
Abstract
Background:
The risks of thyroid dysfunction after iodinated contrast media exposure in patients with euthyroid nodular goiter are largely unknown.
Methods:
This observational, retrospective cohort study included a random selection of one million people in Taiwan. All patients with iodinated contrast media exposure during this study period were selected. Patients with euthyroid nodular goiter were identified as cases, while patients without thyroid nodule were selected as controls. We followed these patients until the first event of thyroid dysfunction including hyperthyroidism or hypothyroidism after iodinated contrast media exposure.
Results:
A total of 334 cases and 2672 matched controls were selected in this study. The mean age of cases and controls were 58.6 and 58.4 years old, and mean follow-up durations were 2.1 and 2 years respectively. After adjustment, patients with euthyroid nodular goiter had a higher risk of thyroid dysfunction (hazard ratio 5.43, [confidence interval (CI) 3.01–9.80]) compared with controls after iodinated contrast media exposure. In the subgroup analysis, the risks of hyperthyroidism and hypothyroidism in cases compared with controls were 5.77 [CI 2.64–12.62] and 4.95 [CI 2.15–11.40] respectively. Half of the euthyroid nodular goiter cases developed thyroid dysfunction within one year after iodinated contrast media exposure. Interestingly, all thyroid-related comorbidities and drug prescriptions did not increase the risk of thyroid dysfunction.
Conclusions:
Presence of euthyroid nodular goiter was associated with higher risk of thyroid dysfunction including hyperthyroidism and hypothyroidism after iodinated contrast media exposure.
Introduction
I
The risk of iodine deficiency decreased following the implementation of a mandatory salt iodization policy in numerous countries worldwide. However, the risk of excess iodine intake is increasing because of dietary changes and the use of medications that contain a high amount of iodine. Potential iodine excess may result from taking common medications, such as amiodarone, as well as iodinated contrast media (ICM), which is used in radiological medical procedures. In contrast to amiodarone, which is widely known to have a potential effect on thyroid function, the potential impact of ICM is largely ignored. A single dose of ICM can contain up to 13,500 mcg of free iodine and 15–60 g of bound iodine, which is several thousand times the recommended daily iodine requirement (4). Although the frequency of thyroid dysfunction after ICM exposure was found to be low (5), it may still be of relevance because the frequency of radiological examinations that require ICM has increased several fold in the last two decades (6–7).
Epidemiologic studies showed that the prevalence of thyroid nodule is surprisingly high in the clinically normal thyroid gland, with a rate of 50% according to autopsy data (8). Fortunately, most of these nonpalpable nodules are benign and clinically insignificant. Nevertheless, several studies demonstrated that patients with nodular goiter have a higher risk of thyroid dysfunction after excess iodine exposure (9 –11). However, this phenomenon was only examined in studies conducted several decades ago with a relatively small sample size and without a controlled study design. Therefore, we conducted a study using a nationwide population-based database to evaluate whether patients with nodular goiter have a higher risk of thyroid dysfunction after excess iodine exposure by ICM.
Material and Methods
Setting
This observational, retrospective cohort study was conducted using the Longitudinal Health Insurance database 2005 dataset, which was obtained from Taiwan's National Health Insurance (NHI) program. Taiwan's NHI program is a compulsory insurance system that is regulated by Taiwan's government, providing coverage for almost 99% of Taiwan's entire population. This dataset comprises detailed information pertaining to patients' disease diagnosis, drug prescriptions, medical expenses, hospital admission, and discharge diagnosis. A detailed description of patients' recruitment and sampling procedure is available on the National Health Insurance Research Database (NHIRD) website (12). All patients' data in the NHIRD are encrypted and scrambled before release to the public for academic research. Data were extracted and analyzed by one independent reviewer. This study was reviewed and approved by the Institutional Review Board of Chung Shan Medical University Hospital, Taichung, Taiwan.
