
Abstract
Background:
Thionamides are associated with a high risk of recurrence following cessation. Thyrotropin receptor-stimulating antibody (TRAb) levels at diagnosis and/or after thionamides may be biomarkers of this risk. This study assesses the natural history of Graves' thyrotoxicosis following thionamide withdrawal and factors that predict recurrence, particularly TRAb levels at diagnosis and cessation.
Methods:
An observational study was conducted of patients with a first presentation of Graves' disease, who were prescribed (and completed) a course of primary thionamide treatment (n = 266) in a university teaching hospital endocrine clinic. Recurrence rates over four years and factors predictive of recurrent thyrotoxicosis were assessed.
Results:
The relapse rate was 31% at one year and 70% at four years. Younger age (39 years [range 30–49 years] vs. 47 years [range 37–53 years]; p = 0.011), higher TRAb levels at diagnosis (8.8 IU/L [range 5.3–17.0 IU/L] vs. 5.7 IU/L [range 4.1–9.1 IU/L]; p = 0.003), and higher TRAb levels at cessation of therapy (1.2 IU/L [range 0–2.3 IU/L] vs. <0.9 IU/L [range 0–1.3 IU/L]; p = 0.003) were associated with a higher risk of relapse. By four years, cessation TRAb <0.9 IU/L was associated with a 58% risk of recurrence compared with 82% with TRAb >1.5 IU/L (p = 0.001). TRAb at diagnosis >12 IU/L was associated with an 84% risk of recurrence over four years compared with 57% with TRAbs <5 IU/L (p = 0.002).
Conclusion:
High TRAb at diagnosis and/or positive TRAb at cessation of therapy suggest a high likelihood of relapse, mostly within the first two years. They stratify patients likely to need definitive therapy (radioiodine or surgery).
Introduction
T
Previous studies have not determined the influence of modest elevations in TRAb concentration at diagnosis or after thionamides. Moreover, the precise risk of recurrence is hampered by relatively short duration of follow-up. This study assesses the long-term natural history of Graves' thyrotoxicosis following thionamide withdrawal and the predictive value of TRAbs.
Subjects and Methods
Patients
Two hundred and sixty-six patients diagnosed with a first presentation of Graves' disease treated with primary thionamide therapy (and completing a physician prescribed treatment course) between 2006 and 2011 were identified from the Edinburgh Centre for Endocrinology and Diabetes (ECED) database. For each case, serial thyroid function tests were recorded for up to four years after drug withdrawal. All patients with active Graves' disease, within the catchment population, are managed in ECED clinics and not in primary care. The catchment area includes the city of Edinburgh, East Lothian, and Midlothian, with a combined population of approximately 700,000.
Patients lost to follow-up were reviewed by the indexing department of Information Services Division Scotland to establish whether they had moved from the health board area, died, or remained within the health board area but had not received further thyroid function tests. All patients with missing data were excluded from that stage of the analysis. Data collection ended in October 2015, with data available in 266, 247, 205, and 184 patients for each successive year (Fig. 1).

Summary of patients included in analysis of recurrence at one, two, three, and four years, including reasons for exclusion from analysis at each step.
Assays
From 2007 onwards, all thyrotropin (TSH), free thyroxine (fT4), and total triiodothyronine (TT3) measurements were performed on an Abbot Architect Immunoassay system (Abbott Diagnostics, Maidenhead, United Kingdom). The reference range for TSH is 0.2–4.5 IU/L; for fT4, it is 9–21 pmol/L; and for TT3, it is 0.9–2.4 nmol/L. Prior to 2007, assays were performed on either Advia Centaur (Siemens Healthcare Diagnostics, Surrey, United Kingdom) or the Vitro ECi platform (Ortho Clinical Diagnostics, High Wyncombe, United Kingdom) across the two hospital sites comprising the ECED. Regression equations were used to correct all non-Architect derived TSH, fT4, and TT3 values reported in this study (Dr. G. Beckett and Ms. C. Shearing, Clinical Biochemistry Department, NHS Lothian, pers. comm.). All assays had a coefficient of variation of <10% over the concentration ranges measured.
