
Abstract
Background:
Radioactive iodine (RAI) is widely used in the management of differentiated thyroid cancer (DTC). The impact of the time interval between total thyroidectomy (TT) and RAI administration on disease outcome remains controversial. The objective of the present study was to evaluate the impact of the time interval between TT and RAI.
Methods:
This study evaluated a cohort of DTC patients who received RAI therapy for whom data on disease status were available. Patients were allocated to one of two groups, according to the time interval between TT and RAI. “Disease-free” was defined as no clinical, imaging, or biochemical evidence of thyroid cancer.
Results:
The study included 545 individuals. The TNM stages were: 322 (59.1%) patients in Stage I, 62 (11.4%) in Stage II, 65 (11.9%) in Stage III, and 82 (15.0%) in Stage IV. The median time interval between TT and RAI was six months (P25–75: 3–10 months). Patients were allocated to one of two groups according to RAI timing administration: group A ≤6 months after TT (median 3 months; n = 295), or group B >6 months after TT (median 10.5 months; n = 250). There were no differences for sex, histological type, tumor size, distant metastasis, or RAI dose between the groups (p > 0.1). Patients in group B were older (47.1 vs. 43.1 years; p = 0.02), had less cervical metastasis (73.6% vs. 59.3%; p = 0.002), and were more commonly classified as low ATA risk (48.0% vs. 36.6%; p = 0.027). One year after initial therapy, 59.3% and 65.6% of patients in groups A and B, respectively, were considered disease-free (p = 0.15). Remarkably, the percentage of patients classified as disease-free was similar, even when analyzing a subgroup of high-risk patients (n = 72; 9.5% vs. 10.0%; p = 1.0). These findings did not change after a median of six years of follow-up. Accordingly, further analysis by multiple logistic regression showed that timing of RAI was not associated with persistent disease (relative risk 0.97 [confidence interval 0.80–1.19]).
Conclusions:
Timing of RAI does not seem to interfere with the disease outcomes in DTC and can therefore be safely planned while taking into account the health system logistics.
Introduction
D
RAI has been used for the postsurgical treatment of DTC for >50 years. The goals of the first dose of RAI administration after TT are the ablation of thyroid tissue remnants and/or irradiation of neoplastic disease (adjuvant therapy). A more controversial objective is to facilitate surveillance using serum thyroglobulin (Tg) measurement. While these goals are important, the ultimate endpoint of postsurgical ablation is to minimize undesirable outcomes of DTC such as persistent disease and recurrence.
The time interval between TT and RAI administration is mostly determined by the patient's access to medical facilities for RAI dosing, especially for patients who need higher doses and require hospitalization. The impact of this time interval on disease outcome is still a matter of debate. In a retrospective analysis of 198 high-risk patients, Japanese researchers found that the risk of death was 4.22 times higher in DTC patients who received the first RAI dosing >180 days after TT compared with those who received the initial therapy within 180 days (6). On the other hand, in low-risk patients, this time interval does not seem to impact on six-month remission rates (88% vs. 91.2% for early or late RAI therapy, respectively) (7).
Assessing the impact of RAI therapy timing is critical in planning treatment for those patients who need this therapeutic modality. Therefore, the objective of the present study was to evaluate the impact of the time interval between TT and RAI administration on disease outcome in a cohort of DTC patients attending a referral center.
Material and Methods
Patients and study design
This study evaluated a cohort of DTC patients who consecutively attended the Thyroid Outpatient Clinic of the Endocrine Division of Hospital de Clínicas de Porto Alegre (HCPA), a tertiary care university teaching hospital in southern Brazil, from 2000 to 2015. All patients with a histological diagnosis of DTC who received RAI therapy were included. Patients who were lost to follow-up after the initial therapy were excluded.
