
Abstract
Background:
Patient education and psychosocial support to patients are important elements of comprehensive cancer care, but the needs of thyroid cancer survivors are not well understood.
Methods:
The published English-language quantitative literature on (i) unmet medical information and (ii) psychosocial support needs of thyroid cancer survivors was systematically reviewed. A librarian information specialist searched seven electronic databases and a hand search was conducted. Two reviewers independently screened citations from the electronic search and reviewed relevant full-text papers. There was consensus between reviewers on the included papers, and duplicate independent abstraction was performed. The results were summarized descriptively.
Results:
A total of 1984 unique electronic citations were screened, and 51 full-text studies were reviewed (three from the hand search). Seven cross-sectional, single-arm, survey studies were included, containing data from 6215 thyroid cancer survivor respondents. The respective study sizes ranged from 57 to 2398 subjects. All of the studies had some methodological limitations. Unmet information needs were variable relating to the disease, diagnostic tests, treatments, and co-ordination of medical care. There were relatively high unmet information needs related to aftercare (especially long-term effects of the disease or its treatment and its management) and psychosocial concerns (including practical and financial matters). Psychosocial support needs were incompletely met. Patient information on complementary and alternative medicine was very limited.
Conclusions:
In conclusion, thyroid cancer survivors perceive many unmet information needs, and these needs extend to aftercare. Psychosocial information and supportive care needs may be insufficiently met in this population. More work is needed to improve knowledge translation and psychosocial support for thyroid cancer survivors.
Introduction
P
The objective of the present study was to conduct a systematic review of the published English language literature, examining (i) the unmet information needs and (ii) the unmet psychosocial support needs of adult thyroid cancer survivors. The results of this review are intended to illuminate care gaps and guide future development of patient education and supportive care programs.
Materials and Methods
Eligibility criteria for studies
This study systematically reviewed published English-language quantitative studies examining unmet information and psychosocial support needs of individuals diagnosed with thyroid cancer. The focus was on studies of individuals diagnosed with thyroid cancer who were adults at the time of they were studied, but there was no restriction on the age at which the original diagnosis of malignancy was made (i.e., childhood or adulthood). There was also no restriction on the histologic type of thyroid cancer, stage of disease, or time frame in the disease/survivorship trajectory. Unmet needs were identified from the patient perspective, using quantitative methods (such as surveys or interview questions). Unmet needs in partners or family members of thyroid cancer survivors were not examined. Individual case reports, unpublished works, or conference proceedings (in the absence of a full-text paper) were not eligible for inclusion in this study. Non-English studies were also excluded due to a lack of resources available for translation. Furthermore, if two or more studies reported overlapping relevant data from the same research study, only the largest and most recent paper reporting the outcomes of interest was included.
Search for relevant studies
A librarian information specialist (R.F.) searched seven electronic databases in December 2014 and September 2015, including: Ovid MEDLINE (beginning 1946), Ovid MEDLINE In-Process and Other Non-Indexed Citations (from inception), EBM Reviews—Cochrane Central Register of Controlled Trials (from inception), EBM Reviews—Cochrane Database of Systematic Reviews (from inception), Embase (beginning 1974), PsycINFO (from 1806), and CINAHL (from inception). The search terms used in the search are listed in the Supplementary Appendix (Supplementary Data are available online at
Study selection
Two reviewers (Y.G.H. and A.M.S.) independently screened the citations from the electronic search, and any citation that was deemed potentially relevant was retrieved in full-text form for formal review. Two reviewers (Y.G.H. and A.M.S.) also independently reviewed the full-text papers that were obtained from the electronic search or the supplemental hand search. At the full-text review stage, each reviewer indicated whether each study was eligible for inclusion, and if it was not, a reason for exclusion was indicated. Any discrepancies between reviewers on inclusion of studies in the review were resolved by re-review of the studies and discussion between the reviewers. If a consensus could not be achieved by discussion, a third party (D.P.G.) was available to finalize the decision. Ultimately, there was a final consensus between reviewers (and, if needed, the third party) on the papers included in the review.