TRAbs were measured using the second-generation BRAHMS LUMItest TRAK assay (BRAHMS Diagnostica, Berlin, Germany) until 2008 when it was replaced by a Roche assay performed on the Cobas E411 analytical platform (Roche Diagnostics, West Sussex, United Kingdom) (11). No significant differences were noted between the two TRAb assays used (12). The functional sensitivity of the TRAb assays was 0.9 IU/L, with normal TRAb levels <1.5 IU/L. Anti-TPO antibodies were measured using Orgentec enzyme-linked immunosorbent assay (Mainz, Germany). The reference range for anti-TPO antibodies is 0–150 IU/L.
Biochemical parameters
Diagnosis of Graves' thyrotoxicosis was defined by clinical features and associated biochemical markers. fT4, TT3, TSH, and TRAbs were recorded at diagnosis. Antithyroid peroxidase antibody titer (anti-TPO) was also recorded if available. A high serum level of fT4 or TT3, suppressed level of TSH, and a positive TRAb titer established a biochemical diagnosis of Graves' thyrotoxicosis.
All follow-up, thyroid function tests were reviewed, and time to normalization of fT4 and TSH was recorded. In the majority of patients (n = 207), TRAb levels prior to cessation of therapy were recorded.
After thionamide withdrawal, serial thyroid tests, including fT4 and TT3, were reviewed up to the end of the study date. The endpoint measurement (in months) was annual remission or time to relapse. Remission was defined as biochemical and clinical euthyroidism, as measured each year after drug withdrawal. Relapse was defined as biochemical or clinical hyperthyroidism with re-referral to the endocrine clinic. Time to relapse was defined by date of first biochemical evidence of relapse.
Clinical parameters and associated risk factors
Clinic letters were reviewed for age, sex, and smoking status. Smoking status was categorized as non-smoker, current smoker, or ex-smoker. No specific duration of time was defined for ex-smoker. Goiter size and thyroid eye disease were not evaluated in final statistical analysis, as no quantitative measures were consistently used for these parameters during the study period.
Therapy
The standard practice in the authors' center was to prescribe an 18-month course of carbimazole, typically starting at 40 mg once daily and titrating down in line with biochemical response, ultimately to 5 mg in most cases. Propylthiouracil (PTU) was given as first-line treatment in women of child-bearing age who were pregnant or expressed plans for pregnancy, and as second-line treatment in patients who did not tolerate carbimazole. A “block-and-replace” regimen was given as second-line treatment to a few individuals. Peak thionamide dose is defined as the highest dose taken during period of drug treatment; final dose is defined as the drug dose immediately prior to cessation. Peak and final thionamide dose did not differ between those who relapsed and those who did not.
Statistics
The primary outcome measure was recurrent thyrotoxicosis following thionamide withdrawal. Subjects were divided into two groups based on recurrence, and the median values of quantitative clinical parameters were compared using the Mann–Whitney U-test. Risk of relapse is presented using Kaplan–Meier survival plots and groups compared using a log-rank test. For categorical variables, Pearson's chi-square test was used. Binary logistic regression was performed to assess categorical and continuous independent factors predictive of relapse (the dependent binary variable). Data were analyzed using IBM SPSS Statistics for Windows v22 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant.
For statistical analysis, concentrations that were above and below the threshold of assay were given specific values. TRAb levels <0.9 IU/L were recorded as 0 IU/L. TRAb levels >40 IU/L were recorded as 40 IU/L. TT3 >12.3 nmol/L or >10 nmol/L (with earlier Advia Centaur or Vitro ECi assay) was recorded as 12.3 nmol/L. TRAb status at diagnosis was stratified into three categories: <5 IU/L, 5–12 IU/L, and >12 IU/L, which were selected pragmatically to provide numerical balance, recognizing the lower frequency of patients with the highest TRAb concentrations. TRAb status at cessation was also stratified into three categories: <0.9, 0.9–1.5, and >1.5 IU/L, reflecting the lower limit of quantification, the reference range, and high values, respectively.
