
Abstract
Background:
The occurrence of nonthyroidal primary malignancy (NTPM) and the potential association of with radioiodine (RAI) treatment are important concerns in patients with differentiated thyroid cancer (DTC), but incidence data are conflicting. The aims of the present study were to investigate the incidence of NTPM and its association with RAI treatment in a cohort of DTC patients treated at a single tertiary medical center.
Methods:
The data of 1943 patients with DTC recorded in the Rabin Medical Center Thyroid Cancer Registry were cross-matched with data from the Israeli National Cancer Registry to identify those diagnosed with an NTPM. Patient medical files were reviewed. Second primary malignancy (SPM) was defined as new malignancy diagnosed at least two years after DTC diagnosis.
Results:
For 1434 of the 1943 patients (73.8%), the American Joint Committee on Cancer TNM stage was 1–2. The mean follow-up was 9.3 years. Of the 1943 patients, 1574 (81%) were treated with RAI, and 1467 were followed for at least 2 years, and of these, 1145 patients (78%) received a cumulative dose of ≤200 mCi. A total of 409 NTPMs were diagnosed in 368/1943 patients with DTC (18.9%; 265 female, mean age 53.9 ± 15 years), including 173 SPMs (42.3%) in 166/368 patients. The most common NTPM and SPM was breast cancer followed by hematologic malignancies. In patients followed for ≥2 years, SPMs were diagnosed in 9% of RAI-treated patients and 10.5% of non-RAI-treated patients. SPM rates were 10.2% and 7.8% for a cumulative RAI dose of ≤100 mCi and >100 mCi respectively. Hazard ratios for SPM in patients that received/did not receive RAI treatment was 1.27 (95% confidence interval 0.88–1.82; p = 0.1). There was no correlation between first or cumulative RAI dose and diagnosis of SPM.
Conclusions:
NTPMs are not uncommon in patients with DTC and usually antecede the DTC. In a population of mostly low-risk DTC patients, in whom limited activities of RAI are usually administered, this treatment is apparently not associated with an overall increased risk of SPMs compared with subjects not receiving RAI treatment.
Introduction
D
It has been suggested that DTC is associated with an increased risk for other primary cancers (3). However, incidence data are inconsistent and it is unclear whether this association is due to screening bias, treatment effects, or other factors.
Radioiodine (RAI; 131I) has been used for more than half a century for diagnostic purposes and for treating patients with hyperthyroidism and papillary or follicular thyroid carcinoma. In patients undergoing diagnostic testing or treatment for hyperthyroidism, the nonthyroidal tissues are exposed to only a low radiation dose, and there have been no findings of an increased radiation-linked risk of a second primary malignancy (SPM) (4 –6). However, much higher activities of 131I are needed to treat patients with thyroid cancer, raising concerns that RAI therapy may increase the risk of development of a second primary in patients with DTC who otherwise enjoy an excellent long-term survival. The possibility of a carcinogenic effect of RAI is particularly worrisome given the recent understanding that RAI should not be automatically administered to all patients with DTC after total thyroidectomy and that its potential harm should be taken into consideration in treatment decision making (7). However, studies seeking to resolve this issue have yielded conflicting results. Several authors reported that the risk of SPM is significantly increased in patients with DTC compared with the cancer risk in the general population (8 –10), whereas others found no relationship between 131I administration and the occurrence of SPMs (11).
The aim of the present study was to assess the prevalence of nonthyroidal primary tumors (NTPMs) in patients diagnosed with thyroid cancer and treated in a single tertiary medical center in Israel. Additionally, we compared the risk of acquiring SPMs in patients with thyroid cancer between those who received RAI treatment and those who did not.