Participants and protocol
Patients were enrolled by random selection from one million patients in 2005, which was representative of 4% of the total population of 23 million people in Taiwan. Patients were tracked from 1 January 2004 to 31 December 2010, with a total follow-up duration of 6 years. All patients with ICM exposure during this study period were selected, including patients who received ICM due to the following medical procedures: computed tomography, cholangiography, intravenous pyelography, and angiography. We further selected patients with euthyroid nodular goiter as cases, while patients without thyroid nodule were classified as controls. Patients with the following criteria were excluded: (1) no ICM exposure during the entire study period (n = 916,240); (2) patients with ICM exposure in the previous year of observation (n = 6683); (3) patients with past history of hyperthyroidism or hypothyroidism, patients with thyroid operation, patients with levothyroxine or anti-thyroid drugs prescription (n = 4,668); and (4) patients with missing data (n = 88).
Disease comorbidities that potentially increase the risk of thyroid dysfunction such as diabetes mellitus, rheumatoid arthritis, bipolar disorder, chronic kidney disease, anemia, and Sjögren's syndrome were identified, as well as drug prescriptions such as amiodarone, beta-blocker, carbamazepine, dexamethasone, interferon, interleukin 6, lithium, phenobarbital, phenytoin, propylthiouracil, and rifampicin. Eight matched controls with propensity score matching of baseline characteristics, such as age, sex, urbanization status, disease comorbidities, use of drugs, and index date were selected for every euthyroid nodular goiter case to minimize selection bias, thereby allowing a more accurate evaluation of the thyroid dysfunction after ICM exposure. A detailed flow diagram of this study design is shown in Figure 1.
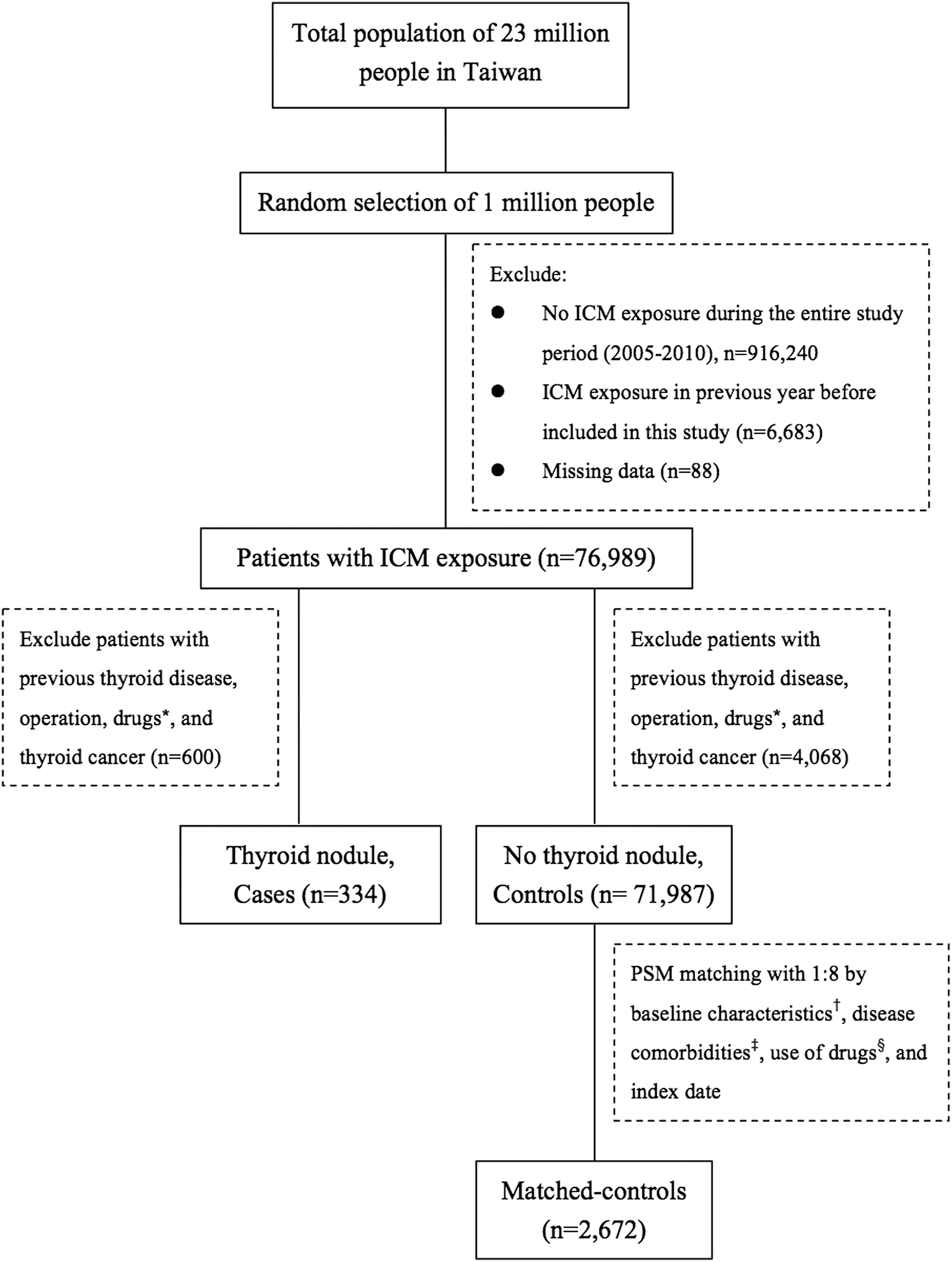
Flow diagram of assessment. *Drugs, including levothyroxine or anti-thyroid drugs. †Baseline characteristics, including age, sex, and urbanizations status. ‡Disease comorbidities, including diabetes mellitus, rheumatoid arthritis, bipolar disorder, chronic kidney disease, anemia and Sjösgren's syndrome. §Use of drugs: amiodarone, beta blocker, carbamazepine, dexamethasone, interferon, interleukin 6, lithium, phenobarbital, phenytoin, prophylthiouracil, or rifampicin. ICM, iodinated contrast media; PSM, propensity score matching.