Treatment protocol and follow-up
The DTC treatment protocol consisted of performing TT, administering an ablative or therapeutic dose of RAI, as indicated, and levothyroxine suppression therapy. Decisions regarding cervical lymph node dissection were made at the discretion of the surgical team at the center where the patients underwent the first surgery. Duration of follow-up was defined as the time between the TT and the last medical visit to the clinic.
The ablation protocol used RAI activities prescribed at the discretion of the attending physician. According to the current Brazilian Nuclear Medicine legislation, the administration of RAI doses >49.9 mCi requires hospitalization, and at the HCPA, admissions for RAI dosing follows a close-fitting preschedule agenda (only two nuclear medicine RAI rooms). Thus, RAI therapy was recommended immediately after surgery, and the time interval between TT and RAI administration was solely determined by the patient's access to medical facilities and availability of RAI for administration. A low-iodine diet was prescribed for two weeks before the RAI administration until two days afterward. The dose was administered in a stimulated thyrotropin (TSH) condition with endogenous hypothyroidism (TSH >30 mIU/L) after withdrawing levothyroxine (at least three to four weeks without thyroid hormone). A post-therapy whole-body scan (WBS) was performed 7–10 days after RAI administration.
In the first evaluation, the following data were recorded for each patient: patient demographics, tumor characteristics (e.g., the date of diagnosis, histological features, extension, and lymph node involvement) and treatment (e.g., surgery, RAI, and other interventions). Each patient was classified using the 7th edition of the TNM/AJCC staging system (I, II, III, or IV) (8). N0 status was defined considering the clinical examination of the neck, preoperative and postoperative neck ultrasound (US) imaging, macroscopic examination during surgery, and pathological examination of patients with lymph node resection. The baseline tumor stage and the risk for persistent/recurrent disease were also defined based on the proposed classification using the 2009 American Thyroid Association (ATA) guidelines (2).
The follow-up protocol called for an initial assessment at three to six months after the initial treatment, which included a physical examination of the neck and measurements of the serum Tg levels under TSH suppression (Tg-T4) and antithyroglobulin antibody (TgAb). In a second evaluation, 6–12 months after the initial treatment, serum Tg under a stimulated TSH condition on endogenous hypothyroidism (TSH >30 mIU/L; sTg) and TgAb were measured. Neck US was also performed in this first year of follow-up. At this point, the patient was classified according to his or her response to initial therapy (see the outcomes section below), and the patients who were classified as disease-free were scheduled for annual visits, during which a physical examination of the neck and measurements of Tg-T4 and TgAb were performed. Patients with persistent disease were scheduled for the same examination twice a year. Additional imaging studies (e.g., dx-WBS, computed tomography [CT]) were performed, as needed, whenever the clinical or laboratory findings raised the suspicion of persistent or recurrent disease.
Outcomes
In the first year of follow-up, the response to initial therapy was assessed based on the serum Tg or sTg levels, neck US, post-RAI WBS (whenever available), and additional imaging exams, whenever indicated. “Disease-free” was defined as having no clinical or imaging evidence of tumor (i.e., no uptake outside the thyroid bed on the post-treatment WBS, and no imaging evidence of tumor on neck US), undetectable (<1 ng/mL) serum Tg-T4 levels, and sTg levels <2 ng/mL.
Persistent disease was subdivided into biochemical or structural disease. Biochemical disease was defined as Tg-T4 values ≥1 ng/mL or sTg levels ≥2 ng/mL, without structural evidence of disease. Structural disease involving cervical lymph nodes was defined by evidence of disease on imaging studies or biopsy-proven disease (cytology or histology), with or without abnormal Tg values. Patients who were diagnosed with persistent disease were evaluated for additional treatment (e.g., surgery, radioiodine, and external-beam radiation), depending on the site involved.
Recurrence was defined as new biochemical or structural evidence of the disease detected in a patient who had been previously determined to be disease-free. In patients with positive TgAbs, the trend of the serum TgAbs levels over time was used, as well as additional imaging studies to define the disease status. Patients with rising levels of TgAbs and/or structural disease on imaging studies were classified as having persistent disease. Patients with stable or declining TgAbs and absence of structural disease were classified as disease-free. For those patients in whom the TgAbs became negative on follow-up, the Tg criteria were used.