Methods
We cross-matched the data of 1945 patients with DTC recorded in the Rabin Medical Center Thyroid Cancer Registry with data on the same patients from the Israel National Cancer Registry (INCR) to identify those with a diagnosis of NTPM. In Israel, reporting of all pathological diagnoses of malignancy in the population except nonmelanoma skin cancers is obligatory. However, since the diagnosis of hematological malignancies, specifically myeloproliferative malignancies and chronic leukemia, is not necessarily based on pathological specimens, their incidence is probably underestimated in pathological-based registries including the INCR. The medical records of the identified patients were reviewed and the following clinical variables were collected: patient age and sex, past history of NTPM, type and time of surgery, histopathology findings, RAI therapy, TNM staging, and additional treatments. Quality control of the registry data was performed by chart review and data verification on several occasions. All patients were monitored by standard methods, including clinical examination, thyroid function tests, neck sonogram, radioiodine scan, and measurement of serum thyroglobulin and antithyroglobulin antibodies. Some patients also underwent other radiological tests as necessary, including computed tomography, positron emission tomography, magnetic resonance imaging, and bone scan. An SPM was defined as a new malignancy if diagnosed at least 2 years after the diagnosis of DTC. For analyzing the risk for SPM associated with RAI, we included only patients that were followed for ≥2 years prior to data collection and compared the SPM incidence in patients treated/not treated with RAI.
The numerical data are expressed as mean ± standard deviation and the categorical data, as n (%). For numerical data, we used independent t-test or the nonparametric Mann-Whitney test to analyze differences between two independent subgroups, and one-way analysis of variance or the nonparametric Kruskal-Wallis test to analyze differences among more than two subgroups. For categorical data, we used Fisher's exact test to analyze differences between two subgroups and chi-square test to analyze differences among more than two subgroups. Time to diagnosis of SPM was analyzed by the Cox proportional hazards model with application of the Fine and Gray methodology to account for competing risks (12). Cumulative 131I dose was entered into the Cox model as a time-dependent covariate. The statistical analysis for this paper was generated using SAS software, version 9.4 (SAS System for PC, copyright 2002–2012).
Results