Variables
The date of ICM exposure was set as the index date and these patients were followed until the first event of thyroid dysfunction, including hyperthyroidism or hypothyroidism, which served as the event date, while disenrollment, mortality, or 31 December 2010 were designated as the end date. A number of comorbidities and covariates were identified by documented evidence of a diagnosis at the time of entry. “Euthyroid nodular goiter case” was defined as patients with International Classification of Diseases, 9th Revision, Clinical Modification (ICD9-CM) code of 241 without evidence of thyroid dysfunction or thyroid cancer (ICD9-CM code of 242–246, and 193), operation, and levothyroxine or antithyroid drugs prescription. “Control” was defined as patients without any thyroid disease (ICD9-CM code of 240–246, 193, operation history, and levothyroxine or anti-thyroid drug prescription) prior to ICM exposure. “Hyperthyroidism” was defined as an inpatient hospitalization with ICD9-CM code of 242.x, or at least two outpatient physician visits with ICD9-CM code of 242.x, or one outpatient physician visit with ICD9-CM code of 242.x plus antithyroid drug prescription. “Hypothyroidism” was defined as an inpatient hospitalization with ICD9-CM code of 244.x, or at least two outpatient visits with ICD9-CM code of 244.x, or one outpatient visit plus thyroid hormone drug prescription. Patients who fulfilled the criteria of either hyperthyroidism or hypothyroidism were considered to have thyroid dysfunction. A detailed description of the definitions of variables is provided in Supplementary Table S1 (Supplementary Data are available online at
Statistical analysis
Descriptive analysis was used to compare variables between euthyroid nodule cases and non-thyroid disease controls. Unpaired Student's t-test and chi-square test were used to compare the parametric continuous and categorical data, respectively, between the two groups. Hazard ratio (HR) and Cox proportional hazards model with 95% confidence interval [CI] were used to analyze the data and to determine the risk of thyroid dysfunction. A two-sided p-value 0.05 was considered to be statistically significant. Cumulative hazard curves of the time to the first event of thyroid dysfunction were calculated using the Kaplan-Meier method. All statistical analyses were performed using the SPSS Statistical Package, version 18 (IBM Corp.).