Results
Treatment
Seventy-eight percent of patients were female. At cessation of therapy, 86% (n = 159/184) were taking carbimazole, and 14% (n = 25/184) were taking PTU. The median duration of thionamide treatment was 18 months (17 –20).
Relapse
The relapse rate after cessation of thionamide therapy was 31% (n = 82/266) at one year, 45% (n = 111/247) at two years, 61% (n = 125/205) at three years, and 70% (n = 128/184) at four years based on confirmed biochemical euthyroidism at each year, with a trend toward a plateau in relapse risk at around 30 months. When accounting for patients still residing within the health board area, who have not sought further thyroid function tests, it may be reasonable to assume they have remained euthyroid, in which case the two-, three-, and four-year relapse figures are 43% (111/261), 54% (125/232), and 66% (128/193), respectively.
Predictive factors
Comparison of biochemical and clinical characteristics between those in remission and those with recurrent thyrotoxicosis at four years is shown in Table 1. An elevated risk of relapse was associated with four consistent factors in all successive years of follow-up: younger age, higher TRAb levels at diagnosis, longer time to normalization of TSH, and higher TRAb levels at cessation of therapy. Sex, fT4 and TT3, smoking status, and anti-TPO concentration at diagnosis were not associated with relapse. Binary logistic regression confirmed that age (hazard ratio [HR] = 0.95 [confidence interval (CI) 0.92–0.98]; p = 0.02), diagnosis TRAb (HR = 1.06 [CI 1.00–1.11]; p = 0.38) and cessation TRAb (HR = 1.79 [CI 1.23–2.59]; p = 0.002) were all independently predictive of relapse.
Results presented as median (interquartile range). Pearson chi-square test was used for sex. Mann–Whitney U-test was performed for all other parameters.
fT4, free thyroxine; TT3, total triiodothyronine; TRAb, thyrotropin receptor-stimulating antibody; TSH, thyrotropin.
The predictive value of TRAb levels at diagnosis was assessed by stratifying patients into one of three TRAb categories: (i) TRAb <5 IU/L; (ii) TRAb 5–12 IU/L; and (iii) TRAb >12 IU/L. TRAb levels of >12 IU/L at diagnosis were associated with a 84% risk of recurrence over four years compared with 57% when diagnosis TRAbs were <5 IU/L (p = 0.002; Table 2). These data are presented in Kaplan–Meier plots demonstrating the influence of TRAbs at diagnosis over four years of follow-up (Fig. 2A). Similarly, the influence of TRAb levels at cessation of thionamide therapy was assessed by stratifying patients into three categories: (i) negative (<0.9 IU/L); (ii) detectable, low normal (0.9–1.5 IU/L); and (iii) positive (>1.5 IU/L). At one year, the rate of relapse was 47% in the elevated TRAb category compared with 22% in the undetectable TRAb category. Higher relapse rates were seen in the elevated TRAb category in all successive years (Table 2). These data are presented in Kaplan–Meier plots demonstrating the influence of TRAbs at cessation over four years of follow-up (Fig. 2B). The median remission time for subjects with undetectable TRAbs at cessation was 26 months [CI 17–34 months] compared to 10 months [CI 5–14 months] in those with elevated TRAbs.