The cohort included 1943 DTC patients with a mean follow-up of 9.3 ± 9.6 years (range 0–62 years, median 6). Three hundred and sixty-eight patients (18.9%) had an INCR diagnosis of NTPM; 37 patients had 2 NTPMs and two had 3, for a total of 409 NTPMs. One hundred seventy-three NTPMs in 166/1943 patients (8.5%) were diagnosed 2 years or more after the diagnosis of DTC and were therefore considered second primaries (SPM). Of these, 14 patients had a diagnosis of NTPM both before and after the diagnosis of DTC (Fig. 1). The mean follow-up period in patients with SPM was 17.4 ± 12 years (median 15, range 2–62 years). Of these, patients that received RAI were followed for 16.4 ± 11.3 years after DTC detection (median 13, range 2–62) and patients that were not exposed to RAI were followed for 20.1 ± 13.9 years (median 13, range 2–43). SPMs were detected 12.9 ± 10.9 years after DTC diagnosis (median 10, range 2–59 years).
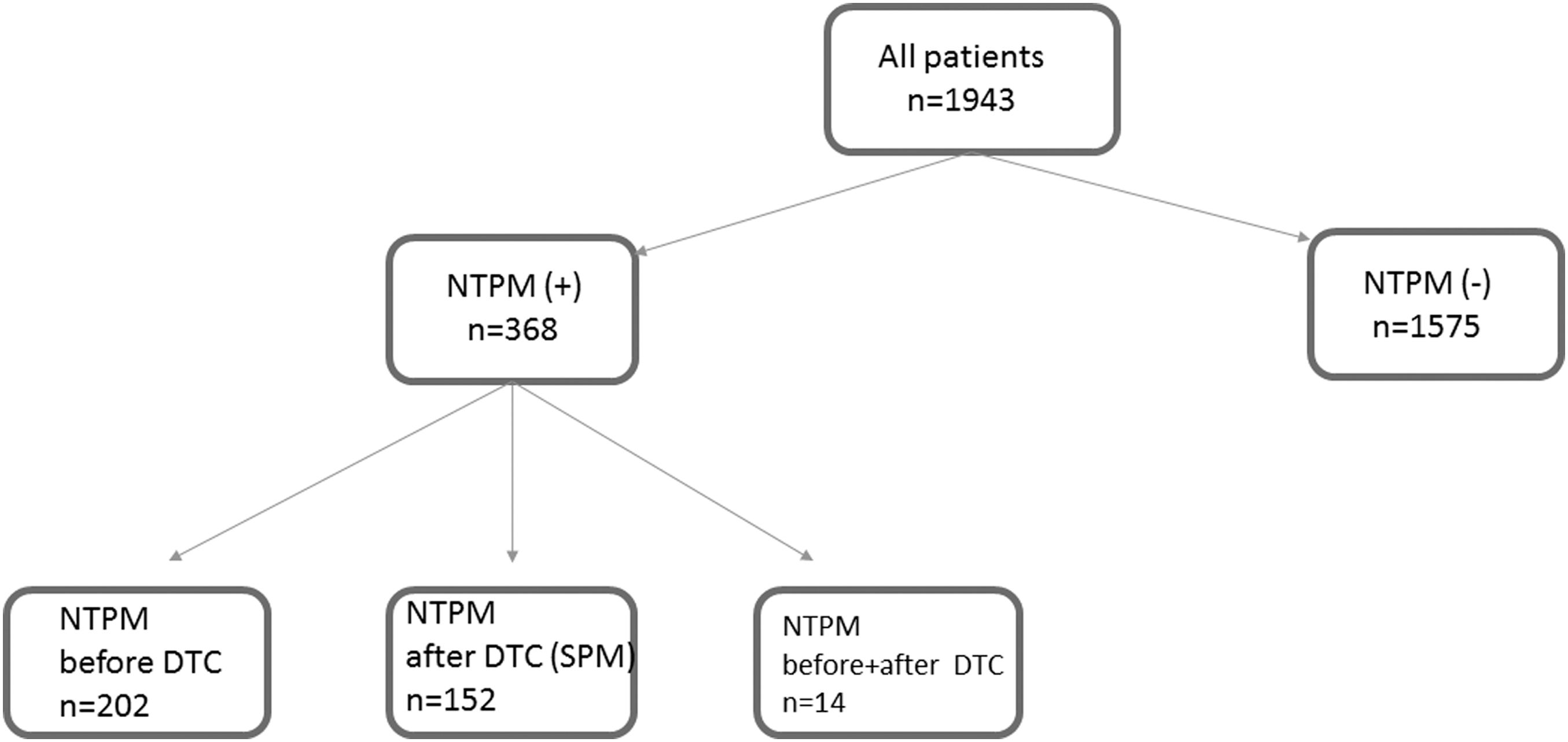
Patients’ categories according to diagnosis of nonthyroidal primary malignancy (NTPM) and second primary malignancy (SPM) detected at least two years after diagnosis of differentiated thyroid cancer (DTC).
The characteristics of all patients and of those with/without NTPM diagnosis are shown in Table 1. Patients who were diagnosed with NTPM were older and have been followed for a longer period of time than those with no NTPM.
NTPM, nonthyroidal primary malignancy; PTC, papillary thyroid carcinoma; PTCFV, PTC follicular variant; RAI, radioactive iodine.
Data on patients who were diagnosed with NTPM prior to DTC diagnosis or with SPM are shown in Table 2.
Fourteen patients who were diagnosed with NTPMs both before and after DTC diagnosis were excluded.
DTC, differentiated thyroid cancer; NS, not significant; SPM, second primary malignancy (NTPM diagnosed at least two years after DTC detection).
The sites of all NTPMs (and SPMs) are presented in Table 3: 101 (and 49) were located in the breast and 53 (and 20) were hematological malignancies, followed by cancers of the gastrointestinal system, urinary system (renal cell carcinoma/transitional cell carcinoma), melanoma, prostate, lung, and others. In all sites except the prostate and lung, the proportion of NTPMs diagnosed before DTC (57.7%) was equal to or higher than the proportion diagnosed after DTC.
Radioiodine data were unavailable for 5 patients (5 SPMs); * p = 0.217, ** p = 0.296.
Hematologic: ALL (n = 3), CLL (n = 5), CML (n = 2), lymphoma (n = 38 including 14 patients with Hodgkin's), multiple myeloma (n = 3), polycythemia vera (n = 2), malignant histiocytoma (n = 1).
Gastrointestinal (GI) system: colon (n = 41), gastric (n = 2), esophagus (n = 1), gallbladder (n = 1).
Others: parathyroid, medulloblastoma, angioenotelioma, or not otherwise specified.
CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia.