Results
Study patients
A total of 76,989 patients with ICM exposure were enrolled from 1 January 2005 through 31 December 2010. Of these patients, 334 patients with euthyroid nodular goiter were selected as cases, and 71,987 patients without any thyroid disease were identified as controls. Meanwhile, a total of 2672 matched controls were selected from 71,987 patients in this study. After adjusting for all variables, the characteristics of the patients at baseline were well balanced between cases and controls. Mean follow-up durations of cases and controls were 2.1 and 2 years respectively. The mean ages of cases and controls were 58.6 and 58.4 years, respectively (Table 1).
Use of drugs: amiodarone, beta-blocker, carbamazepine, dexamethasone, interferon, interleukin 6, lithium, phenobarbital, phenytoin, prophylthiouracil, or rifampicin.
p < 0.05, ** p < 0.01.
Outcomes
A total of 19 euthyroid nodular goiter cases (cumulative risk, 5.7%) developed thyroid dysfunction, compared with 28 non-thyroid disease controls (cumulative risk 1.1%) after ICM exposure. The number needed to harm was one for every 22 people. The mean durations to thyroid dysfunction for euthyroid nodular goiter cases and non-thyroid disease controls were 1.3 and 1.4 years respectively. After adjusting for all variables, patients with euthyroid nodular goiter cases had a higher risk of thyroid dysfunction (HR 5.43 [CI 3.01–9.80]) compared with non-thyroid disease controls after ICM exposure. Women and patients 40–80 years old also had a higher risk of thyroid dysfunction, but this was not statistically significant. Interestingly, none of the thyroid-related comorbidities or drug prescriptions increased the risk of thyroid dysfunction (Table 2).
Adjusted hazard ratio (HR): adjusted for all variables.
Use of drugs: amiodarone, beta-blocker, carbamazepine, dexamethasone, interferon, interleukin 6, lithium, phenobarbital, phenytoin, prophylthiouracil, or rifampicin.
p < 0.05, ** p < 0.01.
CI, 95% confidence interval.
Table 3 shows various model adjustments to evaluate the risk of thyroid dysfunction after ICM exposure. Model 1 was adjusted for baseline characteristics such as age, sex, and urbanization status. Model 2 was adjusted for model 1 plus disease comorbidities, including diabetes mellitus, rheumatoid arthritis, bipolar disorder, chronic kidney disease, anemia, and Sjögren's syndrome. Model 3 was adjusted for model 2 plus drug prescription. The risk of thyroid dysfunction was increased in euthyroid nodular goiter cases after ICM exposure compared with non-thyroid disease controls, even after various adjustments. The adjusted hazard ratios of hyperthyroidism and hypothyroidism in euthyroid nodular goiter cases compared with non-thyroid disease controls were 5.77 [CI 2.64–12.62], and 4.95 [CI 2.15–11.40] respectively. Mean times to overall thyroid dysfunction, hyperthyroidism, and hypothyroidism events between euthyroid nodule and controls were 1.3 years versus 1.4 years; 0.8 years versus 1 year; and 1.7 years versus 1.8 years, respectively. Kaplan-Meier curves of cases and control after ICM exposure showed the increase in first event of thyroid dysfunction seemed to emerge after 6 months of ICM exposure, with continuous divergence over the 6-year follow-up period (Figure 2).
