
Abstract
Background:
Antithyroid drug (ATD) is a widely used treatment for Graves' disease (GD). However, its long-term efficiency remains unclear. This study investigated the long-term disease prognosis and predictive factors for relapse in ATD-treated GD patients.
Methods:
Newly diagnosed, ATD-treated GD patients with at least four years of follow-up were recruited (n = 187). Remission was defined as maintaining a euthyroid status for more than one year after ATD withdrawal.
Results:
During 11.1 years (range 4.0–23.7 years) of median follow-up, overall, 51.9% of the newly diagnosed ATD-treated GD patients achieved remission, 32.1% continued ATD treatment, and 13.4% underwent other ablation treatments. The 10-year remission rates were higher in the first (34.2%) and second (25.5%) ATD courses than in any of the other subsequent ATD courses, and decreased as ATD treatments were repeated. The 10-year relapse rate was the highest after the third ATD treatment (71.4%) compared with that after the first (60.5%) and second (58.3%) courses. Longer duration of ATD treatment (odds ratio [OR] = 1.4 [confidence interval (CI) 1.2–1.7], p < 0.001), higher number of relapses (OR = 4.7 [CI 2.3–9.8], p < 0.001), and moderate to severe Graves' ophthalmopathy (OR = 4.1 [CI 1.1–15.2], p = 0.032) were associated with persistent disease status.
Conclusions:
A second course of ATD can be considered for GD patients after the first relapse because the chance of remission and the relapse rate are similar to the one after the first ATD treatment course. For GD patients with more than two relapses, or with an ATD treatment duration of more than four to five years, low-dose maintenance of ATD or ablative treatment needs to be considered.
Introduction
A
There have been many efforts to find risk factors that predict the relapse after ATD withdrawal. Young age, smoking, male sex, family history, presence of goiter, Graves' ophthalmopathy, high titers of thyrotropin receptor antibodies at diagnosis or at the end of the treatment, or duration of ATD treatment have all been proposed as risk factors. However, the results are conflicting (10 –19). This inconsistency might be due to different ethnic backgrounds or treatment protocols. In addition, variable definitions of relapse or remission could be a major reason for the reported inconsistency. Most studies defined relapse and remission based on a relatively short follow-up duration of less than one to two years (11 –14).
This study investigated the long-term clinical outcomes of newly diagnosed GD patients with a follow-up period of more than four years. The cumulative rates of disease remission and relapse for each ATD treatment were compared, and the predictive factors for relapse after ATD treatment were evaluated.
Methods
Subjects
A retrospective review of electronic medical records was done, including newly diagnosed GD patients who visited Seoul National University Hospital between August 1993 and November 2001. The diagnosis of GD was based on clinical examination with laboratory data (suppressed thyrotropin [TSH] with high free thyroxine [fT4] or total triiodothyronine [TT3] levels) and increased thyroid uptake of 99m-Tc in the radionuclide scintigraphy. A total of 215 patients were screened. Twenty-three patients whose overall follow-up durations were less than four years, as well as five patients who received RAI or surgery after a short course of initial ATD treatment because of a large goiter (n = 3), severe liver function abnormality (n = 1), or severe urticaria (n = 1), were excluded. Finally, 187 patients were enrolled. The clinical status at the last visit to the clinic was used as the final outcome. This study was conducted according to the guidelines of the Declaration of Helsinki, and the research protocol was approved by the Institutional Review Board committee of Seoul National University Hospital (No. 1410-097-619).
Clinical parameters, age, sex, family history of autoimmune thyroid disease, goiter size, and the presence of Graves' ophthalmopathy were assessed. Laboratory parameters including serum TSH, fT4, TT3), and TSH-binding inhibitory immunoglobulin (TBII) were measured (20,21). Goiter size and the presence of Graves' ophthalmopathy were estimated by a single physician (B.Y.C.), as previously described (20 –22). Goiter size was categorized as being nonvisible (<20 g), visible (25 − 50 g), or large (≥50 g) (22). Graves' ophthalmopathy was defined according to the NOSPECS (no signs or symptoms; only signs; soft tissue; proptosis; extraocular muscle; cornea; and sight loss) classification and classified into three groups: absent, mild (NOSPECS grade 1 or 2), and moderate to severe (NOSPECS grade 3 − 6) (23). Serum TSH, fT4, and TT3 concentrations were measured by an immunometric assay (Abbott, North Chicago, IL). TBII activity was measured with the percentage inhibition of [125I] TSH binding using a radioreceptor assay kit (RSR Limited, Cardiff, United Kingdom).