Treatment data were available for 1912 patients, including 1574 (82.3%) who received RAI and 338 (17.7%) who did not. For analyzing the association between RAI therapy and SPM occurrence, we included 1792 patients with follow-up duration of ≥2 years. Of these, 618 patients (34.5%) were followed for <5 years and 396 (22%) for ≥15 years. Of the 1574 patients treated with RAI, 1467 (93.8%) were followed for at least 2 years prior to SPM data collection. Overall, 558/1467 patients (38%) received ≤100 mCi and 1145 (78%) received ≤200 mCi. Only 6 patients were treated with ≥1000 mCi. Among the 166 patients with a second primary, 161 (168 SPMs) had available data on RAI treatment; 132 received RAI and 29 did not (Fig. 2).
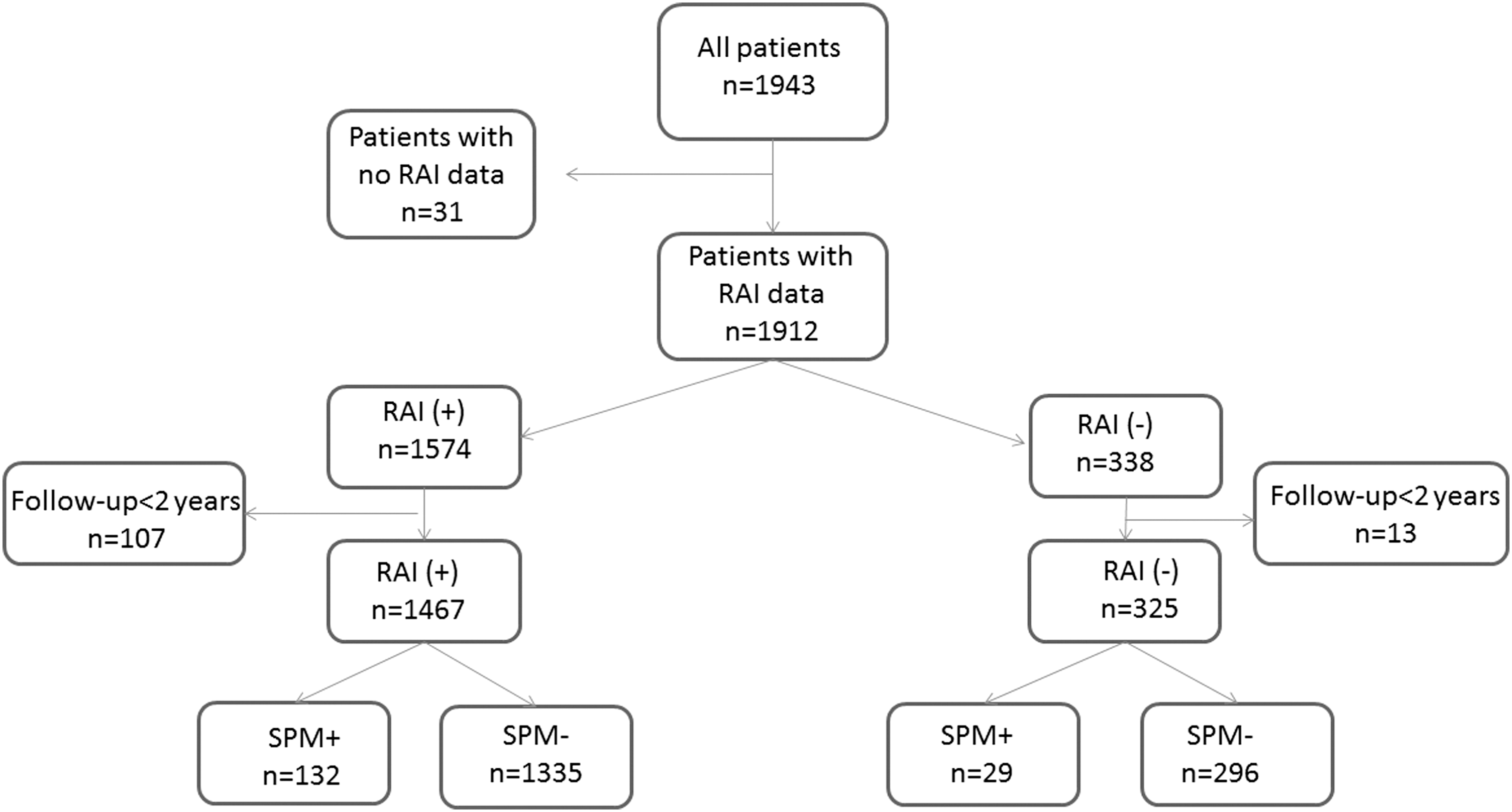
Patients’ categories according to radioactive iodine (RAI) treatment and a diagnosis of second primary malignancy detected at least two years after thyroid cancer diagnosis (SPM).
