
Abstract
Background:
The incidence of thyroid cancer has increased worldwide. The country where the incidence has increased most is South Korea. The goal of this study is to understand the magnitude of association between opportunistic thyroid cancer screening and thyroid cancer incidence, thyroid cancer subtype, and disease-specific mortality.
Methods:
We used the 2010 Korea Community Health Survey, which queried 226,873 individuals if they had been screened for thyroid cancer in the last two years. Thyroid cancer incidence data from 2008 to 2010 were obtained from the Korea Cancer registry data, and mortality data from 2007–2010 were obtained from the Statistics Korea database. The ecological association between thyroid screening and thyroid cancer incidence and mortality by age and sex were examined across Korea's 16 administrative regions by general linear regression models.
Results:
Between 2008 and 2010, the incidence of thyroid cancer was 64.1 per 100,000 individuals: the incidence in females was 107.3 and in males was 21.1. There was a strong positive correlation between regional thyroid cancer screening and regional thyroid cancer incidence (r = 0.77, [95% confidence interval 0.70–0.82]). The magnitude of correlation was higher for females (r = 0.88 [CI 0.83–0.92]) than in males (r = 0.76 [CI 0.67–0.84]) in any age group. Thyroid screening was only associated with increased detection of papillary thyroid cancer (r = 0.74 [CI 0.59–0.88]); and not associated with mortality (r = −0.08 [CI −0.59–0.63]) due to thyroid cancer.
Conclusions:
The magnitude of association between thyroid cancer screening in South Korea and the incidence of thyroid cancer strongly suggests that screening is the most important driver of the epidemic of thyroid cancer, particularly among females. Thyroid cancer screening, however, was only associated with the increase of one tumor histology, papillary thyroid cancer, and it did not have any association with thyroid cancer mortality. The extent to which opportunistic thyroid cancer screening is converting thousands of asymptomatic persons to cancer patients without any known benefit to them needs to be examined carefully.
Introduction
T
Thyroid cancer screening is a potential driver of the thyroid cancer epidemic. In 1999, the government of South Korea initiated a free national screening program for several cancers under the mantra “early detection saves lives” (5 –7). Thyroid cancer screening was not included in this program; however, it soon became a common practice to offer thyroid ultrasonography to asymptomatic patients for a small fee throughout the country, with major impact on the rate of thyroid cancer (5). An analysis showed that the proportion of the population screened in a region in 2008 and 2009 was strongly correlated with the regional incidence of thyroid cancer in 2009 (4). However, the association of thyroid screening with incidence of thyroid cancer in different age groups and across sexes, as well as the influence of screening on thyroid cancer mortality, and type of thyroid cancer remains unclear.
The Korean Community Health Survey (KCHS) is a nationwide annual health interview survey carried out by the Korean government to estimate the personal lifestyle and health behavior of adults aged ≥19 years (8). Respondents without a previous cancer diagnosis were asked about their experiences with screening for common cancers. In the 2010 survey, 229,229 people were asked whether or not they have undergone thyroid cancer screening. This information represents an opportunity to assess accurately the incidence of thyroid cancer at a national level and to understand the magnitude of association between opportunistic thyroid cancer screening and thyroid cancer incidence.
Methods
Data source
Data for this study were obtained from three sources: KCHS, the Korea Central Cancer Registry, and the Statistics Korea database.
Thyroid cancer screening
Thyroid cancer screening data were obtained from KCHS data in 2010. This population-based, cross-sectional survey was designed to investigate the health status, health behaviors, and health care utilization in each region. There are 16 regions in Korea. These regions reflect historical, geographical, but mainly administrative boundaries. A multistage probability sampling design was used to select participants.
The KCHS was administered by trained interviewers. On average, this survey consists of 180 questions with a completion rate of 97% (8). Eligible participants are asked about sex, age, residence, years of education, household income, marital status, and occupation. For health-related behaviors, smoking, alcohol use, and regular exercise were measured. For cancer screening experiences, participants were asked about their screening experiences: “Have you undergone cancer screening during the last 2 years?” Screening was conducted for each of following cancer types: for men, gastric cancer, liver cancer, colon cancer, prostate cancer, thyroid cancer; for women, breast cancer and cervical cancer were added and prostate cancer was omitted. Those who had a previous cancer diagnosis were not asked this question.