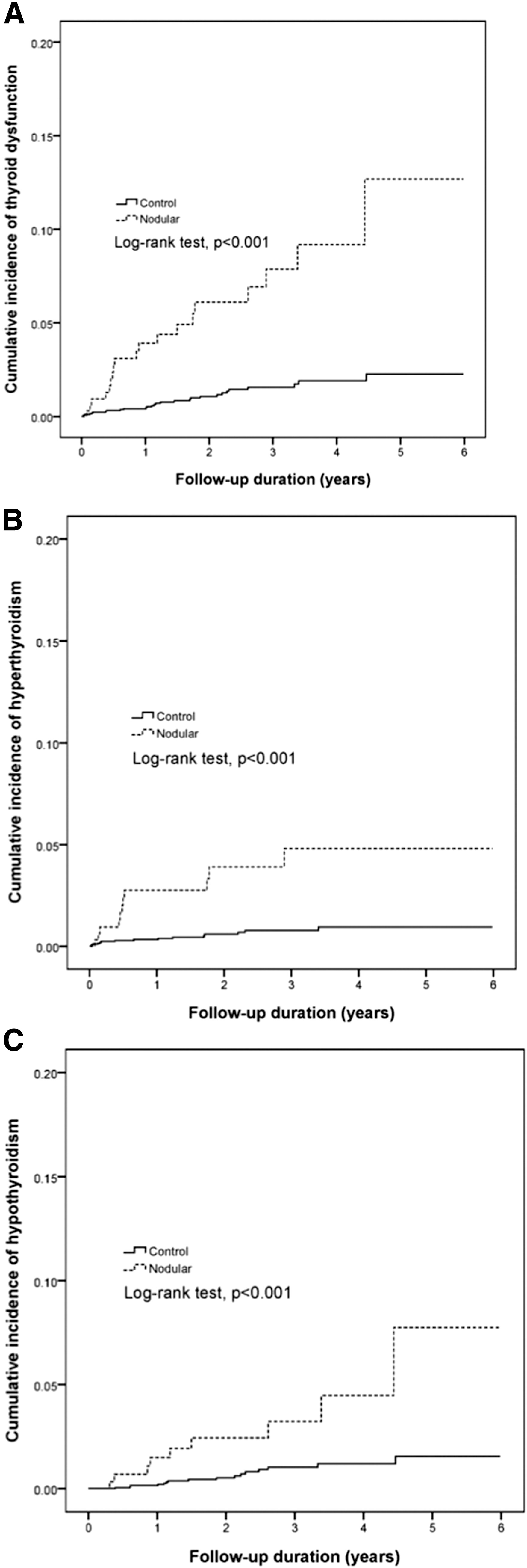
Kaplan-Meier analysis among euthyroid nodular goiter patients and controls after iodinated contrast media exposure; (
Model 1: adjusted for age, sex, and urbanization.
Model 2: model 1 + diabetes mellitus, rheumatoid arthritis, bipolar disorder, chronic kidney disease, anemia, and Sjogren's syndrome.
Model 3: model 2 + use of drugs.
p < 0.01.
Figure 3 shows the detailed times to thyroid dysfunction events between cases and controls after ICM exposure. In the first year, 58% of euthyroid nodular goiter cases developed thyroid dysfunction compared with 36% in the non-thyroid disease controls. In the first 6 months, half of these patients, including cases and controls, developed hyperthyroidism, whereas only about 20% of the patients developed hypothyroidism. Surprisingly, none of the cases or controls developed hypothyroidism in the first 3 months, and most of this population developed hypothyroidism after 1 year of ICM exposure.