Table 3 shows the incidence of NTPMs and SPMs per site and SPM diagnosis in RAI-treated and untreated patients (135 SPMs and 33 SPMs respectively).
One hundred thirty-two RAI-treated patients were diagnosed with SPM. The data for RAI-treated patients with/without SPM are summarized in Table 4. SPMs were diagnosed in 9% of RAI-treated patients and 10.5% of non-RAI-treated patients after a follow-up of ≥2 years. The SPM rate after a cumulative dose of ≤100 mCi and >100 mCi was 10.1% (56/557) and 7.8% (71/910) respectively. After a cumulative dose of ≤200 mCi and >200 mCi SPM occurrence was 8.2% (94/1145) and 10.2% (33/322) respectively. The mean first dose was 103 ± 49 mCi in the patients with a second primary and 116 ± 45 mCi in the patients without a second primary; the corresponding mean cumulative doses were 186 ± 172 mCi and 170 ± 134 mCi.
One hundred seven patients without SPM were excluded due to follow-up period greater than two years.
No significant correlation was found between the first or cumulative RAI dose and the diagnosis of SPM. The hazard ratio for SPM was one per 1 mCi increase for both the first and cumulative RAI activities [confidence interval (CI) 0.99–1.01]. The hazard ratios for SPM in patients after the first RAI treatment compared to patients with no RAI treatment, adjusted for age and sex, was 1.27 ([CI 0.88–1.82], p = 0.1). Similarly, no increased risk was found with increasing cumulative RAI activity by dose category (Table 5).
Thirty-five RAI-treated patients were excluded, including five patients with SPM, due to missing data on cumulative RAI dose.
Discussion
The present study shows that approximately one out of five thyroid cancer patients treated at our medical center was diagnosed with another primary cancer, either prior to or after DTC detection. Yet, with a mean follow-up period of 9.3 years, we found that in thyroid cancer survivors, RAI therapy is not associated with an increased risk of SPM.
The 18.9% incidence of NTPMs in DTC patients found in this study is higher than the 12.3–14.2% reported by others (3,13). Although this difference may be explained by specific genetic or environmental factors in the Israeli population, it might also be related to our use of the INCR rather than hospital files as a data source to determine NTPM incidence, such that the probability of our missing a malignant diagnosis was very low.
In our study, more than half the NTPMs (56.8%) were diagnosed prior to the diagnosis of DTC. In most sites, the proportion of NTPMs diagnosed before DTC was higher than or equal to the proportion of those diagnosed after DTC. This type of bidirectional association between cancers, described also by others (3), raises the possibility of shared genetic or environmental risk factors rather than a carcinogenic effect of RAI.
In accordance with other authors (8,9,13,14), we found that the most common site of the second malignancy in our population was the breast, accounting for 27.3% of all NTPMs (101/409). Some studies have suggested an increased incidence of breast carcinoma in women with thyroid carcinoma (9,15), and RAI therapy has been proposed as risk factor (16). By contrast, others showed that the risk was not associated with the administration of RAI (17). In an Israeli study evaluating the development of both thyroid and breast cancer in the same patients, the authors found an elevated risk for DTC after breast cancer (standard incidence ratio [SIR] 1.34 [CI 1.03–1.72]) and SIR of 1.07 for the risk for breast cancer after thyroid cancer (18). In the present cohort, the number of patients diagnosed with breast cancer before and after DTC diagnosis was similar.