Laboratory analysis
Serum Tg measurements were conducted using immunoradiometric assays (from 2000 to 2002, radioimmunoassay; from 2002 to 2010, electrochemiluminescence; and from 2010 until the present, chemiluminescence) with functional sensitivities of ≥1 ng/mL. TgAbs were measured using the passive agglutination method from 2000 to 2010 and by chemiluminescence from 2010 until the present. After each new technique had been implemented, the necessary procedures for standardization and validation were performed. TSH levels were measured by electrochemiluminescent immunoassay (ADVIA Centaur XP; Siemens, Tarrytown, NY). These tests were all conducted in the central laboratory of the HCPA.
Statistical analysis
The clinical and laboratory data are reported as the mean ± standard deviation (SD) values or as the median and 25th and 75th percentiles (P25–75) for continuous variables, or as absolute numbers and percentages for categorical variables. Comparative analyses were performed using an unpaired Student's t-test, Mann–Whitney U-test, or chi-square test, as appropriate.
Generalized linear models with a log link and Poisson errors were used to estimate the impact of the time between TT and RAI. Variables with a p-value of <0.10 in the univariate analysis were included in the multivariate models.
All tests were two-tailed, and all analyses were performed using IBM SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). A two-tailed p-value of <0.05 was considered statistically significant.
Results
Patients
From a cohort of 901 patients, 545 individuals were evaluated based on inclusion and exclusion criteria (Fig. 1). Clinical and oncological characteristics of the included patients are described in Table 1. The mean patient age at the time of diagnosis was 44.9 ± 15.1 years, and 436 (80.0%) were women. PTC was diagnosed in 464 (85.1%) patients. The median tumor size was 2.0 cm; 186 (34.1%) patients had lymph node metastases, and 50 (9.2%) patients had distant metastases. The TNM/AJCC classifications were: 322 (59.1%) Stage I, 62 (11.4%) Stage II, 65 (11.9%) Stage III, and 82 (15.0%) Stage IV. The TNM/AJCC stage was unknown for 14 patients. According to the ATA classification, the risk level was low in 228 (41.8%) patients, intermediate in 245 (45.0%) patients, and high in 72 (13.2%) patients.
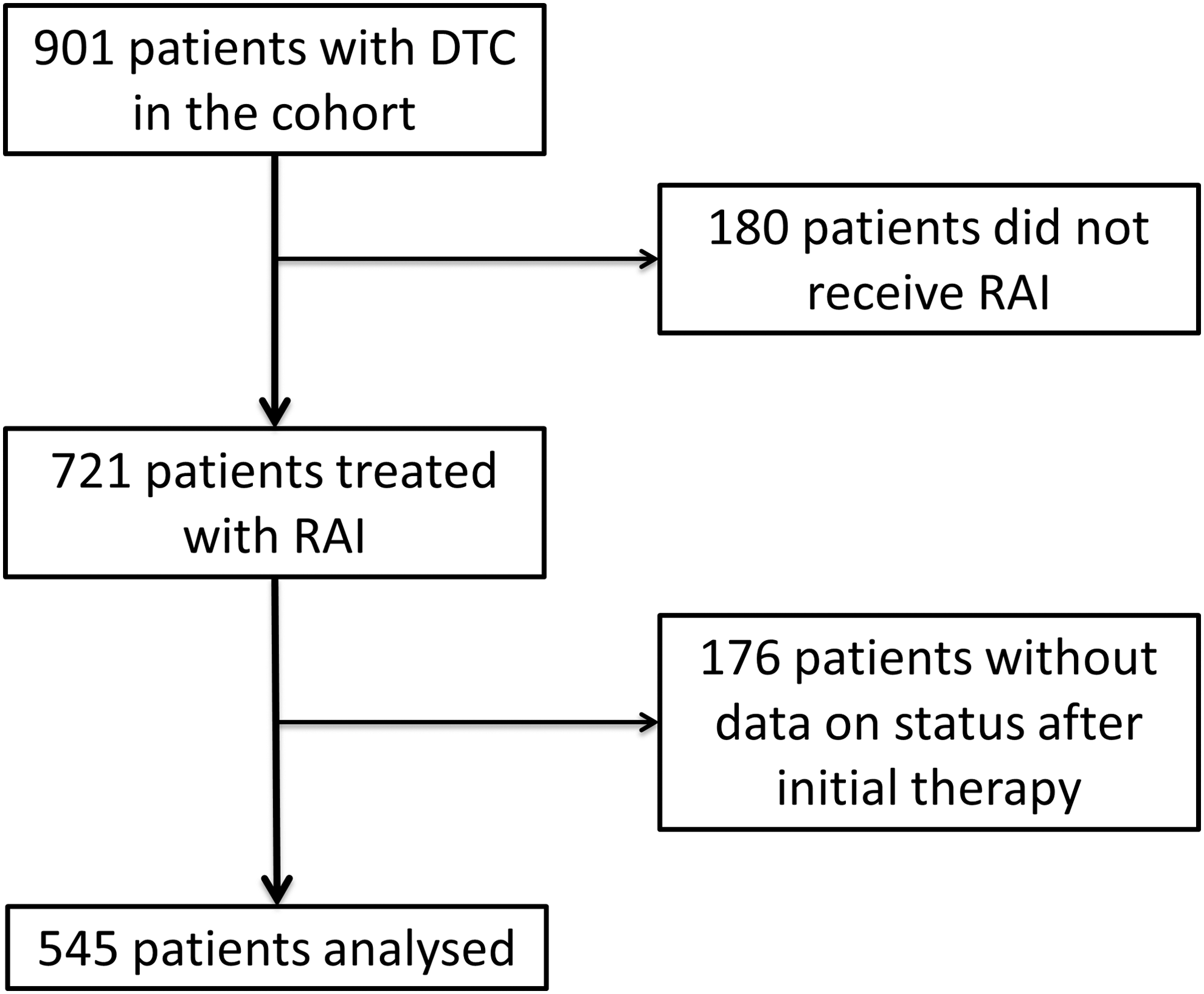
Flow chart of the study.
Data are expressed as mean ±SD, median (25th–75th percentiles), or frequencies.
The tumor size was unavailable in these patient subgroups (all patients were >45 years of age).
TNM/AJCC, TNM staging system of the American Joint Committee on Cancer; ATA, American Thyroid Association; RAI, radioactive iodine; SD, standard deviation.
All patients underwent TT and neck dissection, as indicated. The mean ablative or therapeutic RAI dose was 112.3 ± 38.1 mCi (range 30–250 mCi). Post-therapy WBS was performed in 503 patients: 20 (3.9%) showed no uptake, 448 (89.2%) presented only cervical uptake, and 35 (6.9%) had distant metastases.
Impact of RAI timing on clinical outcomes
The median time interval between TT and RAI was six months (P25–75: 3–10 months). To investigate whether the timing of RAI administration had an impact on the response to the initial treatment, the patients were assigned to one of two groups, according to the time interval between TT and RAI: group A ≤6 months after TT (n = 295), or group B >6 months (n = 250). The median time interval in group A was three months (P25–75: 2–5 months), and in group B it was 10.5 months (P25–75: 8–16 months). There were no differences for sex, histological type, tumor size, distant metastasis, or RAI dose between the groups (p > 0.1). Patients in group B were older (47.1 vs. 43.1 years; p = 0.002), had less cervical metastasis (73.6% vs. 59.3% classified as N0; p = 0.002), and were more commonly classified as low ATA risk (48.0% vs. 36.6%; p = 0.027; Table 2).