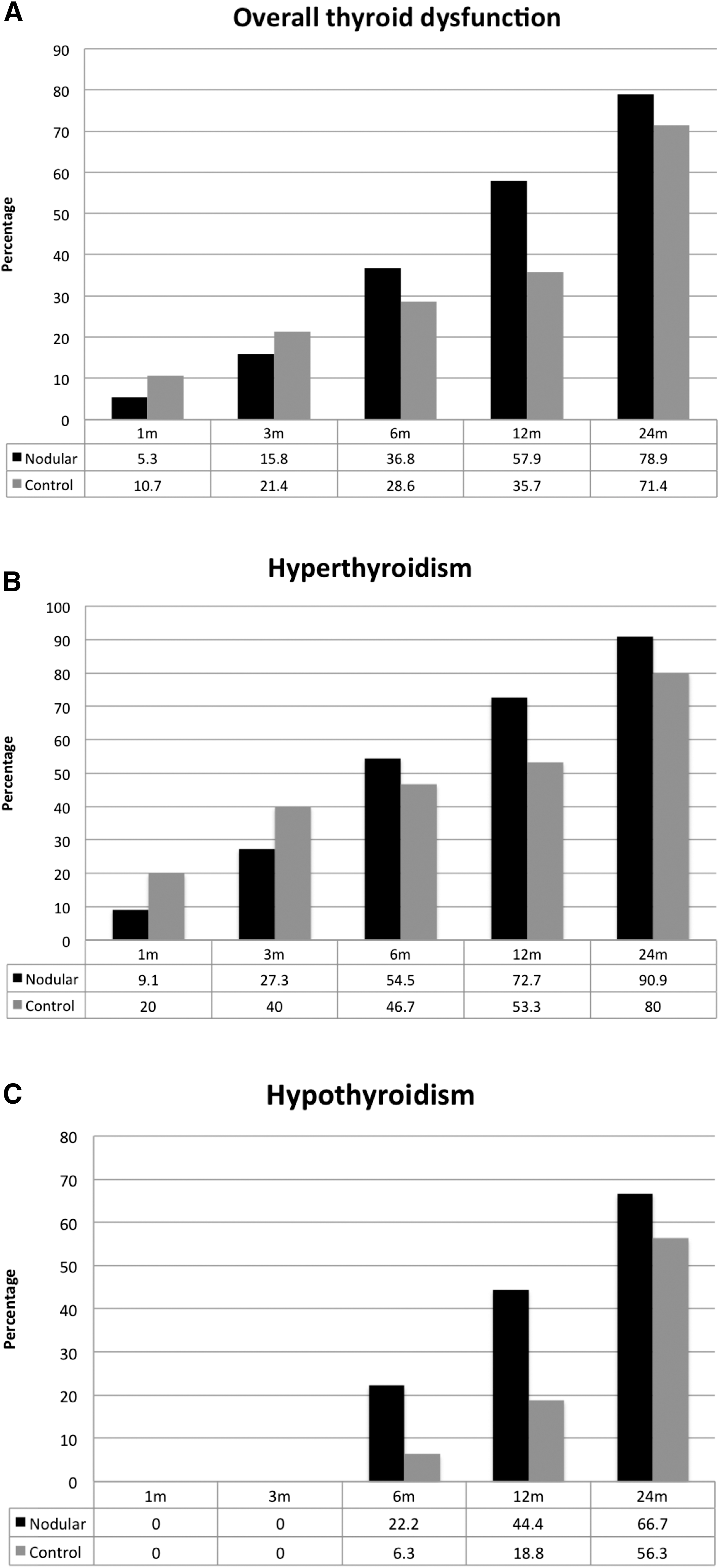
Time to thyroid dysfunction after ICM exposure: (
Most of the patients with euthyroid nodular goiter developed thyroid dysfunction following the first exposure to ICM, whereas patients without thyroid disease developed thyroid dysfunction after three or more exposures to ICM. After the first exposure to ICM, 15 of 212 patients with euthyroid nodular goiter developed thyroid dysfunction (cumulative risk of 7.1%), compared with 17 of the 1502 non-thyroid disease controls (cumulative risk of 1.1%). No linear correlation was found between ICM exposure frequency and thyroid dysfunction in this study, as shown in Supplementary Table S2.