We did not find an association between RAI therapy and an increased risk of SPM. Furthermore, we were unable to show a dose–response relationship between RAI treatment and SPM risk. These findings are at variance with some previous studies, both in cohorts and population based, that demonstrated a significant increase in the incidence of SPM among patients with DTC who received RAI treatment compared with those who did not (8,9,19). Yet, other studies showed no association between RAI therapy and the risk of SPM (20 –22), similar to our findings.
There are several factors that may explain the difficulty in elucidating the true incidence of SPM in patients with DTC and its association with RAI administration. The first is the absence of a uniformly accepted definition of SPM, with the pre-set lag from diagnosis of DTC ranging from 2 months (9, 23) to 2–3 years (11, 24) in different studies. Analysis of SPM risk using a permissive definition may be hampered by a statistical surveillance bias. In an Israeli survey, the relative risk for a second primary in the breast after thyroid cancer was highest during the first year of follow-up and gradually declined thereafter (18). Similarly, Ronckers et al. (23), in a SEER-based analysis, found that the highest risk for a diagnosis of SPM was seen in the first year after DTC diagnosis. Since the usual latent period attributed to radiation-induced carcinogenesis is long, the reported high risk of a second primary within a short time after DTC diagnosis points to a cause other than RAI. It is more likely associated with surveillance bias. In the present study, we defined a second primary as a cancer diagnosed at least 2 years after diagnosis of DTC. Using this criterion, we found that our patients with DTC had an overall risk of 8.5% of acquiring a second primary (9% after exclusion of patients with follow-up <2 years). This rate is in agreement with previous reports (8,9,19).
Another factor is the need for long-term follow-up of a large number of patients to estimate the incidence of SPM. The largest study to date of the association of DTC with the risk of SPM included 178,844 patients derived from a nationwide, population-based cancer registry in Korea (10). A total of 2895 patients (1.6%) were diagnosed with subsequent second primary malignancies. The median duration of follow-up was 3 years for all patients and 5.8 years for patients with second cancers (10). The authors found that the median latency period from the initial diagnosis of thyroid cancer to the diagnosis of SPM was 3.3 years. The elevated risk of SPM normalized after 10 years of follow-up for most cancer sites. In the present study, the incidence of SPM diagnosis was much higher (8.5%) and this may be explained, at least partly, by the longer duration of surveillance (a median of 6 and 8 years for all patients and patients with NTPMs respectively). Furthermore, in patients with SPM, follow-up length (median: 15 years) was considerably longer than that of the whole cohort and SPM were diagnosed after a median period of 10 years after DTC detection. Thus, it may be speculated that a longer follow-up period would have resulted in an even higher SPM risk.
Finally, large epidemiological (9) or nationwide surveys (10) are highly powered to detect differences in SPM incidence between patients with DTC and the general population. At the same time, data on RAI in these larger studies are usually either limited to yes/no information (3,9,22,23) or are lacking altogether (10). Thus, institutional reports that provide detailed data on study populations including RAI treatment have an important role in revealing a possible association between RAI administration and SPM risk.
In the only meta-analysis on the risk of SPM in patients with DTC after RAI treatment published to date (11), Sawka et al. reported that patients who were treated with RAI had a small absolute excess risk of acquiring a second primary relative to patients who were not treated with RAI (1.19; [CI 1.04–1.36]). Although this meta-analysis comprises only two studies, one from Europe and the other from North America (8, 9), both are large multicenter studies that include 37,119 patients. The North American study (9) was a SEER-based analysis of 30,278 patients diagnosed with DTC from 1973 to 2002. The relative risk analysis of RAI-associated SPM included 9661 patients (4248 treated with RAI). The findings showed a slightly increased overall risk of developing a SPM (SIR 1.09; [CI 1.05–1.14]). However, the SEER database does not include information on RAI dose activity. Furthermore, prior analyses using the same SEER database (3,22,23) during overlapping periods yielded varying results. For example, Bhattacharyya and Chien (22) analyzed the data of 29,231 patients with DCT in 1988–2001 (10,349 treated with RAI). On multivariate analysis, hazard ratios were significant only for age and male sex (1.052 and 1.438 respectively; p < 0.001), with no effect of the use of RAI. Our findings are in accordance with these results, regarding both the impact of age and sex on SPM occurrence and the neutral effect of RAI.