Data collection process and critical appraisal of studies
Two reviewers then independently critically appraised and abstracted the data from the included papers using abstraction forms developed for this study (the available abstractors included two clinical endocrinology trainees [A.A., A.S.G.], an endocrinologist [A.M.S.], and a research assistant [A.N., in the Acknowledgements]). Any data abstracted by a research assistant was also independently abstracted by an endocrinology investigator (A.A., A.S.G., or A.M.S.) to ensure clinical context consideration. The tools planned to be used to appraise studies critically included either the Cochrane Risk of Bias Tool (11) for systematic reviews, trials, or comparative studies, or the Center for Evidence-Based Management Critical Appraisal of a Survey tool (12) for single-arm survey studies, depending on the study design of the included paper. The latter (12) was selected as a Cochrane Risk of Bias Tool was not available to appraise single-arm survey studies critically. Consensus was achieved for the critical appraisal and abstracted results between reviewers, and the results were tabulated and summarized descriptively. In the event of any questions of consensus on critical appraisal or abstracted data, a third party (D.P.G.) was available to resolve any conflicts. The systematic review results, including a figure showing study flow, were reported as per PRISMA recommendations (13).
Analysis of results
The results were summarized descriptively. Pooling of data was not planned, given the anticipated heterogeneity of data-collection tools (various questionnaires or interviews). The level of agreement was estimated between reviewers by calculating a kappa statistic (with confidence intervals [CI]) for the following data: (i) relevance of citations from the electronic search for full-text review, (ii) inclusion of reviewed full-text papers in the study, and (iii) methodologic critical appraisal. The kappa statistics were estimated using Confidence Interval Analysis Software v2.2.0 (T.N. Bryant, PhD, University of Southampton). For data on unmet information needs, given the heterogeneity of questionnaires and variety of topics encompassed within these questionnaires, two reviewers independently identified relevant themes, and consensus was achieved between reviewers on theme category. The information needs data were then descriptively presented according to theme category. Given the overlap of data relating to unmet information needs on psychosocial issues and unmet psychosocial support needs in the included studies, these data are summarized together.
