Motor unit recruitment tracings were recorded for offline analysis.
Quantitative LEMG analysis
A Matlab (The Mathworks, Natick, MA)-based program was developed to analyze the raw LEMG data. The raw LEMG waveforms were first binned into non-overlapping epochs. The epoch durations for the TA-LCA and CT muscles were 200 ms (19) and 50 ms, respectively. A shorter bin width was chosen for the CT muscle to capture the dynamic control for the upward glissando /e/. The timing of each turn and its amplitude was localized using an automatic algorithm. Specifically, a turn was defined by the change in polarity with amplitude of at least 100 μV before and after the change, to exclude noise-related peaks. Turn frequency was computed for each epoch as the number of turns divided by the epoch duration. Turn amplitude was computed as the mean of the absolute turn-amplitude values. For each muscle, the turn frequencies for the epochs were averaged with turn frequencies that ranked among the top three epochs to yield the peak turn frequency. The turn ratio was defined as the turn frequency of the lesion side muscle divided by the turn frequency of the normal side muscle, which prevents individual bias.
Videolaryngostroboscopy
The otolaryngologist asked each patient to project the vowel /e/ at their habitual pitch and intensity, and the voice and vocal fold vibration samples were recorded by videolaryngostroboscopy. Using Image J software (Image J 1.44; National Institutes of Health, Bethesda, MD), the recorded movie was analyzed offline frame by frame, yielding the normalized glottal gap area (NGGA) following the method by Omori et al. (22) as described in the equation:
Glottal gap area is defined as the image area in square pixels within the glottal area identified using the segmentation process, and membranous vocal fold length represents the distance expressed in pixel length from the anterior commissure to the tip of the membranous vocal process. The glottal gaps were measured in both maximally open and closed phases during vocal fold vibration to yield open-phase and closed-phase NGGAs, respectively.
Voice acoustic analysis
The voice samples were recorded by a certified speech pathologist while the patient read a standard passage and sustained a vowel in conversational pitch and loudness. The maximal phonation time represented the duration a patient could sustain an /a/. A stable segment from the mid-portion of the vowel voice sample was used for the following acoustic analysis. Acoustic characteristics of the recorded voice were measured using a computerized speech laboratory system (CSL4300B 5.05; Kay-PENTAX, Montvale, NJ) that yielded the fundamental frequency (F0), jitter (frequency perturbation), shimmer (amplitude perturbation), and harmonic-to-noise ratio. Finally, the patient produced each of a sustaining /s/ and /z/ as long as possible, from which the S/Z ratio (S/Z) was computed as the ratio of /s/ and /z/ durations (23).
UVFP-related health: VOS questionnaire
The VOS, developed by Gliklich et al. (24) using a Likert scaling technique, is a five-item survey for evaluating the physical and social problems caused by UVFP. The total scores were normalized between 0 (worst) and 100 (best), based on the published algorithm. The Mandarin version of VOS has undergone a standard survey-validation process (25).
General health: the SF-36 quality-of-life questionnaire
The SF-36 Health Survey is a 36-item, patient-reported survey of patient health. The SF-36 consists of eight scaled scores, which are the weighted sums of the questions in each section. Each component scale is directly transformed into a 0–100 score on the assumption that each question carries an equal weight and the lower the score the more disability. The recall period for SF-36 is four weeks. We adopted the SF-36 Assessment Standard Taiwan version 1 with its Taiwanese norm (26,27).
Statistical analysis
Differences between the TS and OS groups were compared using chi-square tests or Fisher's exact test for nominal data (such as sex, lesion side, and CT injury) and Student's t-tests for numerical data. Analysis of covariance was used to analyze the fundamental frequency obtained in acoustic analysis in a model using sex as a covariate because the sex would affect fundamental frequency. In statistical analysis for each parameter, only complete data were used. The level of significance was defined as p < 0.05.
Results
During the study period, 198 UVFP patients received LEMG evaluation, 147 cases of which were caused by surgical morbidity. Forty-two patients were excluded, two for brain surgery-related bulbal palsy, three for a history of intracordal injection, five for refusing the examination, 23 for incomplete LEMG data, and nine for bilateral vocal fold palsy confirmed by LEMG. A final 105 patients remained for data analysis, with 52 in the TS group and 53 in the OS group.
Patients in the TS group received TS, such as thyroidectomy, while those in the OS group received other types of surgery, including 21 with esophageal surgery, 16 with lung surgery, six with heart surgery, five with cervical spinal surgery, three with mediastinal surgery, one with subclavian artery repair, and one with supraclavicular lymph node dissection (Fig. 1). Because of loss of follow-up with some patients, there were three missing data sets in the TS group and three in the OS group for videolaryngostroboscopy, four in the TS group and two in the OS group for voice acoustic analysis, and one in the TS group and three in the OS group for voice outcome survey and quality of life.