Discussion
This study found that patients with euthyroid nodular goiter had a higher risk of thyroid dysfunction (HR 5.43 [CI 3.01–9.80]), including hyperthyroidism (HR 5.77 [CI 2.64–12.62]) and hypothyroidism (HR 4.95 [CI 2.15–11.40]) after ICM exposure compared with patients without any thyroid disease. To the best of our knowledge, this is the first study in an Asian country to evaluate the effect of thyroid dysfunction in euthyroid nodule patients after ICM exposure, and to date is the largest such study with a control group. Thyroid dysfunction risk mostly occurred after the first exposure to ICM within 1 year, and there were no differences in disease comorbidities and drug prescription.
Iodine intake is a major environmental determinant of thyroid dysfunction after excess iodine intake. In iodine-deficient areas, hyperthyroidism commonly develops after excess iodine intake, an effect that is known as the Jod-Basedow phenomenon (13 –16). Although the general population in Taiwan is known to be iodine-sufficient with a median UIC of 100 mcg/L, older patients (more than 60 years) were classified as being mildly iodine deficient with a median UIC of 87 mcg/L (3). Interestingly, this study demonstrated that the risk of thyroid dysfunction was not increased in older patients (>60 years) after ICM exposure compared with younger patients (<60 years old).
The risk of hyperthyroidism was evaluated in iodine-sufficient areas after excess iodine intake (5), especially in patients with previous thyroid disease such as nodular goiter, and latent Graves' disease (9 –11). In Boston, Vagenakis et al. reported that 4 of 8 patients with euthyroid nodules who were administered high amounts of iodide (five drops of a saturated solution of potassium iodide) developed hyperthyroidism (9). Moreover, Rajatanavin et al. studied 3 patients with euthyroid multinodular goiter who received excess iodine exposure by radiocontrast media, betadine, and amiodarone. All of them developed hyperthyroidism within 1 year of observation (10). The current study was conducted in Taiwan, which is an iodine-sufficient area. We found that the thyroid dysfunction risk was increased almost five-fold after ICM exposure in euthyroid nodular goiter cases and the number needed to harm was one in every 22 patients compared with non-thyroid disease controls. In the subgroup analysis, we found that 72% of euthyroid nodular goiter cases developed hyperthyroidism within 1 year, while more than half of the euthyroid nodular goiter cases developed hypothyroidism after 1 year of ICM exposure.
The normal adaptation to the sudden increase of iodine excess has been explained by the Wolff-Chaikoff effect (17). A transient reduction of thyroid hormone synthesis was observed in rats within 24 hours after exposure to a high amount of iodine. Several inhibitory substances such as intrathyroidal iodolactones, iodoaldehydes, or iodolipids are generated, which result in reduced thyroid peroxidase activity. Decreased expression of the sodium-iodide symporter, and perhaps decreased intrathyroidal deiodinase activity, also contributes to decreased synthesis of thyroid hormones after iodine excess (18). The mechanism of iodine-induced hyperthyroidism involves impairment of the acute Wolff-Chaikoff effect due to rapid iodine excess and influx into the thyroid gland, which results in increased thyroid hormone synthesis. The resultant hyperthyroidism may be due to an autonomous nodule becoming hyperfunctioning after exposure to excess iodine.
An important finding in this study was that patients with euthyroid nodular goiter also had a higher risk of hypothyroidism after ICM exposure, a finding that has not been previously reported. The main difference between our study and a previous study (8–9) was the sample size and follow-up duration. The onset of hypothyroidism was observed after more than six months of exposure to ICM. The exact mechanism of the delayed effect of hypothyroidism after ICM exposure is complex and not clearly understood. A possible mechanism involves decreased expression of some thyroid hormone-related genes after ICM exposure.