Results
Summary of the results of study selection
The two reviewers independently screened 1984 unique citations obtained from the electronic search. Subsequently, a total of 51 full-text studies (14 –64) were reviewed for consideration of inclusion in the study. Of the full-text studies reviewed, 48 originated from the electronic search (14 –16,18,20 –63) and three from the hand search (17,19,64). Seven studies were included in the systematic review (14 –19,64). The level of agreement between reviewers at the electronic citation review stage was estimated by a kappa statistic of 0.515 [CI 0.346–0.684], and at the full-text review stage, the kappa statistic for agreement was 0.516 [CI 0.230–0.803]. The flow of study selection is summarized in Figure 1.
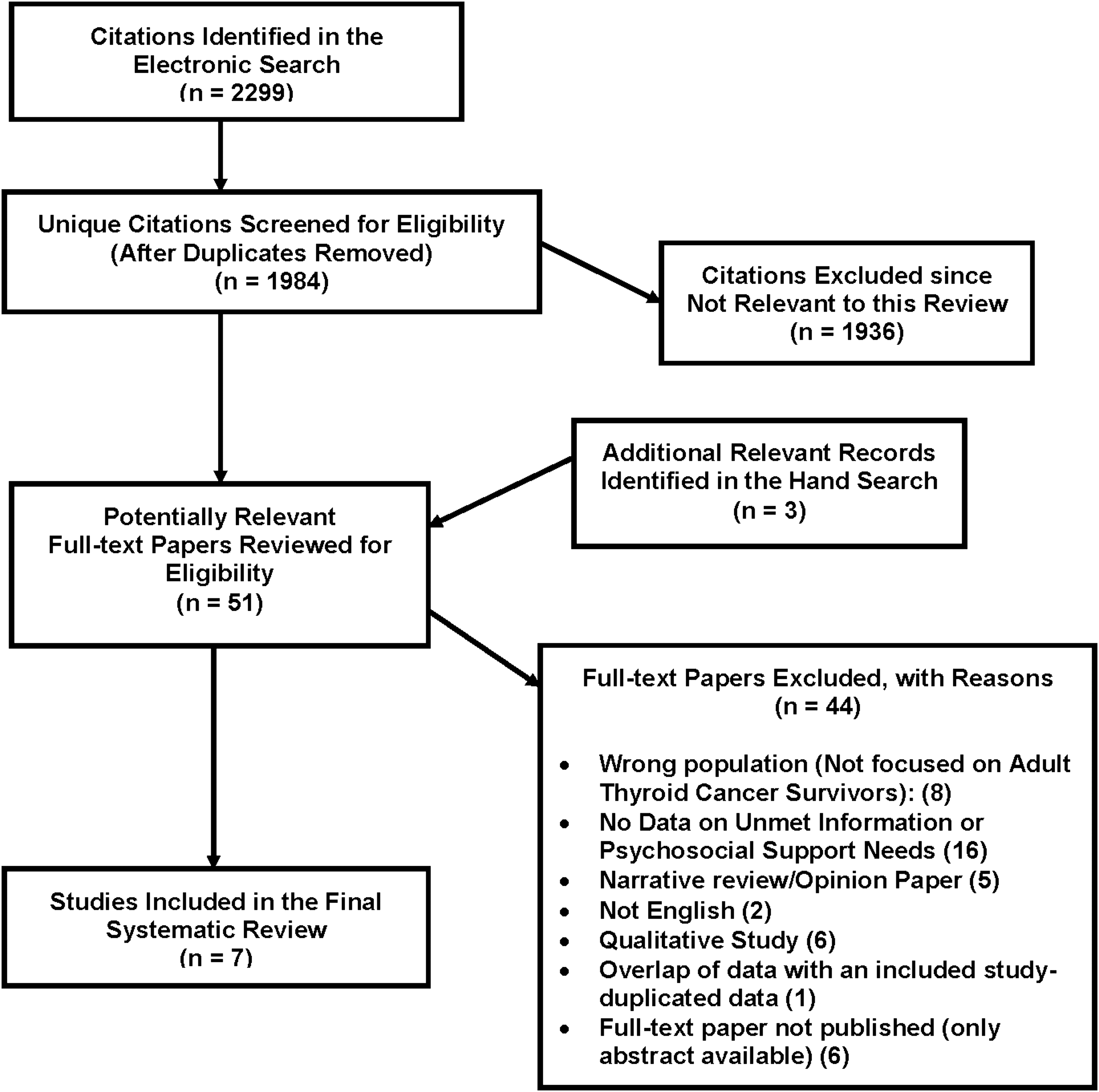
Flow diagram summarizing the process of study selection.
Characteristics of the included studies
The seven included studies were all cross-sectional, single-arm, patient-directed survey studies (Table 1) (14 –19,64), and the total number of respondents included in studies in this review was 6215 thyroid cancer survivors (for either outcome of unmet information or psychosocial support needs). The surveys were administered by a variety of methods, including online via the Internet (14,15,17,64), paper-based questionnaire (14,15,18,64), in-person interview (14,16), or telephone interview (19). The respective study sizes ranged from 57 (19) to 2398 (14) thyroid cancer survivors, with the three largest studies including an Internet component that was available through thyroid cancer patient support groups (14,17,64). The survey response rates ranged from 33.7% (16) to 86.2% (15), and three of the studies that were available freely on the Internet could not report response rates (14,17,64). One study received funding from industry (14), another three from private or hospital foundations (18,19,64), a fourth was unfunded (17), and two others did not report funding sources (15,16).