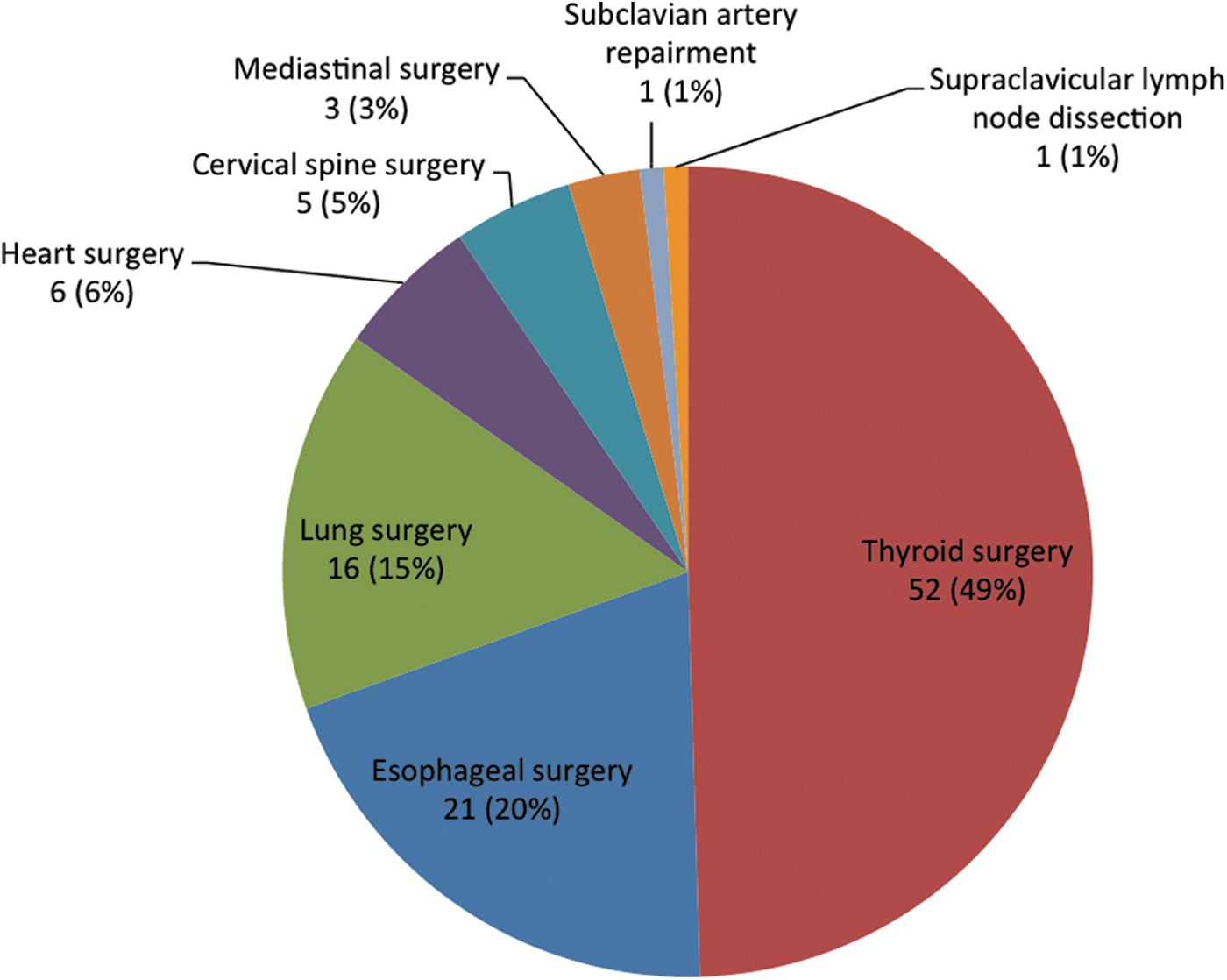
Surgical types of all unilateral vocal fold paralysis (UVFP) patients included in the present study. Data are presented as case number (percentage). Color images available online at
Demographics
The TS group showed a female predominance (male/female: 7/45), compared with a male predominance in the OS group (male/female: 37/16; p < 0.001; Table 1). The two groups did not differ in age (50.8 ± 13.4 years vs. 53.3 ± 15.5 years, respectively; p = 0.38). The OS group had a higher proportion of left UVFP (right/left: 15/38) than the TS group did (right/left: 25/27; p = 0.04). The TS group had a higher probability of CT muscle involvement, being relevant to eSLN injury, compared with the OS group (16/52, 31% vs. 7/53, 13%, respectively; p = 0.03). There was also a longer referred interval from symptom onset to LEMG exam in the TS group than in the OS group (5.6 ± 5.6 months vs. 3.8 ± 1.7 months; p = 0.03).