Follow-up protocol and data collection
Patients were initially treated with 15–30 mg/day of methimazole for one month, 10–20 mg/day from the second month to the time of serum fT4 normalization, and 2.5–5 mg/day thereafter, as previously described (22). ATD was discontinued when (i) both the serum TSH and TBII values were normalized, or (ii) a euthyroid status was maintained for more than one year with low-dose maintenance ATD treatment (methimazole <5 mg/day), regardless of the TBII levels (22). For the patients who relapsed or who showed a fluctuating thyroid functional status during ATD treatment, ablative therapy such as RAI or surgery was recommended. For those who refused ablation, a second course of ATD treatment or more were performed. Low-dose ATD treatment was performed in patients who did not want to discontinue the ATDs after relapsing two or more times. The number of relapses, ATD treatment duration, and time from ATD discontinuation to relapse were retrieved from the medical records.
Definition of remission after ATD treatment or relapse after ATD discontinuation
Remission was defined as a euthyroid status with normal free T4, T3 and TSH maintained for more than one year after ATD withdrawal. For those who showed an abnormal thyroid function within 3 months after drug discontinuation, ATD was restarted, and the status was defined as persistent. Relapse was defined as a decrease in the TSH level with or without elevated free T4 in the course of remission. The TBII value was not considered in the definitions of remission, persistence, or relapse of disease.
Statistical analysis
The continuous variables are shown as either the mean ± standard deviation (SD) or the median and range. The categorical variables are described as numbers with percentages in parentheses. For comparison of continuous variables between two groups, an independent t-test or Mann–Whitney U-test was used. Analysis of variance with Tukey's post hoc analysis was used for the comparison of continuous variables between more than two groups. The chi-square test or Fisher's exact test was used for the comparison of categorical variables. Survival curves based on the time to relapse were plotted using Kaplan–Meier curves to determine the rates of relapse or remission during follow-up. Logistic regression analysis was used to estimate the influence of several parameters on the long-term prognosis of persistent GD. The level of statistical significance was defined as a p-value of <0.05. Statistical analyses were performed with the IBM SPSS Statistics for Windows v19.0 (IBM Corp., Armonk, NY).
Results
Clinical course of GD after ATD treatment
Among the 187 enrolled patients, 142 (75.9%) were women, and their mean age at diagnosis was 38.0 ± 13.9 years. Of these, 114 (61.0%) had goiter, 51 (27.3%) had Graves' ophthalmopathy, and two (1.0%) had other combined autoimmune diseases (Myasthenia graves and rheumatoid arthritis). There was no sight-threatening Graves' ophthalmopathy. The median follow-up duration was 11.1 years (range 4.0–23.7 years), and they received a median of two cycle (range 1–5 cycles) of ATD treatment. Initially, 93% of the patients received methimazole as their initial ATD, and nine patients changed to propylthiouracil because urticaria developed within three months after the initial treatment. There were no serious adverse events related to ATD. A total of 25 patients became pregnant during their follow-up; 14 were able to stay off ATDs during the pregnancy, and eight were treated with propylthiouracil while one received low-dose methimazole, and two required thyroxine during pregnancy. There were no serious long-term adverse events related with the ATD treatment, including neonatal congenital abnormalities.
Figure 1 shows the clinical course of the enrolled patients (n = 187). Individual patients are shown in Supplementary Figure S1 (Supplementary Data are available online at

Flow chart of the patients with Graves' disease who were followed up for at least four years. ATD, antithyroid drug; RAI, radioactive iodine therapy; OP, operation. *These patients were excluded because of the follow-up loss.
Sixty (32.1%) patients continued ATD treatment until their last visit: 41 patients were under active ATD treatment with fluctuating abnormal thyroid functions, and 19 patients were receiving low-dose maintenance of ATD treatment, ≤5 mg/day of methimazole with normal thyroid function. These 19 patients received low-dose maintenance therapy for a median of 4 years (range 3.0–5.9 years) with no further deterioration in thyroid function. They experienced a relapse median of once (range 1–2 times), and their cumulative ATD treatment duration was a median of 14.4 years (range 12.3–17.3 years) with no serious adverse events. Twenty-five (13.4%) patients underwent ablative therapy such as RAI treatment or surgery due to ATD refractoriness.
Cumulative relapse rate after ATD withdrawal
To evaluate the therapeutic efficacy of each course of ATD treatment, the cumulative rates of ATD discontinuation were analyzed for each course. After two years of ATD treatment, the usual recommended duration for ATD treatment (6), 45.5% and 42.9% of the patients discontinued ATD after the first and second courses of ATD treatment, respectively, while only 28.6% discontinued ATD after the third treatment course (Fig. 2A). Interestingly, the cumulative rates of ATD discontinuation continued to increase after the initial two-year treatment. At four years, 67.9%, 54.1%, and 51.4% of the patients discontinued ATD after the first, second, and third courses of treatment, respectively (Fig. 2A).