In patients without any thyroid disease, excess iodine after ICM exposure will result in transient or permanent hyperthyroidism (19–20). The pharmacokinetics of all currently available ICM are similar. The half-life of ICM in patients with normal renal function is approximately 2 hours. Therefore, approximately 20 hours are needed for the entire administrated ICM to be totally excreted (21). The peak of UIC occurrs at 1.1 weeks, and the mean time to normalization is 5.2 weeks after ICM administration (22). When compared with patients without ICM exposure, our previous study demonstrated that the risk of thyroid dysfunction (HR 1.46 [CI 1.29–1.66]), including hyperthyroidism (HR 1.22 [CI 1.04–1.44]) and hypothyroidism (HR 2.00 [CI 1.65–2.44]), was increased significantly after ICM exposure (5).
This study has several strengths, most notably its large sample size, long-term follow-up, and strict inclusion criteria. Our data are representative of a nationwide population based in Taiwan. It is also the first such study in an Asian country that also includes patients without thyroid disease who served as controls. However, there are also some limitations in this study. First, it was not possible to collect data on the exact dose and detailed ICM osmolarity in every ICM-related examination. Second, because the NHIRD is primarily maintained for reimbursement, there were no data regarding patients' personal information, such as smoking history, family history, body mass index, and laboratory data such as thyrotropin, free thyroxine, thyroid antibodies, and UIC, which may potentially mask subclinical disease. Third, there was no detailed information regarding the size and number of thyroid nodules, which may potentially influence the risk of thyroid dysfunction. Finally, the retrospective study design itself may potentially have resulted in selection bias.
However, because the dataset used in the present study was derived from the whole population without a sampling procedure, potential selection bias related to sampling error was not a concern. Although thyroid dysfunction might have been misclassified, the likelihood of such an occurrence is low because miscategorized diagnoses influence reimbursement, which is not tolerated by hospitals and clinics. In fact, Taiwan's National Health Insurance program also conducts stringent monitoring of claims to avoid overdiagnosis and prevent financial irregularities.
Currently, there are no prophylactic recommendations or guidelines before ICM exposure in clinical practice in Taiwan and elsewhere. Clinicians in Taiwan do not regularly monitor thyroid function after ICM exposure. Thyroid function is only checked when the patient experiences typical thyroid disease symptoms and signs. Further prospective studies with control groups are urgently needed to evaluate the risk of thyroid dysfunction in patients with nodular goiter after ICM exposure. The use of radiological examination requiring ICM in clinical practice is rapidly increasing, and thus the corresponding risk of thyroid dysfunction can be expected to rise. Indeed, the risk of thyroid dysfunction in the present study was found to be high, and the prevalence of thyroid nodules itself was surprisingly high. Another important question regarding this issue that needs to be addressed is whether the size or number of thyroid nodules will increase the risk of thyroid dysfunction after ICM exposure.
Finally, this study demonstrates that in an iodine-sufficient area, patients with euthyroid nodular goiter have a higher risk of thyroid dysfunction after ICM exposure compared with patients without any thyroid disease. Treating physicians must be especially mindful of patients with thyroid nodules with respect to the elevated risk of thyroid dysfunction after ICM exposure. Although severe hyperthyroidism, which may lead to thyroid storm, rarely occurs in clinical practice (23), the consequences of thyroid dysfunction should not be underestimated. Clinical physicians should be aware of the complications of ICM and use it cautiously in clinical practice.
Footnotes
Acknowledgments
We thank Yu-Hsun Wang of Chung Shan Medical University Hospital for his support and contribution. CN Huang, JY Chiou, SC Lo, and E. Kornelius, designed the study; CN Huang, JY Chiou, E. Kornelius, YS Yang, SC Lo, CH Peng, and YR Lai acquired, analyzed, and interpreted the data; E. Kornelius wrote the manuscript; and CN Huang and JY Chiou reviewed and edited the manuscript. CN Huang drafted the manuscript. CN Huang is the guarantor of this work and takes responsibility for the integrity of the data and the accuracy of the data analysis. We verify that all authors had access to the data and a role in writing the manuscript.
The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, the Ministry of Health and Welfare, or the National Health Research Institutes.
Author Disclosure Statement
The authors have nothing to disclose.