In keeping with the general epidemiology of thyroid cancer, the majority of participants were female in the studies reporting sex (14 –17,19,64), and other demographic characteristics are summarized in Table 2. The education level of participants was reported in five studies (15,16,18,19,64), and higher education (i.e., university or vocational school or more than 12 years/high school education) was reported between 26.2% (15) and 91.2% (19) of study respondents. In studies reporting on histopathologic type of thyroid cancer, papillary thyroid cancer was the most common (Table 2) (14,15,18,19,64). The clinicopathologic disease stage at diagnosis was reported in three studies, and in all of these, low-risk disease was the most prevalent category (15,19,64). In another study not specifically reporting other details of disease stage, distant metastatic disease was reported by a minority of respondents (14.1%) (14). The duration of time from diagnosis or initial treatment of thyroid cancer was variable, but the majority of participants within included studies were beyond the first treatment year (14,17,18,19,64). Furthermore, in a cancer registry study, a mean of 9.6 years (standard deviation [SD] = 5.6 years) had elapsed since the initial diagnosis (15). The prevalence of therapeutic radioactive iodine use (including remnant ablation, adjuvant radioactive iodine, or treatment of residual or persistent disease) was variable, ranging from 28.1% (19) in a study of low-risk patients to 100% in a study focusing on patients receiving low-dose outpatient radioactive iodine treatment (16). Information on the current disease status, including history of recurrent or persistent thyroid cancer, was reported in only two studies (14,19), and the prevalence ranged from 1.8% in a small study of low-risk patients (19) to 14.1% (338/2398) in a study that did not restrict inclusion based on clinicopathologic stage of disease (14).
History of therapeutic radioactive iodine for thyroid cancer includes either remnant ablation, adjuvant radioactive iodine, or treatment of suspected or known residual or recurrent disease.
Staging system reference from the original publication: UICC 2002 TNM Classification of Malignant Tumours (6th ed.), Wiley-Liss, New York.
SD, standard deviation.
The level of agreement between two reviewers using the Center for Evidence-Based Management Critical Appraisal of a Survey tool (12) was estimated by a kappa statistic of 0.615 [CI 0.415–0.778] for all of the 12 questions shown in Table 3. Ultimately, both reviewers achieved consensus on the critical appraisal for all categories as summarized in Table 3. All of the included articles were subject to various methodological limitations, such as a lack of reporting of statistical power justification for sample sizes in all studies (Table 3) (14 –19,64). Three of the studies utilized questionnaires that had been subject to some validity testing either within the current study or referenced in previous studies (15,18,19), and in one study, a validated quality-of-life questionnaire was combined with additional questions (including those on information and support needs), but it was not clear whether the additional questions or combined questionnaire was validated (64).
Not for the outcomes of unmet information and psychosocial support needs.
Results of the included studies: unmet information needs
Theme 1. Thyroid cancer disease-related information (including terminology, stage, prognosis, and etiologic factors)
Banach et al. reported that 63% of thyroid cancer survivors reported that they had not received clear information on their disease and its treatment at the time of diagnosis (14). Furthermore, Husson et al. (15) reported that many thyroid cancer survivors indicated that they received little or no information about various aspects of their disease (27–86%), and some of the specific unmet needs included general information about thyroid cancer and thyroid function (unmet in 18%), as well as an explanation for the cause of their thyroid cancer (unmet in 11%) (15). Morley et al. reported that 74.0% of thyroid cancer survivors recalled receiving general information about thyroid cancer and 37.1% received information on thyroid terminology (17). Roberts et al. (18) reported that on a scale of 1–5 (where 5 is the best possible score), the mean scores and SD for receiving adequate information related to thyroid cancer in general, included: survival rates, 4.02 (SD = 1.18); cause of thyroid cancer, 2.70 (SD = 1.20); medical terminology, 3.15 (SD = 1.23); and the stage of thyroid cancer, 3.00 (SD = 1.31). Sawka et al. (19) reported that 44% of thyroid cancer survivors indicated an unmet information need relating to family members' risk of malignancy. In advising on ways to improve care, Banach et al. indicated that 45% of thyroid cancer survivors recommended that more information about the disease be provided to patients (14).