In our study, a significant portion of the patients with DTC received repeated RAI treatment. Analysis of the hazard ratio for developing a SPM by cumulative RAI dose showed no significant association. Only a few authors have previously addressed the possible dose–response effect of the cumulative activity of RAI on SPM occurrence. Khang et al. (25) and Fallahi et al. (24) in surveys from Korea and Iran respectively, reported that a cumulative RAI dose of <37 GBq (1000 mCi) did not increase the risk of SPM. In our study, 221 patients received ≥300 mCi (11.1 GBq), with no statistically significant increased risk for a SPM (Table 5). However, only 6 patients received ≥37 GBq (1000 mCi).
In a recent population-based study from Taiwan by Teng et al. (14), 602 cases of SPM were identified among 20,235 thyroid cancer patients (3.4%) with a median follow-up of 5.9 years. A cumulative RAI dose greater than 150 mCi possessed a statistically significant risk for all cancer combined (hazard ratio [HR] 1.3) and leukemia (HR 6.03). The authors did not find an increased HR of other specific cancer types including breast cancer (HR after >150 mCi, 1.09 [CI 0.63–1.9]). In the present study, we did not specifically analyze the risk of leukemia due to the probable underestimation of its incidence in the INCR and the small number of cases. It is also noteworthy that in the survey by Teng et al. the incidence of SPM was considerably lower than the 9% reported in our study with a similar median follow-up period of 6 years.
The impact of repeated RAI treatments was also investigated in a large multicenter European survey from Rubino et al. (8). The total number of patients with thyroid cancer was 6481, of whom 4225 received RAI; mean duration of follow-up was 13 years. A total of 576 patients (8.9%) were diagnosed with SPM. The authors found an increased risk of both solid tumors and leukemia with an increase in the cumulative activity of RAI and established a dose-dependent effect, which implies causality (8). However, there was an increased relative risk for a diagnosis of SPM for only four types of cancers including leukemia (115 of the total 576 SPMs). Of these, 57 patients (50%) were diagnosed with female genital cancer, but the risk for this cancer was not significantly increased compared to the general population, either overall (SIR 0.7 [CI 0.5–1]) or for the subgroup treated with RAI (SIR 0.9 [CI 0.6–1.3]). Additionally, it should be noted that the authors detected an increased risk for second solid-tumor primaries only when cumulative doses of RAI were as high as >7.4 GBq (200 mCi) with no evidence for excess risk in the majority of patients that were exposed to lower RAI doses (8). In our study, 73.8% of the DTC patients had AJCC TNM stage 1 or 2 disease and 78% of the RAI- treated patients received ≤200 mCi. Thus, our results are actually in agreement with the findings of Rubino et al. of no excess risk for SPM in patients exposed to this range of RAI activity.
The present study has strengths and limitations. The strengths include the fairly large number of patients with detailed information regarding DTC diagnosis, RAI treatment and occurrence of NTPMs prior to or after DTC detection. The mean follow-up period of 9.3 years is relatively long. Yet, exploring the full consequences of RAI on the incidence of tumors with a long latency period probably requires an even longer surveillance. Additionally, since the increased risk of SPM after RAI found by other authors was small (11), it is possible that our sample size was not big enough to detect it, especially in the subgroup of patients that received a high cumulative RAI dose. Thus, while our study did not find an increased risk for SPM after RAI administration, it cannot exclude this association. Still, though the generalizability of our findings to high cumulative RAI activity is restricted, the study has particular relevance for the large proportion of low risk DTC patients. Finally, we did not specifically analyze the risk of leukemia after RAI due to its probable underestimation in the INCR and the small number of patients.
In conclusion, NTPMs are not uncommon in patients with DTC and they antecede DTC in most cases. In a population of mostly low risk DTC patients treated with limited dose activities of 131I (most under ≤200 mCi), the risk of SPM was not significantly different in DTC patients treated with 131I compared to those not treated with 131I after a mean follow-up period of 9.3 years.
Footnotes
Acknowledgments
We would like to thank Dr. Barbara Silverman and Dr. Irena Liphshitz from the Israel National Cancer Registry for crossing the data of our patients with their records.
Author Disclosure Statement
The authors have nothing to disclose.