Data are expressed as mean ± SD, median (25th–75th percentiles), or frequencies.
ATA, American Thyroid Association; RAI, radioactive iodine; TT, total thyroidectomy.
One year after the initial therapy, 59.3% (n = 175) of patients in group A and 65.6% (n = 164) in group B were considered disease free (p = 0.15; Fig. 2). These findings did not change after a median of six years of follow-up (63.3% of the patients were disease free in group A vs. 67.7% in group B; p = 0.31; Fig. 3). Next, the impact of the time interval between TT and RAI administration on the recurrence rates was considered. There were no differences in the recurrence rates between the groups (5.4% vs. 3.0% for groups A and B, respectively; p = 0.39).
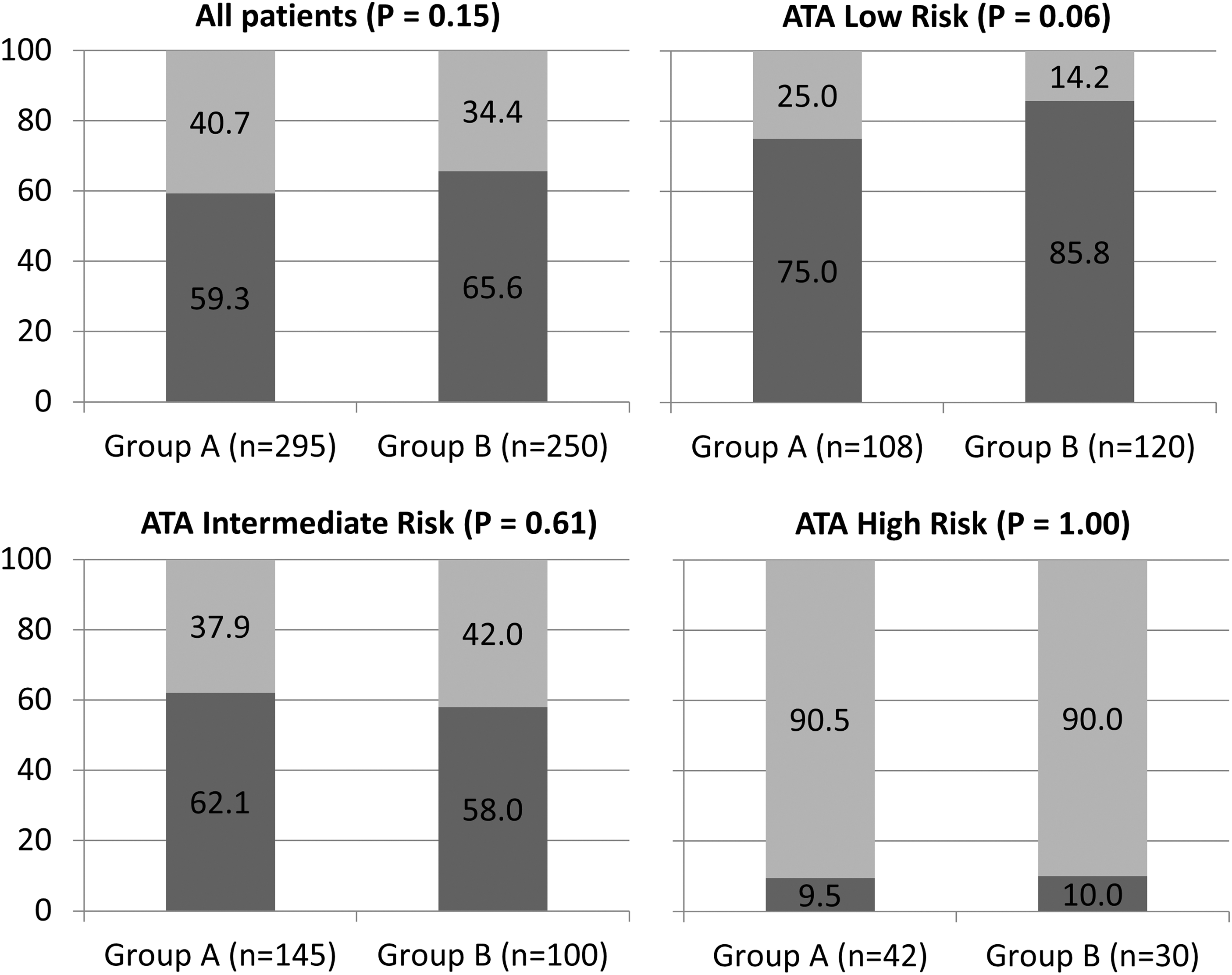
Status after initial therapy regarding time between total thyroidectomy (TT) and radioactive iodine (RAI) administration. Group A: ≤6 months (median 3 months). Group B: >6 months (median 10.5 months). Dark-gray bars: patients classified as disease free. Light-gray bars: patients classified as persistent disease.