Theme 2. Information on thyroid cancer treatment (including treatment decision making)
Husson et al. (15) reported that 21–90% of thyroid cancer survivors received little or no information on various aspects of thyroid cancer treatment. Morley et al. (17) reported that 55.2% of thyroid cancer survivors recalled receiving information and support about treatment decisions. However, Morley et al. reported that the majority (84.2%) of patients recalled receiving information and support relating to thyroidectomy (17). Aschebrook-Kilfoy et al. reported that 26.3% of thyroid cancer survivors perceived that they had received inadequate communication about risks of thyroid cancer surgery from their healthcare providers (64). Furthermore, Morley et al. reported that 74.0% of survivors recalled receiving information and support on radioactive iodine therapy as well as 68.0% on “isolation” relating to radioactive iodine use (17). Aschebrook-Kilfoy et al. also reported that 28.8% of respondents indicated that they felt that the risks of radioactive iodine treatment were not adequately explained by their physicians (64). Kim et al. (16) reported that in a population of thyroid cancer patients undergoing outpatient low-dose radioactive iodine treatment, 45% of participants indicated that access to information sources about radiation safety was fairly or very difficult, and 49% of participants perceived that their awareness on radiation safety was not satisfactory. Also with potential relevance to radioactive iodine treatment, Morley et al. reported only 7.0% of respondents recalled receiving information and support relating to “fertility preserving options,” and 2.8% reported receiving “resources for fertility preservation” (17). Roberts et al. (18) reported that on a scale of 1–5 (where 5 is the best), the mean scores and SDs for receiving adequate information on thyroid cancer treatment or treatment decision making included: what to expect during surgery, 3.78 (SD = 1.15); how much pain to expect after treatment, 3.11 (SD = 1.32); how to prepare for surgery or radiation, 3.80 (SD = 1.05); and what to expect during “isolation,” 3.86 (SD = 1.09). Sawka et al. (19) reported that 63% of low-risk thyroid cancer survivors indicated an unmet need related to information on new treatments. Banach et al. reported that 34% of thyroid cancer survivors recommended that more information about the treatment options be provided to improve care (14).
Theme 3. Information on diagnostic tests (including imaging studies)
Husson et al. (15) reported that 20–27% of thyroid cancer survivors received little or no information on various issues regarding thyroid cancer-related diagnostic tests. Roberts et al. (18) reported that on a scale of 1–5, the mean score for receiving adequate information on diagnostic tests was as follows: what tests are given and why, 3.98 (SD = 0.95); frequency and rationale for “body scans,” 3.35 (SD = 1.31); and possible negative consequences of “body scans,” 2.58 (SD = 1.32). Banach et al. reported that about a quarter (24%) of respondents recommended that quicker patient access to test results was needed to improve care (14).
Theme 4. Information on aftercare (including clinical/personal monitoring for recurrence, long-term physical effects of the disease or its treatment, chronic thyroid hormone treatment, and rehabilitation)
Husson et al. (15) reported that 86–91% of thyroid cancer survivors received little or no information on aftercare, and some of the specific unmet needs included information on long-term effects of treatment and medication use (unmet in 67%), as well as general information on aftercare and rehabilitation options (unmet in 19%). Morley et al. reported that the following percentages of individuals reported receiving information and support on various issues relating to aftercare: recurrence (40.9%), thyroid hormone replacement (72.5%), possible long-term effects of treatment (25.4%), symptoms to watch for (37.7%), physician-based disease surveillance (38.2%), and managing treatment health effects (22.9%). Roberts et al. (18) reported that on a scale of 1–5 (where 5 is the best possible score), the mean scores and SDs for statements on receiving adequate information related to aftercare included the following: how to take medications properly, 3.97 (SD = 0.93); doctors monitoring for recurrence, 3.60 (SD = 1.24); how surgery affects appearance, 3.35 (SD = 1.14); duration side effects after surgery, 3.31 (SD = 1.18); problems related to calcium deficiency, 3.00 (SD = 1.40); symptoms requiring medical attention, 2.93 (SD = 1.31); treatment side effects, 2.79 (SD = 1.31); how to manage side effects, 2.75 (SD = 1.22); symptoms of possible recurrence, 2.67 (SD = 1.36); and possible impact of lifestyle factors on recurrence, 2.37 (SD = 1.10). Sawka et al. (19) reported that the following percentages of a sample of low-risk thyroid cancer survivors indicated an unmet information need related to various aspects of aftercare: possible long-term side effects of treatment, unmet in 63%; how to check for signs that cancer has returned, unmet in 47%; physical fitness/exercise, unmet in 23%; nutrition/diet, unmet in 35%; and having children in the future, unmet in 11% (although 51% indicated that this question was not applicable to them).