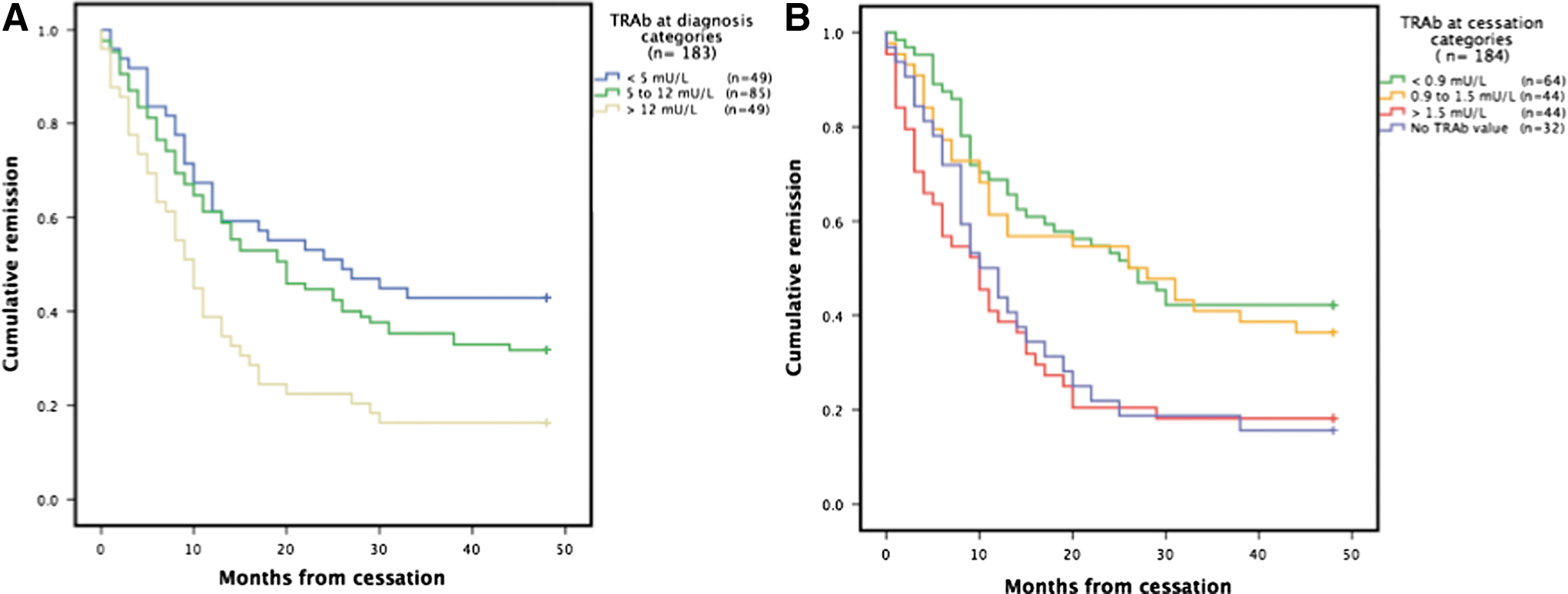
Kaplan–Meier plots of patients in remission 48 months after thionamide cessation. (
Data are n (%). Log-rank * p < 0.05; ** p < 0.01.
Discussion
This study has shown that even modestly elevated TRAb at cessation of thionamide therapy is associated with a very high rate of recurrent thyrotoxicosis, with a similar pattern observed in patients with high TRAb levels at diagnosis. These data are likely to be useful in helping determine optimal primary therapy (thionamide, radioiodine, or surgery) and in clarifying the risk, and time course, of recurrence in patients completing a primary course of thionamide. Increased mortality has been reported in thionamide-treated patients who develop recurrent thyrotoxicosis, particularly in those with cardiovascular morbidity (13). In such situations, where the risks of recurrent thyrotoxicosis are unacceptably high, these data suggest long-term, low-dose thionamide may be a better option than withdrawal and observation.
Relapse rate at one year (31%) was similar to previous reported studies (7,8). While there is a degree of variability in the duration and dose of thionamide therapy across this cohort, reflecting typical clinical practice, it is unlikely to have affected outcomes. Duration of therapy was similar in the relapse and remission groups, and there were no statistical significant differences in thionamide doses between groups. This is in keeping with a meta-analysis that showed higher doses, longer duration, and use of a “block-and-replace” regimen with thionamide therapy did not influence relapse risk (10).