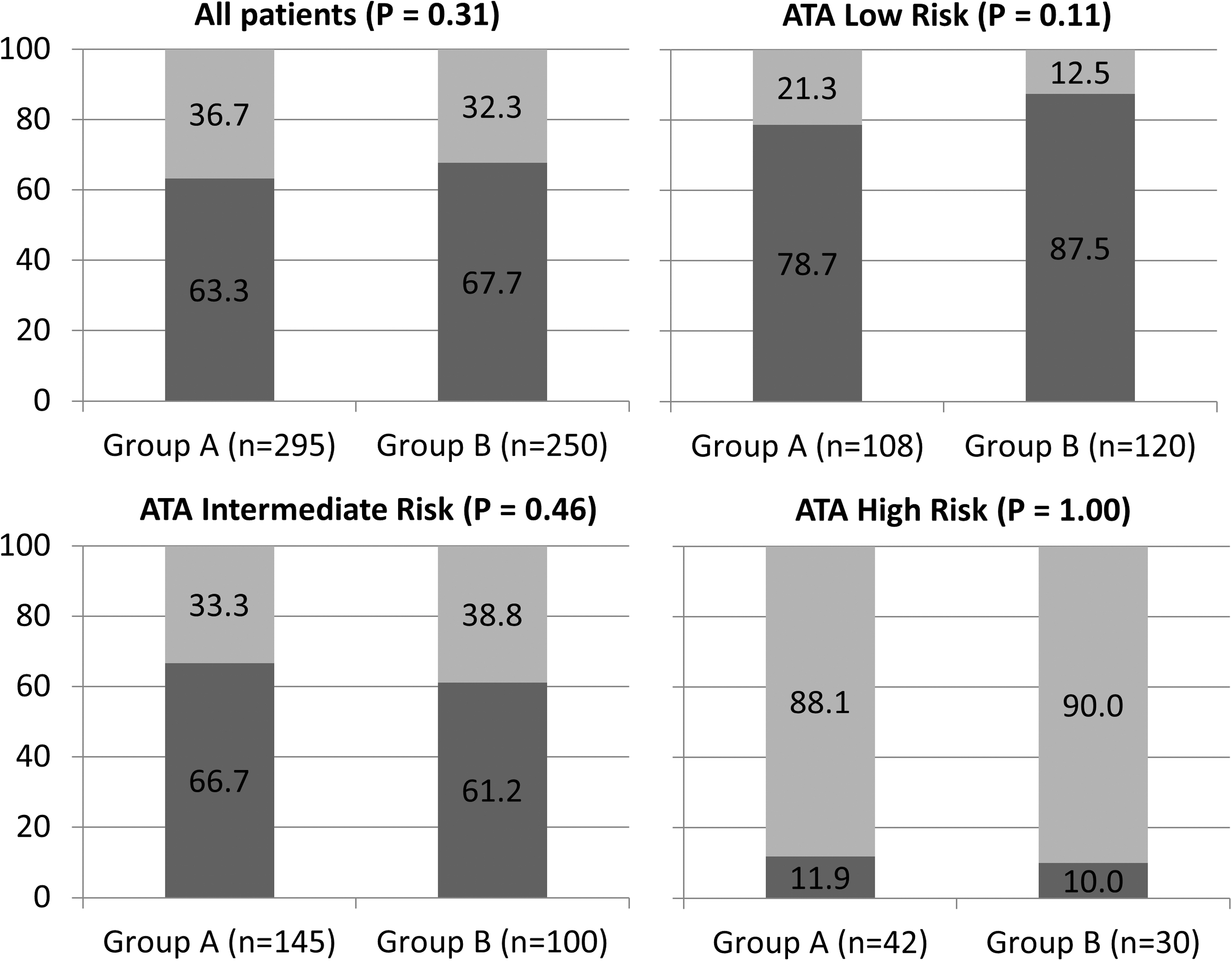
Status after median follow-up of six years regarding time between total TT and RAI administration. Group A: ≤6 months (median 3 months). Group B: >6 months (median 10.5 months). Dark-gray bars: patients classified as disease free. Light-gray bars: patients classified as persistent disease.
