
Abstract
Background:
The study considered the long-term outcome of patients with papillary thyroid carcinoma treated with 30 mCi radioiodine.
Objective:
The aims of this study were to define and compare the remission rates of papillary thyroid carcinoma ablated with 30 mCi 131I prepared by either thyroid hormone withdrawal (THW) or recombinant human thyrotropin (rhTSH; Thyrogen®), and to identify variables predictive of a favorable prognosis.
Method:
An observational study was conducted at an academic medical center and a comparative summary of six studies is presented. Three hundred and seventy patients (THW group, n = 203; rhTSH group, n = 167) were recruited from a prospectively managed registry. The mean follow-up was 9.3 years (range 5.1–15.8 years) in the THW group and 7.1 years (range 5.0–9.7 years) in the rhTSH group. The primary endpoint was the long-term remission rates (no evidence of disease) in the THW group compared with the rhTH group.
Results:
The response at 12–18 months after 30 mCi remnant ablation was excellent in 79.3% and 76.0% of patients in the THW group and the rhTSH group, respectively (p > 0.05). The long-term remission rates also did not significantly differ between both groups at 95.6% and 97.0%. Although the surveillance period for the THW group exceeded that of the rhTSH group, no significant difference in recurrence-free survival was discerned by the Kaplan–Meier curves. In a multivariate analysis, an excellent response to therapy at 12–18 months correlated significantly with long-term remission rates in the THW group (p = 0.031, odds ratio [OR] = 2.6 [confidence interval (CI) 1.1–6.0]), the rhTSH group (p = 0.03, OR = 5.3 [CI 1.2–23.8]), and the pooled groups (p = 0.001, OR = 3.43 [CI 1.63–7.2]). The pre-ablation thyroglobulin level significantly correlated with remission rates only in the THW group (p = 0.035, OR = 5.5 [CI 1.1–27.1]).
Conclusions:
The response to remnant ablation with 30 mCi radioiodine is often excellent, and the long-term remission rates can be expected to be high, independent of the method of delivery (i.e., THW or rhTSH).
Introduction
D
Methods
A series of consecutive patients with PTC treated with 30 mCi 131I was extracted from a prospectively maintained registry from a single tertiary care center. Details of a portion of the early cohort of patients were previously reported (8). In summary, all the patients had a total thyroidectomy performed by high-volume thyroid surgeons, and after 6–12 weeks, the patients received 30 mCi radioiodine for remnant ablation. A low-iodine diet was started two weeks prior to the administered low activity, but the method of thyroidal stimulation changed with time. THW was used initially for the early cohort between 1998 and 2007, and then from 2008 onward, rhTSH was the preferred method of stimulation for this later cohort of patients. A preablation serum thyrotropin (TSH)-stimulated Tg level, anti-Tg titer, and neck sonography were obtained in all patients. All patients with anti-Tg antibodies were excluded from the study, since the association of preablation stimulated Tg to the final outcome was a secondary goal of the study. Seven to 10 days after the administration of 131I, a whole-body scan (WBS) was performed. The dose of levothyroxine was adjusted to maintain the TSH <0.1 mIU/L, and at 12–18 months after remnant ablation, the response to therapy was assessed with a rhTSH-stimulated Tg, anti-Tg antibodies, 4 mCi 131I WBS, and neck sonography. Yearly, active surveillance while on levothyroxine suppression included serum TSH, Tg, anti-Tg antibodies, and neck sonography. Abnormal results were followed by other cross-sectional modalities or functional imaging and tissue diagnosis when feasible. Only patients with at least five years of follow-up were retained for analysis because as previously reported in another study (9), most of the recurrences manifested in that interval. This study was approved by the hospital research Ethics Committee. Definitions of the response to therapy at 12–18 months followed the latest ATA guidelines (10): (i) excellent response—negative imaging and suppressed Tg <0.2 μg/L or stimulated Tg <1.0 μg/L; (ii) biochemical incomplete response—negative imaging and suppressed Tg >1 μg/L or stimulated Tg >10 μg/L; (iii) indeterminate response—nonspecific findings on imaging studies, nonstimulated Tg detectable but <1 μg/L, stimulated Tg detectable but <10 μg/L; (iv) structural incomplete response—structural or functional evidence of disease, with any Tg level.