Data are presented as mean ± standard deviation.
p < 0.05; ** p < 0.01; *** p < 0.001.
†p-Value was adjusted by sex.
UVFP, unilateral vocal fold paralysis; TS, thyroid surgery; OS, other surgery; eSLN, external branch of superior laryngeal nerve; LEMG, laryngeal electromyography; NGGA, normalized glottal gap area; TA-LCA, thyroarytenoid-lateral cricoarytenoid muscle complex; CT, cricothyroid muscle.
Quantitative LEMG
Quantitative recruitment analysis showed no difference in turn frequency or turn ratio of the TA-LCA muscle complex in the lesion side between the two groups, indicating an equal level of recurrent laryngeal nerve denervation. However, turn frequency of the TA-LCA muscle in the normal side was significantly higher in the OS group than in the TS group (1043 ± 407 vs. 846 ± 265, respectively; p = 0.004). Because the turn frequency of the normal TA-LCA muscle was within the normal range, this difference may simply reflect the difference of neuromuscular compensation for UVFP.
The incidence of CT injury in the TS group was significantly higher (16/52, 31%) than that in the OS group (7/53, 13%; p = 0.03). The turn frequency of the CT muscle in the lesion side showed a trend for being lower in the TS group than in the OS group (647 ± 323 vs. 739 ± 312, respectively; p = 0.14). The turn frequency of the CT muscle in the non-palsy side was similar between the two groups (p = 0.88).
Next, we specifically analyzed patients with combined RLN and eSLN injuries to compare their CT and TA-LCA activities between the TS and OS groups (Table 2). Among UVFP patients with eSLN injury, there was no difference in CT turn frequency (329 ± 257 vs. 378 ± 173, respectively; p = 0.65) or TA-LCA turn frequency (283 ± 201 vs. 273 ± 177, respectively; p = 0.92) in the palsy side between the two groups. Again, the TA-LCA turn frequency on the non-palsy side was significantly higher in the OS group (1008 ± 371 vs. 722 ± 242, respectively; p = 0.04).
Data are presented as mean ± standard deviation.
p < 0.05.
Videolaryngostroboscopy
A total of 99 patients (49 in the TS group, 50 in the OS group) received videolaryngostroboscopy. Analysis of the glottal gap showed no difference in closed-phase NGGA (p = 0.32) or open-phased NGGA (p = 0.39) between the two groups (Table 1).
Voice acoustic analysis
voice acoustic analysis was performed in 98 patients: 48 in the TS group and 50 in the OS group. The TS group had a significantly higher harmonic-to-noise ratio (6.62 ± 3.16 vs. 5.32 ± 3.27, respectively; p = 0.047) and lower jitter (3.28 ± 2.10 vs. 5.14 ± 5.68, respectively; p = 0.03) than the OS group did. The TS group had significantly higher fundamental frequency (208 ± 69 vs. 162 ± 59). However, this was not significant after sex was adjusted in an analysis of covariance model. Other voice parameters, including maximal phonation time (p = 0.17), S/Z ratio (p = 0.37), and shimmer (p = 0.57), did not differ between the two groups (Table 1).
UVFP-related health: VOS questionnaire
The VOS questionnaire data were collected from 101 patients: 51 in the TS group and 50 in the OS group. There was no difference in VOS score (34.3 ± 16.6 vs. 36.5 ± 18.7, respectively; p = 0.53) between the two groups (Table 1), indicating comparable voices.
General Health: SF-36
SF-36 questionnaire data were collected from 101 patients: 51 from the TS group and 50 from the OS group. Quality-of-life domains measured by the SF-36 were compared between the two groups (Table 1). The TS group had relatively higher scores in physical functioning (81.2 ± 15.2 vs. 70.5 ± 20.3, respectively; p = 0.003) and role limitations due to physical health (39.2 ± 44.5 vs. 21.5 ± 37.8, respectively; p = 0.03) compared with the OS group, and a trend for higher scores in bodily pain (80.0 ± 20.6 vs. 71.7 ± 25.7, respectively; p = 0.08). There were no differences in other domains, including vitality (p = 0.67), general health perceptions (p = 0.6), social functioning (p = 0.64), and mental health (p = 0.26), between the two groups. These results indicate that quality of life was less affected in patients in the TS group compared with the OS group.
eSLN injury in thyroidectomy-related UVFP
To evaluate the impact of eSLN injury on clinical presentations, subgroup analysis was performed specifically for patients in the TS group (Table 3). In the group without eSLN injury, there were three, four, one, and one missing data sets for videolaryngostroboscopy, voice acoustic analysis, and voice outcome survey, and quality of life, respectively. Individual parameters with complete recording were collected for statistical analysis.