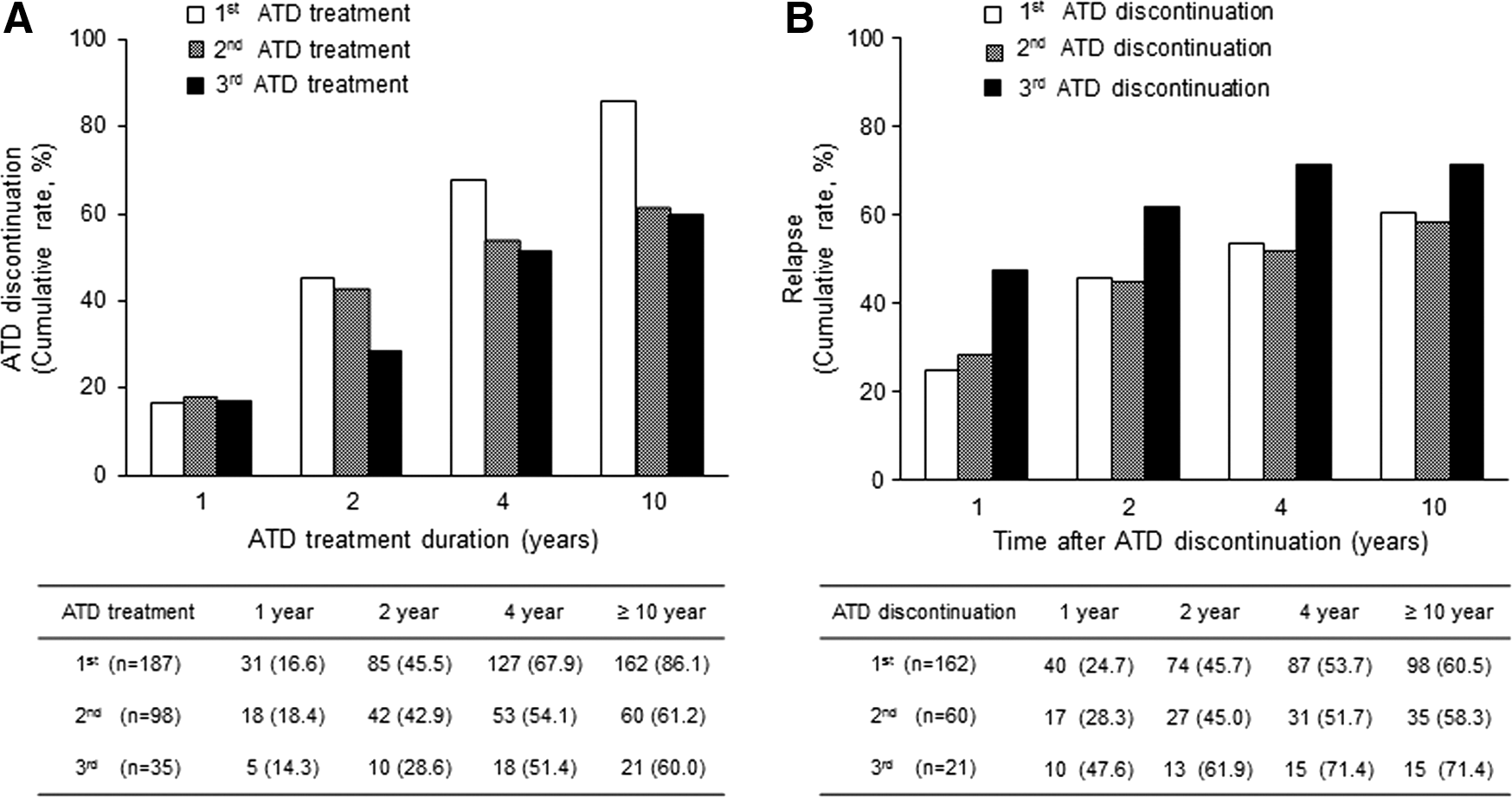
The cumulative rates of ATD discontinuation and relapses according to the each ATD treatment course. (
The final cumulative rate of relapse was 71.4% in the third course, much higher than 60.5% in the first course and 58.3% in the second course (Fig. 2B). The cumulative rates of relapse increased with time, and >90% of relapses occurred within four years after ATD discontinuation. Especially, in the third ATD treatment, there was no further relapse after four years after ATD discontinuation (Fig. 2B).
Comparison of clinical characteristics between the remission group and the persistent group
To analyze clinical and treatment-related factors predicting the long-term prognosis of ATD therapy, the clinical characteristics were compared between the remission and persistent groups.
The age at diagnosis and initial goiter size were similar between the two groups. Meanwhile, the male sex ratio (32.9% vs. 14.4%; p = 0.004) was higher, and the presence of Graves' ophthalmopathy (35.3% vs. 17.5%; p = 0.017), especially at a moderate to severe stage, was more frequent in the persistent group than it was in the remission group (Table 1).
p-Value by Mann–Whitney U-test.
fT4, free thyroxine; T3, triiodothyronine; TBII, TSH-binding inhibitory Ig; ATD, antithyroid drug.