Materials
Biochemistry
Thyrotropin was measured by an electrochemiluminescence immunometric assay (Elecsys® TSH Immunoassay; Roche Diagnostics, Indianapolis, IN) up to 1999, then with a TSH Thyrotropin Cobas assay (Roche Diagnostics) until the end of the study. Both assays had a functional sensitivity of 0.01 mIU/L and a reference value established in-house ranging from 0.4 to 4.5 mIU/L. Tg was first measured by a radioimmune assay (Kronus; USC Endocrine, Los Angeles, CA) with a functional sensitivity of 1 μg/L up to 2002. Afterward, Tg was measured by an immunometric assay (Immulite 2000 Thyroglobulin; Siemens, Los Angeles, CA) with a functional sensitivity of 0.9 μg/L. Anti-Tg antibodies were determined by a chemiluminescent assay (Immulite 2000 Anti-Tg Ab; Siemens) and considered negative when <20 IU/mL.
Nuclear medicine imaging methods
All patients were scanned using a dual-head Philips (Markham, Canada) Skylight camera, with a high-energy (364 KeV rated) collimator. Total body scans were taken at a scan speed of 6 cm/min using a continuous acquisition mode. A 512 × 1024 matrix was used. Both anterior and posterior views and spot views of the neck at 15 min/view were obtained using a pinhole collimator. Two nuclear medicine specialists interpreted the scans.
Neck sonography
Sonography was performed by the same operator (M.T.) with a linear multi-frequency 12–14 MHz transducer (General Electric, Fairfield, CT) for morphological analysis (B-mode) and for color Doppler evaluation. The thyroid bed and central and lateral compartments were examined for suspicious lesions and, if detected, submitted to ultrasound-guided fine-needle aspiration for cytology and Tg measurement in the needle washout fluid (11).
Statistical analysis
Categorical variables were summarized as frequency and percentages, whereas continuous variables were summarized as mean and standard deviation or median and range. Comparison between groups for categorical variables was done using the chi-square test, and for continuous variables using an independent sample t-test. Univariate and multivariate logistic regression models were used to estimate crude and adjusted odds ratios with confidence intervals. Kaplan–Meier analysis was used to plot the cumulative recurrence-free survival, and differences between curves were assessed by the log-rank test. All statistical analyses were performed using PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL). A two-sided p-value of <0.05 was considered statistically significant.
Results
In the cohort of patients prepared by THW at the time of ablation, 203/215 eligible patients were retained for analysis. Ten patients were lost to follow-up, and two patients died of lung cancer before attaining five years of surveillance data. In the cohort of patients prepared with rhTSH at the time of ablation, 167/194 eligible patients were retained for analysis. Twenty-four patients had incomplete data, and three patients died (renal cell cancer, glioblastoma multiforme, and complications arising from atrial fibrillation).
The patient demographics for the THW group, the rhTSH group, and the pooled group are summarized in Table 1. The mean age and the percent of females were comparable in the THW group and the rhTSH group. As expected, the mean follow-up period was longer for the THW group (9.3 ± 2.2 years; range 5.1–15.8 years) compared with the rhTSH group (7.1 ± 0.9 years; range 5.0–9.7 years). The proportion of patients with classical PTC histology, the individual American Joint Cancer Commission's tumor-node-metastasis categories (AJCC-TNM) (12), and the rates of microscopic extrathyroidal extension (ETE), multifocality, and vascular invasion did not significantly differ between both groups. The patients in this series did not undergo prophylactic central compartment lymph node dissection. The lymph nodes retrieved were berry-picked by the surgeons or included within the perithyroidal specimen. This strategy accounted for the relatively low rate of microscopic nodal disease (i.e., n = 35/356; 9.5%) in the pooled group. In the THW group, 50.7% were categorized as low risk and 49.3% as intermediate risk for recurrence (ATA recurrence risk stratification 2015) compared with 59.3% and 40.7%, respectively, in the rhTSH group.
AJCC, American Joint Cancer Commission; T, tumor; N, node; Nx, no nodes submitted; ETE, extrathyroidal extension; ATA, American Thyroid Association; rhTSH, recombinant human thyrotropin; THW, thyroid hormone withdrawal; Tg, thyroglobulin.