Theme 5. Information and support for psychosocial issues (including practical and financial matters and support services)
Banach et al. reported that 84% of thyroid cancer survivors indicated that they did not receive information on patient support organizations at the time of their diagnosis (14). Furthermore, Banach et al. reported that 93% of thyroid cancer survivors reported not receiving support from a psychologist or counselor and 77% did not receive support from a nurse or other support person at the time of diagnosis (14). Husson et al. also reported that the majority of thyroid cancer survivors received little or no information on the following issues: psychological assistance (92%), additional help (89%), and the expected impact of their thyroid cancer diagnosis/treatment on their social life (80%) (15). Similarly, Morley et al. reported that only about one in every five (20.9%) of thyroid cancer survivors perceived that they had received care and information about emotional and psychological concerns (17). Morley et al. indicated that the percentage of individuals reported receiving specific information and support related to psychosocial issues was as follows: managing financial aspects related to the disease or its treatment (6.3%), health insurance benefit counseling (7.0%), employment issues (12.0%), educational issues (3.9%), managing medical expenses (6.6%), bankruptcy (1.2%), support groups (27.9%), opportunities to meet other survivors (18.8%), counseling to manage psychological distress (12.3%), coping with fear of recurrence (9.2%), obtaining support from family/friends (32.4%), support during “isolation” for radioactive iodine treatment (20.0%), and coping strategies (10.4%). Aschebrook-Kilfoy et al. reported that 33.8% of thyroid cancer survivors perceived a lack of support from their physicians, and 23.1% perceived a lack of support from family members (64). Roberts et al. (18) reported that on a scale of 1–5 (where 5 is the best), the mean scores and SDs for statements related to psychosocial information needs included: expenses covered by insurance, 3.23 (SD = 1.20), other people's experiences with thyroid cancer, 3.02 (SD = 1.31), and where to get the most up-to-date information related to various thyroid cancer diagnostic/medical issues, 2.75 (SD = 1.19). Roberts et al. (18) also reported that on a scale of 1–5 (where 5 is the best), the mean scores and SDs for statements inquiring about receiving adequate support to deal with the following issues: fears about side effects, 3.20 (SD = 1.25); emotions at the time of diagnosis, 3.07 (SD = 1.24); getting support from family, 3.03 (SD = 1.17); anxiety about the future, 2.92 (SD = 1.32); uncertainty about the future, 2.90 (SD = 1.35); medical bills and statements, 2.88 (SD = 1.22); fears about the cancer coming back, 2.85 (SD = 1.22); the impact of cancer on the family, 2.79 (SD = 1.14); and understanding “why me?,” 2.72 (SD = 1.22). Sawka et al. (19) reported that the following percentages of thyroid cancer survivors indicated an unmet information need related to psychosocial issues: managing concern about cancer recurrence, unmet in 35%; managing concern about a second primary malignancy, unmet in 40%; financial support for medical care, unmet in 26%; how to discuss one's cancer experience with family and friends, unmet in 14%; and meeting other adolescents or young adult survivors, unmet in 14%. In suggesting potential improvements in care, Banach et al. indicated that the following percentages of thyroid cancer survivors recommended that the following be provided: 43% psychological support, 42% introduction to patient support groups, and 27% introduction to a fellow patient (individual peer support) (14).
Theme 6. Information on co-ordination of care (including patient involvement)
Husson et al. reported that 87% of thyroid cancer survivors received little or no information about different care locations (15). Morley et al. reported that less than half (44.9%) of survivors indicated that they had received information and support about communicating with their medical team and about a quarter (27.8%) had received information and support about accessing their medical record (17). Roberts et al. (18) reported that on a scale of 1 to 5 (where 5 is the best), the mean score for receiving adequate information on where to get practical information related to medical care was 3.27 (SD 1.31). Roberts et al. also indicated that the mean score for adequate support to manage access to medical records was 3.21 (SD 1.25). In advising on how to improve care, Banach et al. reported that 17% of thyroid cancer survivors recommended that access to a specialist or oncology nurse be provided and 16% indicated that easier access to cancer care teams was needed (14).