The overall median ATD treatment duration was significantly longer in the persistent group than it was in the remission group: 8.7 years (range 5.7–11.5 years) versus 3.1 years (range 1.7–5.4 years), respectively, with similar median follow-up durations (p < 0.001; Table 1). However, the time from ATD discontinuation to relapse was similar between the groups at both the first and second ATD courses.
Prognostic factors of ATD treatment in GD
To explore further the predictive factors for the long-term prognosis of ATD treatment, multivariate analyses were done with clinical and treatment-related parameters comparing the remission and persistent groups defined above. Moderate to severe Graves' ophthalmopathy (odds ratio [OR] = 4.14 [confidence interval (CI) 1.13–15.17]) and an increased relapse number (OR = 4.71 [CI 2.27–9.78]) were strong predictive factors for the long-term prognosis, and a longer overall ATD treatment duration (OR = 1.43 [CI 1.20–1.70]) was also a significant factor for persistent disease (Table 2).
OR, odds ratio; CI, confidence interval.
Discussion
The present study reports on the long-term clinical course of 187 ATD-treated GD patients with a median follow-up of 11 years. Overall, 51.9% of them achieved remission, 32.1% continued ATD treatment, and 13.4% underwent other ablation treatments. The remission rates were the highest in the first ATD treatment and decreased as the ATD treatments were repeated, and the relapse rate was much higher after the third ATD treatment than it was in the preceding ones. The relapse rates of the first and second courses of ATD treatment were similar. Finally, multivariate analysis showed that the presence of moderate to severe Graves' ophthalmopathy, an increased relapse number, and a longer overall ATD treatment duration were also significant predictive factors for persistent disease. To the best of the authors' knowledge, this is the longest follow-up study in this area.
There have been several expert opinions that second-line ATD treatment or chronic, maybe lifelong, ATD treatment might be useful for the treatment of relapsed hyperthyroidism (8,24 –26). The major finding in the present study is that the first and second courses of ATD treatment showed similarly favorable clinical outcomes in contrast to the much worse outcomes after three or more courses. In good agreement with the present study, a recent study with 128 recurrent GD patients also showed relatively lower relapse rates of 24.2% at four years after the second ATD withdrawal (24). Taken together, regarding the lower relapse rate after the second ATD discontinuation in this study and others, repeating the ATD treatment once more (second course) could be a reasonable treatment option for GD patients after their first relapse.
How long the patients should be observed for after ATD discontinuation is another important issue. This study demonstrates that 50% of the relapses developed within one year after ATD discontinuation, and >90% of the relapses occurred within four years. Consistently, a Swedish study (15) also showed similar results that relapse occurred mainly during the first year, while the prognosis was excellent after four years without relapse. Based on those results, it is proposed that at least two years or up to four years of follow-up after ATD discontinuation might be considered to detect an early relapse.
Another interesting finding is that low-dose maintenance of methimazole might be beneficial in patients who repeatedly relapse. In this study, 19 patients were maintained on low-dose methimazole therapy for more than three years (median 4.0 years; range 3.0–5.9 years) with neither serious adverse events nor further deterioration of thyroid function. These data are consistent with a previous study that showed the efficiency and safety of low-dose methimazole treatment compared to RAI therapy (27). Further prospective studies are needed to validate this finding.
With a median of 11 years of long-term follow-up duration, this study shows that among the basal clinical characteristics, moderate to severe Graves' ophthalmopathy was the sole independent risk factor for persistent disease status. During the course of the treatments, the number of relapses and longer duration of ATD treatment also had predictive value for persistent disease. One of the limitations of this study is that the predictive value of TBII could not be appropriately evaluated and compared to other clinical factors. Previously, a lower TBII titer and a decrease or disappearance of TBII after treatment have been suggested as one of the prognostic factors predicting disease remission (28,29). However, the prognostic effects of TBII in these patients on ATD treatment could not be analyzed because of a large number of missing values. Additionally, TBII in this study was measured by a first-generation method, which had lower sensitivity (30). Another limitation of this study is the fact that all data were collected retrospectively (covering 1993–2000); clinical parameters including goiter size and the ophthalmopathy were described depending on physician examination and may have been variable. Further prospective studies are therefore needed.
In conclusion, a second course of ATD treatment might be beneficial in patients who relapsed for the first time, as well as in newly diagnosed patients. Ablative treatment or low-dose maintenance of ATD might be considered in high-risk patients for persistent GD who underwent more than two relapses or longer ATD treatment of more than four or five years.
Footnotes
Acknowledgments
This work was supported by the Seoul National University Hospital Research Fund (Grant No. 04-2015-0630).
Author Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.