The lack of impact of RAI timing was observed across all ATA risk classification categories (Figs. 2 and 3), including patients classified as high risk (macroscopic tumor invasion or incomplete tumor resection or presence of distant metastases). Remarkably, in those patients, the rate of individuals considered as disease free after initial therapy was 9.5% and 10.0% in groups A and B, respectively (p = 1.00; Fig. 2). Similar results were observed after a median of six years of follow-up (Fig. 3).
To explore further the role of timing of RAI on disease outcome, patients who received RAI within the first quartile (i.e., ≤3 months; n = 148) were compared with those in the fourth quartile (i.e., >10 months; n = 125). No differences were observed in the prevalence of disease-free status after the initial treatment (59.5% vs. 58.8%; p = 0.75) or after six years of follow-up (62.6% vs. 61.3%; p = 0.92). Multivariate analyses using disease status after initial therapy as dependent variable and age, cervical metastasis, ATA risk (p < 0.10 in the univariate analysis), and time between TT and RAI as independent variables, showed that the time between TT and RAI was not associated with persistent disease after initial therapy (Table 3).
RR, relative risk; CI, confidence interval.
Because a significant number of patients were referred to our center after the thyroidectomy, the data about lymph node dissection/lymph node metastasis was partially/or not available for 185/545 patients included. To assess whether the lack of this information would introduce a bias and influence the results, the effect of the timing of RAI on the outcome of the 360 patients with information about lymph node metastasis status provided by the surgical report was also analyzed. Of these 360 patients, 174 (31.9%) had no cervical metastasis (N0), 36 (6.6%) had metastasis to the central compartment (N1a), and 150 (27.5%) had metastasis to the lateral lymph node compartments (N1b). The results were similar to those obtained when all patients were included in the analysis: group B patients (received RAI >6 months) had less lymph node metastasis than those in group A (42.3% vs. 56.6% of patients classified as N0 in groups B and A, respectively; p = 0.02). To exclude a further potential effect of the surgical procedure on the results, the impact of the time between TT and RAI dosing on the group of patients who underwent surgery at the HCPA was analyzed, all of them operated by the same surgical team (n = 224). Again, there was no impact of the timing of RAI (65.2% vs. 71.0% of disease-free patients in groups A and B, respectively; p = 0.51).
Discussion
RAI therapy is widely used in the management of DTC patients. However, the impact of the time interval between TT and RAI administration on the response to treatment remains a matter of discussion. This study demonstrates that timing of RAI administration is not the primary determinant of DTC outcome, at least if administered within the first year after TT. This finding was consistent across all categories of TNM stage and ATA risk stratification.