Theme 7. Information on complementary and alternative medicine
Morley et al. reported that only 5.3% of thyroid cancer survivors had received information and support on complementary and alternative medicine (17). Roberts et al. (18) reported that the mean score for receiving adequate support to get access to non-traditional (alternative, complementary) treatments was 2.40 (SD = 1.09) (on a scale of 1–5, where 5 is the most support). Furthermore, Sawka et al. reported that 68% of low-risk thyroid cancer survivors indicated an unmet information need on complementary and alternative treatments (19). Three of the studies in this review did not examine thyroid cancer survivors' information needs related to complementary and alternative medicine (14 –16).
Discussion
This systematic review found that unmet information needs in thyroid cancer survivors were highly variable relating to the disease, diagnostic tests (including imaging studies), treatments, and co-ordination of medical care. However, across multiple studies, there appeared to be relatively high prevalence rates of unmet information needs related to aftercare (especially long-term effects of the disease or its treatment and its management) and psychosocial concerns (including practical and financial matters). The results of this review also suggest that thyroid cancer survivors perceived that they were offered relatively little psychosocial support for concerns such as including in management of psychological/emotional issues, fear of recurrence, fear of side effects, of financial matters/employment, and impact on the family. Limited information was also provided to patients on complementary and alternative therapies.
In order to address some of the information needs of patients in a standardized manner, national thyroid organizations such as the American Thyroid Association (ATA) (65) and British Thyroid Association (BTA) (66) have made some patient information freely available online. The ATA online brochure on thyroid cancer reviews topics including the disease, its causes, how it is diagnosed, subtypes, treatments, prognosis, and disease surveillance (65). Furthermore, the BTA Clinical Practice Guidelines on Management of Thyroid Cancer include patient-directed information on a variety of thyroid cancer care–related topics, as well as contact information for patient support groups (66). The patient-directed information in the BTA guideline was developed in collaboration with patient representatives, and reported in a published appendix as part of the guideline (66). The topics included in the BTA patient leaflets include: general information on the thyroid and thyroid cancer, thyroid nodule investigations, thyroid surgery, radioactive iodine (ablation and therapy), medullary thyroid cancer, and advanced or higher-risk differentiated thyroid cancer (66). Patient support groups such as Thyroid Cancer Canada (67), ThyCa (68), the Butterfly Thyroid Cancer Trust (69), and the Light of Life Foundation (70) also provide some information online as well as access to patient support. There are also numerous other patient support groups providing very helpful information and psychosocial support resources in a variety of formats and languages throughout the world. Yet, in spite of the important work of such established organizations, this review suggests that some patients may not be receiving information about these resources or that additional resources may need to be developed. It is also important to acknowledge that information and support needs may be variable among individual patients, which may explain some of the variability of outcomes observed in this review. Furthermore, personalization of provision of information and support can be challenging in practice.
A possible barrier to access to psychosocial care may be the perception among some healthcare professionals that thyroid cancer is a “good cancer” and under-recognition of related psychosocial distress in survivors (21). In a qualitative study of Canadian thyroid cancer survivors, Easley et al. reported that survivors felt that they were perceived by healthcare professionals as not needing support, and they also felt unworthy of accessing available support programs (21). Yet, these survivors perceived their diagnosis and treatment as life-altering, and affirmed the presence of physical and emotional impacts (21). In another qualitative study, it was reported that thyroid cancer survivors perceived the diagnosis to be life-changing, but some felt dismissed by their healthcare providers as not having a “serious disease” (32). Furthermore, thyroid cancer survivors indicated that a “good cancer” message was generally not reassuring (32). Moreover, survivors experienced fear of recurrence and feelings of uncertainty about their future (32). Some possible barriers to provision of psychosocial support to thyroid cancer survivors is that some healthcare professionals treating thyroid cancer survivors may not feel completely confident exploring such issues, lack the time needed to address them within the constraints of a busy clinical practice, or lack local resources for appropriate referral. It is critically important that thyroid cancer survivors, just as other cancer survivors, are screened for emotional distress, and that adequate psychosocial supports are made available to individuals who need them. More research is needed on how to optimize psychosocial support and related health outcomes in thyroid cancer survivors. In order for such clinical and research targets to be fulfilled, it is important for healthcare providers, health policy makers, and research funding bodies ultimately to reject the notion of a “good cancer” and to take important strides to address the unmet information and psychosocial support needs of thyroid cancer survivors.