The response at 12–18 months to 30 mCi remnant ablation was excellent in 79.3% and 76.0% of patients in the THW group and the rhTSH group, respectively (p > 0.05 between groups). As most of the patients with elevated Tg levels and incomplete or indeterminate responses progressed to undetectable Tg levels without further treatment, the long-term remission rates also did not significantly differ between both groups at 95.6% and 97.0%. There were 86/356 (24.2%) patients with an incomplete/indeterminate response associated with complete remission at the end of the follow-up period. In this subgroup, 12 patients initially had microscopic nodal disease (pN1a) with one or two metastatic nodes. In one patient, 6/15 nodes harvested were positive for malignancy. There were only eight patients with radioiodine uptake outside the thyroid bed. None of these correlated with structural abnormalities on cross-sectional imaging, and all achieved remission at the end of the follow-up period. Although the surveillance period for the THW exceeded that of the rhTSH, no significant difference in recurrence-free survival was discerned by the Kaplan–Meier curves (Fig. 1). Whereas 12 patients with incomplete ablation were not in remission by the end of the study, only two patients, both in the intermediate risk category, who were successfully ablated at initial evaluation had recurrent disease at long-term evaluation (Table 2).
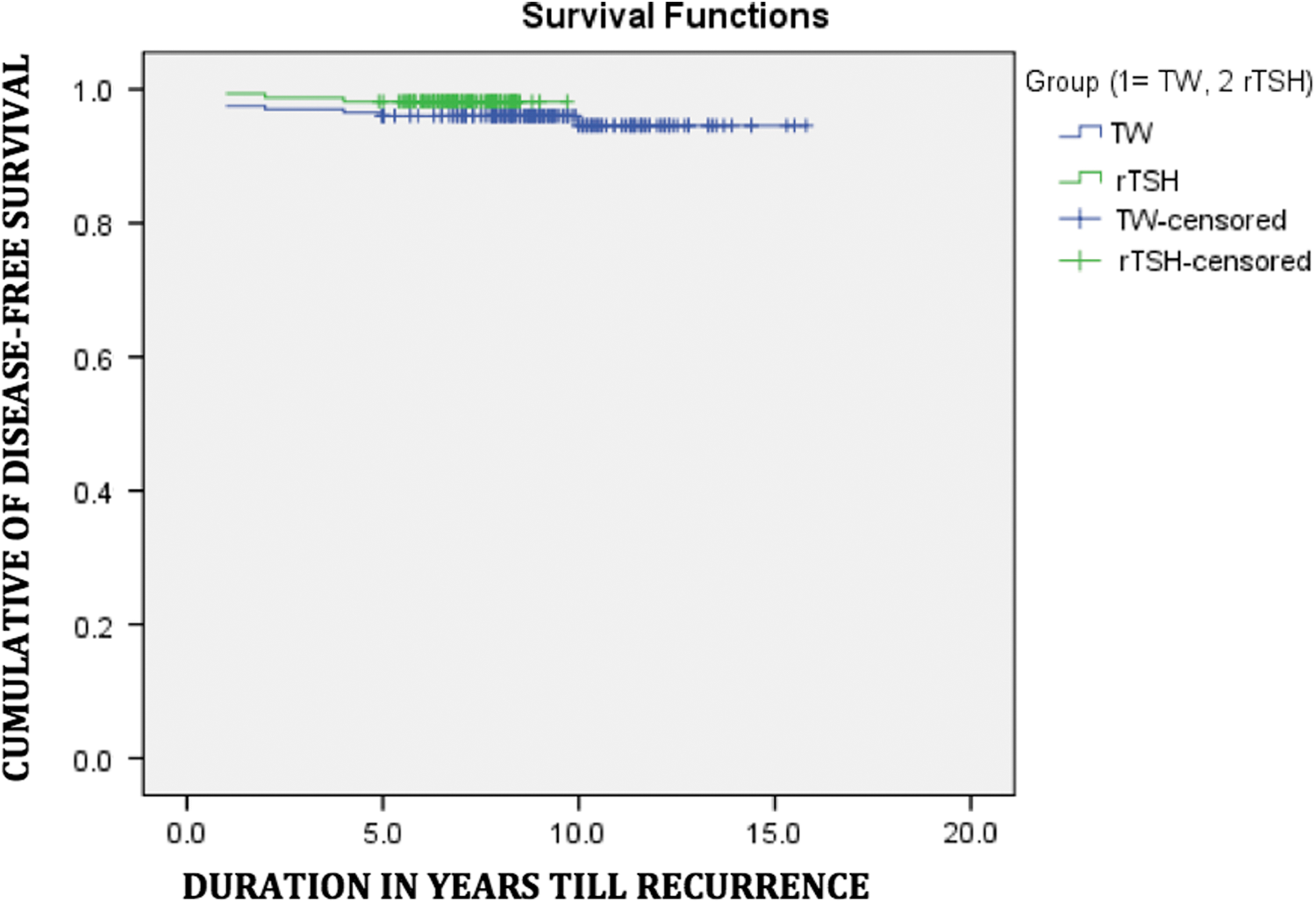
Kaplan–Meier curve showing time to recurrence in both the recombinant human thyrotropin cohort and thyroid hormone withdrawal (THW) cohort. Longer time of follow-up for THW did not result in higher recurrence rates. Color images available online at
As the final outcomes did not differ between both groups of patients, in both univariate and multivariate analyses, the patients were analyzed as a single group (pooled). To identify variables related to long-term prognosis, various factors were compared: age, sex, tumor histology and size, mETE, T stage, N stage, tumor multiplicity, and excellent response to therapy. In the pooled cohort of patients, variables that were significantly associated with remission in a univariate analysis included classical-type PTC (p < 0.001), absence of ETE (p < 0.006), and an excellent response to therapy (p < 0.001), but not the preablation stimulated Tg (p 0.161). In a multivariate analysis of these significant factors, an excellent response to therapy at 12–18 months correlated significantly with long-term remission rates in the THW group (p = 0.031, odds ratio [OR] = 2.6 [confidence interval (CI) 1.1–6.0]), rhTSH group (p = 0.03, OR = 5.3 [CI 1.2–23.8]), and pooled group (p = 0.001, OR = 3.43 [CI 1.63–7.2]). The preablation Tg level significantly correlated with remission rates only in the THW group (p = 0.035, OR = 5.5 [CI 1.1–27.1]). Indeed, patients with stimulated Tg levels <10 μg/L were 5.5 times more likely to be in remission.
Discussion
In a series of consecutive patients with low- and intermediate-risk PTCs undergoing remnant ablation with 30 mCi radioiodine, long-term remission rates were robust and did not differ between patients prepared with either THW or rhTSH. In a multivariate analysis, patients with an excellent response to therapy at 12–18 months following ablation were 3.4 times more likely to be in long-term remission in both groups. Furthermore, patients in the THW group with a preablation Tg <10 μg/L were 5.5 times more likely to be in remission. In the low-risk group, only patients with an incomplete response recurred. However, in the intermediate-risk group, two patients, despite an excellent response to therapy (complete ablation), had a late recurrence of structural disease.
There is a paucity of data reporting on the long-term remission rates of patients with PTC undergoing remnant ablation with 30 mCi radioiodine using modern criteria and methodology. Two randomized control trials have reported similar rates of ablation success among patients prepared with either THW or rhTSH, and receiving either 30 mCi or 100 mCi radioiodine (6,7). Until long-term outcomes from these two trials are available, we must rely on data gathered from observational studies to guide patient management. Table 3 summarizes the results of six studies, including the current report, describing outcomes of patients with differentiated thyroid carcinoma undergoing remnant ablation with 30 mCi radioiodine after an extended interval of active surveillance. Most studies prepared patients for remnant ablation with either THW or rhTSH, except the studies by Welsh et al. (5) and Kukulska et al. (2), which used only THW. A separate analysis of outcomes with either THW preparation or rhTSH preparation was available only for the present study, although pooled results were reported by Molinaro et al. (3).
TTX, total thyroidectomy; CLND, central compartment node dissection; DTC, differentiated thyroid cancer; BIR, biochemical incomplete response; SIR, structural incomplete response; SA, successfull ablation; UA, unsuccessfull ablation; WBS, whole body scan.