Arguably, thionamide therapy should therefore continue until TRAb levels are negative or at least in the normal range (i.e., <1.5 IU/L). It would be interesting to investigate whether continuing thionamide therapy until TRAbs become undetectable would be associated with improved long-term remission rates. Remission rates were not meaningfully different between those with undetectable TRAbs (<0.9 IU/L) and those with minimally detectable TRAbs at cessation (0.9–1.5 IU/L), with 22% of “negative” TRAb patients relapsing within one year of treatment withdrawal. This highlights the necessity for more effective biomarkers of disease activity. Recent advances in “third-generation” TRAb assays, with sensitivity levels of <0.4 IU/L (14), may permit more accurate recurrence risk assessment, although this will require confirmation in prospective studies. A functional TRAb assay, utilizing a chimeric TSH receptor (Mc4), has shown superior efficacy in predicting relapse following thionamide withdrawal in 33 patients in whom thionamide withdrawal was attempted. However, pending confirmation of these promising early data, the Mc4 assay is unlikely to be widely available for clinical use (15). The findings in the presentcohort are difficult to reconcile with previous reports suggesting no predictive value of cessation TRAbs (16), but are congruent with the findings of a number of other investigators (8,17,18).
Higher TRAb levels at diagnosis were associated with higher relapse risk, and Kaplan–Meier curves showed significant differences among the three TRAb categories at one- and particularly four-year follow-up. In many respects, although this parameter is slightly less predictive than cessation TRAbs, it is a more useful clinical parameter, as it has the potential to inform treatment choice at the outset (i.e., radioiodine, surgery, or thionamide).
Longer time to normalization of TSH was consistently identified as a predictor of relapse across all time points, although not independently of age and TRAbs. “Time to normal TSH” may operate as a simple proxy of the rate of change in disease activity over time, perhaps akin to an earlier study where rate of fall of TRAbs across sequential measurement predicted relapse (8). Interestingly, the degree of biochemical thyrotoxicosis (as determined by diagnosis fT4 or TT3) was not associated with recurrence, which conflicts with earlier studies (7).
No significant influence was observed of male sex or smoking (not reported), but this may reflect the relatively small number of men in this cohort and incomplete smoking data. Another limitation of this study is the omission of a standardized assessment of goiter size, which has previously been shown to predict relapse risk (7). Similarly, thyroid eye disease has previously been identified as a risk factor for recurrence (19), but this was not included in our analysis. This partly reflects the fact that patients with moderate and severe ophthalmopathy often require prolonged courses of thionamide therapy, with ongoing evidence of disease activity, including persistently elevated TRAbs (19). This study does not include all patients commenced on thionamide, but rather all those where it was felt appropriate to discontinue therapy after a prescribed course, inevitably meaning that those with severe, persistent disease are not within the scope of this investigation. The influence of pregnancy, which has previously been associated with a significantly increased risk of relapse, was not assessed (20). Iodine status is also recognized as a factor influencing relapse rates and may limit the generalizability of findings from a single geographical area. A recent assessment of iodine status in the United Kingdom revealed iodine deficiency in 52–59% of girls aged 14–15 years in Scotland. Populations with significantly different iodine sufficiency levels may display different relapse characteristics (21).
Conclusion
This study provides useful information to guide appropriate primary therapy and, where thionamides are selected, follow-up after withdrawal. These data should help inform shared decision making when selecting a primary treatment for a first episode of Graves' thyrotoxicosis, and suggest stronger consideration of definitive therapy. In patients with very high TRAbs at presentation and significant cardiovascular risk, the near inevitability of recurrence suggests early recourse to definitive therapy. In patients completing a course of thionamide, clear information is provided on the time course and risk of recurrence, and consideration of long-term therapy is suggested where TRAbs are positive.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.