A preliminary, unexpected finding observed in some of the studies in this review was the identification of unmet patient information needs relating to the use of complementary and alternative medicine by thyroid cancer survivors. Complementary and alternative medicine is defined by the National Cancer Institute's Office of Cancer Complementary and Alternative Medicine (OCCAM) as “any medical system, practice, or product that is not thought of as standard care” (71), where standard care may be inferred to refer to Western mainstream medicine standard of care. Furthermore, OCCAM differentiates complementary medicine, which is used in “along with” standard care, from alternative medicine, which is used “in place of” standard care (71). Rosen et al. reported that in a survey of 1327 thyroid cancer survivors, 74% of respondents utilized complementary or alternative medicine (72). These data are not dissimilar from the American general oncology literature, where about two-thirds (66.5%) of survivors report using such treatment (73). It appears that many thyroid cancer survivors, like other oncology populations, express interest in complementary and alternative medicines, but they may lack sufficient information to make an informed choice about their utilization. An important challenge facing clinicians in counseling patients in this regard is insufficient high-quality evidence in this area in the context of thyroid cancer care.
The strengths of this systematic review include the execution of an electronic database search for citations by a library information specialist; duplicate independent review of all citations and full-text papers, and duplicate data abstraction; and critical appraisal of included studies. However, the levels of agreement between reviewers on inclusion of studies were limited, given the variable levels of clinical training of reviewers and some challenges in distinguishing studies describing patient distress outcomes without any quantification of the level to which associated needs were met/unmet (which were not eligible for inclusion) from those reporting on unmet psychosocial support needs. Another limitation is that only English language studies were included due to a lack of sufficient resources for translation. In addition, some of the primary studies may have overlapped study populations if any of the respondents participated in more than one survey study (e.g., for online surveys without access restrictions). Another weakness of this study is that specific personalized information and psychosocial support needs according to important variables such as clinico-histopathologic subgroup, life stage, or disease status in response to treatment were not identified. Clinically, it is clear that thyroid cancer may manifest as a wide spectrum of presentations ranging from indolent (micro-) papillary thyroid cancer to highly aggressive anaplastic cancer, and that it may be diagnosed at any life stage (spanning from childhood to elder years) and that the psychosocial impact may vary in part depending on these variables. Furthermore, the disease treatment response and any side effects related to the disease or its treatment and potential interaction with pre-existing comorbidities may impact the well-being and needs of thyroid cancer patients. Singer et al. have previously reported that thyroid cancer patients in a German inpatient rehabilitation unit experienced more physical and psychological symptoms and worse functioning than the general population do, with the most frequent complaints including problems with fatigue, sleep, and impaired emotional and role functioning (74). Singer et al. reported that many aspects of quality of life were found to be unrelated to disease stage, with the exception of physical function and global health status (74). Such data suggest that it may not be appropriate to assume that distress in thyroid cancer patients is only restricted to higher-risk patients.
In conclusion, there are substantial unmet medical information and psychosocial support needs in thyroid cancer survivors, including those in aftercare. More attention is needed to improve knowledge translation and psychosocial support to this frequently overlooked population of cancer survivors.
Footnotes
Acknowledgments
Financial support for this study was provided in part from a University Health Network Foundation—Thyroid Cancer Research Fund. A.M.S. was supported by a University of Toronto Department of Medicine Clinician Scientist Merit Award. The assistance of the following individuals is also acknowledged in this study: Asima Naeem (research associate, who assisted with abstraction of some of data) and Coreen Marino (administrative assistant, who assisted with retrieval of papers for review). A.M.S. is an unpaid (volunteer) member of the Medical Advisory Panel for the Thyroid Cancer Alliance patient support organization. The Thyroid Cancer Alliance had no role in the design, execution, or reporting of this study.
Author Disclosure Statement
No financial disclosures.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.