The benefits of RAI treatment have been extensively discussed in the last few years. Evidence from retrospective studies (9,10) and a meta-analysis (11) has suggested that RAI ablation is associated with a reduction in the 10-year risk of recurrence and mortality rate. In contrast, other studies have observed no benefit, particularly for low-risk patients, as recently demonstrated by meta-analyses (12,13). Another matter of discussion is the activity of RAI administrated, with recent trials showing the equivalence of efficacy between low and high doses (14,15). Surprisingly, the impact of the RAI timing on disease outcome has not been evaluated, even though it is an important issue when planning the treatment logistics. Indeed, only two studies were found that have focused on the impact of this treatment variable. Accordingly, the current DTC guidelines have no recommendations about the timing of RAI dosing (1 –3). Nevertheless, concerns about the best timing for RAI administration are shared among patients and physicians in clinical practice.
The present study evaluated the impact of timing of RAI treatment on DTC outcome in a large cohort of patients followed in a tertiary, university-based hospital. It should be noted that RAI therapy was recommended immediately after surgery for all patients, but due to the limited access to medical facilities and availability of nuclear medicine rooms, patients usually have to wait several weeks or months to receive RAI. The study shows that timing to RAI therapy after TT has no impact on the rate of persistent disease or recurrence after surgery. Importantly, this observation was consistent across all categories of TNM stage and ATA risk stratification. These findings contrast with those reported by Higashi et al. (6), which may be partially explained by significant methodological differences. First, the Japanese study only included patients with advanced disease (patients <45 years old with distant metastases or >45 years with at least Stage III DTC), while the present study included patients covering the whole spectrum of the disease. Second, in the prior study, the average interval between TT and RAI therapy was 2.59 years, while in this study it was only six months, which could better reflect current practice patterns in the care of patients with DTC. Of note, a very high mortality rate was observed in the Japanese cohort (15.6% of DTC-related deaths). A previous study by Tsirona et al. (7) also failed to demonstrate an impact of time to RAI on outcomes. However, the authors only included patients with low-risk DTC.
This study has some limitations that must be noted. First, this is a retrospective study without a control group in a cohort being followed prospectively. The groups, when divided using the median time between TT and RAI, showed some demographic differences. Patients in group B were older, presented less frequently cervical metastasis, and were more commonly classified as low ATA risk—differences that could potentially bias the results. Nevertheless, even in the logistic regression (when the analysis was controlled for these differences), there was no impact of the timing of RAI on disease outcomes. Because a significant number of patients were referred to the HCPA after the surgical procedure, another potential limitation is the lack of information about the lymph node dissection procedure. However, the results did not change when only those patients with complete data in the surgeons report were analyzed, or when only the subgroup of patients who underwent surgery at the HCPA by the same surgical team were analyzed.
On the other hand, this study has several strengths. All patients included were followed at a single institution, which ensures a similar therapeutic approach and follow-up strategy, thereby enhancing the validity of the data. It should be noted that the time interval between TT and RAI administration was solely determined by the patient's access to medical facilities and availability of RAI for administration, consistent with pragmatic, effective research. Moreover, the inclusion of ATA risk categories enhances the external validity of the findings.
In conclusion, this study shows that the time between TT and RAI dosing does not impact disease outcomes (response to initial therapy, disease status on follow-up, and recurrence rate) in patients with DTC. These findings are valid for all ATA risk categories, including high-risk patients, and may have some important clinical implications. First, patients can be reassured that the RAI therapy, whenever indicated, can be safely administered at any time within the first year after thyroid surgery. Most importantly, concerns about early RAI therapy are not justified, and RAI administration may be safely planned according to the logistics of the local health system and the patient.
Footnotes
Acknowledgments
This work has been made possible due to grants from CNPq, CAPES, FIPE, and PRONEX/FAPERGS. We wish to thank the surgeons at our hospital, Dr. Alceu Migliavacca, Dr. José Ricardo Guimarães, and Dr. Diego Mossmann, for surgical management of our patients.
Author Disclosure Statement
R.S.S., A.B.Z., J.M.D., and A.L.M. have nothing to declare.