Data are presented as mean ± standard deviation.
p < 0.05.
The patient demographics did not differ between the groups, including sex, age, side of paralysis, or referral interval to otolaryngologist. TS patients with eSLN injury had a trend for larger close-phase NGGA (12.3 ± 13.0 vs. 6.38 ± 7.45, respectively; p = 0.11), and significantly higher jitter (4.43 ± 2.57 vs. 2.71 ± 1.58, respectively; p = 0.02) and shimmer (1.55 ± 1.36 vs. 0.73 ± 0.83, respectively; p = 0.01) compared with TS patients without eSLN injury. Further, TS patients with eSLN injury had a trend for lower maximum phonation time (4.8 ± 2.9 vs. 7.2 ± 5.6, respectively; p = 0.13) and harmonic-to-noise ratio (5.21 ± 3.91 vs. 7.33 ± 2.48, respectively; p = 0.06). There were no differences in quality of life between the two groups. Based on the findings on the videolaryngostroboscopic study and acoustic analysis, CT dysfunction caused by eSLN injury further impaired tone and amplitude control and sustainability in TS patients.
Discussion
The present study found that TS-related UVFP had a higher proportion of eSLN injury, longer duration from disease onset to the first LEMG examination, less impairment in frequency control and voice harmonics, and a better quality of life compared with OS techniques. It is important to consider whether these differences are due to surgery techniques or a result of patient demographics, as patients receiving TS are younger and predominantly female (7) compared with patients receiving OS (10,13,14). However, there was a comparable age between the two groups in this study, despite clinical experience and other studies showing a relatively younger age in patients with vocal fold palsy caused by TS, with a mean age of 45 years in TS (7), 65 years in aortic surgery (13), 61 years in pulmonary surgery (16), and 58 years in esophageal surgery (10).
The higher proportion of eSLN injury in UVFP after thyroidectomy is related to CT dysfunction and can cause further deterioration of the voice and quality of life (19,20). Subgroup analysis in the TS group supports that the CT dysfunction, caused by eSLN neuropathy, affects voice control. This is an important consideration for treatment planning for TS patients, as those with eSLN involvement tend to have more social and occupational problems, despite relatively good physical function.
Ligation of the superior thyroid artery during TS for the superior pole of the thyroid gland can result in eSLN damage, especially if the procedure is performed too high along the vascular pedicle (28,29). Further, the eSLN has a variable course, increasing the risk for surgical injury. Several classifications for anatomic variance were constructed to guide the surgeon to identify the nerve, to predict and prevent risk of injury (28 –30). In the present study, OS that may damage eSLN were predominantly esophageal surgeries involving the upper third esophagus, lung surgery with neck lymph node dissection, and cervical spine surgeries, all of which involve neck procedures. Indeed, for the esophageal surgical method, transhiatal resection with cervical esophagogastrostomy had a high incidence of vocal fold palsy when compared with abdominal-thoracic anastomosis (10).
A longer referred interval to the laryngology specialists was also found in TS patients. Indeed, UVFP patients caused by TS had less impairment in their physical function and quality of life when compared with those caused by OS. Thus, thyroid surgeons may consider UVFP as a transient complication and choose a relatively conservative management, or simply observation for spontaneous recovery. However, prolonged observation without voice therapy may result in compensatory vocal behaviors (such as supraglottic hyperfunction) that further complicate their recovery (31).
Besides that, early referral can also facilitate adequate intervention for UVFP such as intracordal hyaluronate injection, which can provide immediate improvement of voice and long-lasting improvement of quality of life (32). We concur with the voice issue recommendations in the recently published guidelines by the American Thyroid Association and the American Academy of Otolaryngology (31,33), which recommend that postoperative voice evaluations be performed at two weeks to two months after surgery. These recommendations contrast with the relative late referral to laryngologists found in the current study.
There are several potential limitations in this study. First, the two groups have an obvious sex difference, which may induce bias in examination values, especially for those obtained in the voice acoustic analysis. Second, there is a wide variety of operations performed in the OS group, making it difficult to compare it accurately with the TS group. Finally, there is no long-term follow-up. This will be performed in future studies to help determine the prognostic factors that are important for the selection of appropriate treatments for each patient.
Conclusion
The incidence of eSLN injury is high in UVFP caused by TS, and patients with eSLN paralysis had worse voice performance. A relatively late referral was noticed for UVFP caused by TS.
Footnotes
Acknowledgments
The research was supported by a National Science Council Grant (MOST 103-2314-B-182A-056-MY2 and 104-2314-B-182-050-) and a Chang Gung Medical Foundation Grant (CMRPG 3D1412, 5D01061, 3E1721, and 3C046c). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
The authors declare no conflict of interest.