The long-term remission rates (i.e., no evidence of disease [NED]) for the pooled groups of patients varied among studies and ranged from 67.9% to 97.7% over a median of 24 years and 10 years, respectively. This variation could be related to the different characteristics and extent of disease, criteria used to express a disease-free state, and type/length of surveillance adopted. However, the three studies employing similar inclusion criteria, treatment, and modern surveillance modalities have reported comparable remission rates of 88.1% (3), 94.1% (4), and 96.2% in the present study. It is noteworthy to mention that the cohort of patients in the three studies included low-, intermediate-, and some high-risk patients without metastases. Across the studies, these patients responded equally well to low-activity remnant ablation, and the risk category did not factor as significant for prediction of remission.
In the four studies including this report, additional doses of radioiodine were not administered to patients with incomplete remnant ablation as defined by either scintigraphic or biochemical criteria. Nevertheless, the patients in these studies had favorable long-term outcomes, which correlated with initial successful ablation (excellent response). Indeed, as reported previously, ongoing risk stratification is a powerful tool to predict long-term recurrence rates, since 30–50% of patients with an excellent response to primary therapy could be downgraded (13,14). In the present study, response to primary therapy was the best predictor of outcome for patients prepared with either THW, or rhTSH, as well as in the pooled cohort. As previously reported by Vaisman et al. (15), this study also observed that patients with a biochemical incomplete response can be reclassified as having NED without additional therapy other than levothyroxine suppression. Nevertheless, these patients still require regular surveillance, since, as shown here, two of the intermediate-risk patients with an excellent initial response (successful ablation) experienced a late long-term recurrence. In the study with the longest follow-up, the overall survival at 10 years and 30 years did not differ significantly between the group of patients successfully ablated and those unsuccessfully ablated (87% and 81% vs. 77% and 62%, respectively; p = 0.154) (5). None of the deaths was considered attributable to thyroid cancer, a finding that is consistent with the current study. These results contrast with those reported by Verburg et al., who found a significantly higher thyroid cancer–specific mortality in the group at least 45 years old treated with <2000 MBq (54 mCi) compared with the group treated with 2000–3000 MBq (54–81 mCi) or >3000 MBq (>81 mCi; 15-year 16.1 ± 7.7%, 0.8 ± 0.8%, and 7.2 ± 5.5%, respectively; p = 0.004) (16). They strongly recommend against low-activity radioiodine therapy for purposes of remnant ablation in low-risk patients, especially those >45 years old. Although difficult to reconcile with the present data, the discrepancy reflects a problem with ascertainment of cancer-specific death. In addition, Schvartz et al. reported in a subgroup analysis that overall survival and disease-free rates did not differ significantly between low-risk patients who were treated with a standard dose of 100 mCi and those who received a low dose of 20 mCi (17).
A meta-analysis, including data from an early cohort of patients, showed that a low stimulated preablation Tg level (i.e., <10 μg/L) under conditions of THW predicted successful ablation (8,18). The data by Molinaro et al. (3) and the findings presented here show that a low stimulated preablation Tg level predicts a low recurrence rate in patients prepared with THW. Although a similar association of preablation Tg and successful ablation with rhTSH has been reported, this variable has not been found to be a predictor of remission (19). Spencer et al. reported that the rhTSH-stimulated Tg is determined by patient-specific factors, such as the TSH responsiveness of Tg-producing tissue (normal remnant and/or tumor tissue) and independent of sex, age, basal Tg, and the 72-hour TSH level (20) Furthermore, pharmacokinetic studies demonstrated that the highest mean Tg level was achieved more than two days after the second rhTSH injection, and then the mean values continued to increase on day 3 and declined on day 7 (21,22). Indeed, Melo et al. reported a positive correlation between preablation rhTSH-stimulated Tg levels and unsuccessful ablation rates when serum Tg levels were measured on the fifth day after the first injection (19). In our study, the preablation rhTSH-stimulated Tg was measured one day after the second injection, hence before peak values were attained. This difference in timing may have contributed to lack of an association.
In conclusion, 30 mCi can be used for the purposes of remnant ablation in patients with low- and intermediate-risk PTC. The response to therapy is often excellent, and the long-term remission rates can be expected to be high, independent of the method of TSH stimulation (i.e., THW or rhTSH). The preablation stimulated Tg level will not only predict response to therapy (ablation success), but also long-term remission among patients prepared with THW.
Footnotes
Author Disclosure Statement
The authors report that no competing financial interests exist.