We identified all individuals over 20 years old who responded to the 2010 survey. We excluded participants who were missing information on cancer screening. A total of 2356 participants were excluded due to missing information (529 subjects) or age younger than 20 years old (1827 subjects). The final analysis used data from 226,873 subjects. Individual data of these eligible participants was used to calculate thyroid cancer screening prevalence in the 16 administrative regions.
Thyroid cancer incidence and mortality
Thyroid cancer incidence data from 2008 to 2010 were obtained from the Korea Cancer registry data which covers the entire population and is maintained by Korea National Cancer Center (6). The Cancer registry data include information on demographics, tumor histology and regions. Cancer cases were classified according to the International Classification of Diseases, 10th edition (ICD-10). Completeness of incidence data for 2010 was 97.1%. We obtained age- and sex- specific incidence data of thyroid cancer in 16 administrative regions. Mortality data from 2007–2010 were obtained from Statistics Korea database (9). Cause of death was coded and classified according to ICD-10. From the Statistics Korea database, we identified thyroid cancer deaths cases, by extracting those in whom the cause of death was coded as C73 (malignant neoplasm of thyroid cancer), which was used to calculated mortality in study region.
Data analysis
We calculated age- and sex-specific screening prevalence for 16 administrative regions. In calculating screening prevalence by the region, the multistage probability sampling design was considered. We also computed annual age- and sex-standardized thyroid cancer incidence by the region for each year. Incidence rates were calculated by dividing the number of incident cases of thyroid cancer by of the total population in the region. The 2010 population was used as the standard population. Each year, from 1 January 2007 to 31 December 2010, for each region, we also computed thyroid cancer mortality for men and women and for 10-year age categories. Mortality was calculated by dividing number of deaths during a year by the total population. Population data were also obtained from Statistics Korea using the resident registration population on July 1 of specified years. General linear regression models with 95% confidence intervals (CIs) and their associated p-values were used to evaluate the association between thyroid screening and thyroid cancer incidence, mortality by age and sex and 10-year age group by 16 regions. Figures depicting the age-adjusted incidence and mortality were prepared by plotting the rates
Results
In 2010, 226,873 people from 16 administrative regions responded to the survey. From this cohort of patients, 31,701 (13.9%) reported having been screened for thyroid cancer in the last two years. The majority of those screened were females (63%), between the ages of 50 and 59 years (28%) and lived in either the Southeast (26%) or Southwest (23%). Table 1 shows the characteristics of the screened cohort. Between 2008 and 2010, the incidence of thyroid cancer was 64.1 per 100,000 people: in females 107.3 and males 21.1 per 100,000 people. The incidence of papillary thyroid cancer was 62.4 per 100,000 people: in females 104.7 and males 20.2 per 100,000. Between 2007 and 2010 the mortality of thyroid cancer was 0.7 per 100,000 people.
The geographic regions include: Seoul; Northwest (Gyeonggi, Incheon); Southeast (Busan, Daegu, Ulsan, Gyeongbuk, Gyeongnam); Southwest (Gwangju, Chenbuk, Chunnam); Northeast (Gangwon, Jeju); and Central (Chungbuk, Chungnam, Daejun).
There was a strong positive correlation between regional thyroid cancer screening and regional thyroid cancer incidence (r = 0.77 [CI 0.70–0.82]). In a linear regression analysis, an absolute 1% increase in screening frequency was associated with a 7 per 100,000 increase in overall thyroid cancer incidence. Geographic areas with high screening prevalence were associated with a higher incidence of thyroid cancer (Fig. 1). The magnitude of the correlation was higher for females (r = 0.88 [CI 0.83- 0.92]) than in males (r = 0.76 [CI 0.67–0.84]) in any age group (Figs. 2 and 3). Furthermore, thyroid cancer screening was not correlated with thyroid cancer mortality in any sex or age group (r = −0.08 [CI −0.59–0.63]). Finally, thyroid screening was only associated with increased detection of papillary thyroid cancer (r = 0.74, [CI 0.59–0, 88]); and not associated with any other type of thyroid malignancy. (r = −0.17 [CI −0.57–0.36]) (Fig. 4) (Supplementary Tables S1–S3 show raw regional data; Supplementary Data are available online at
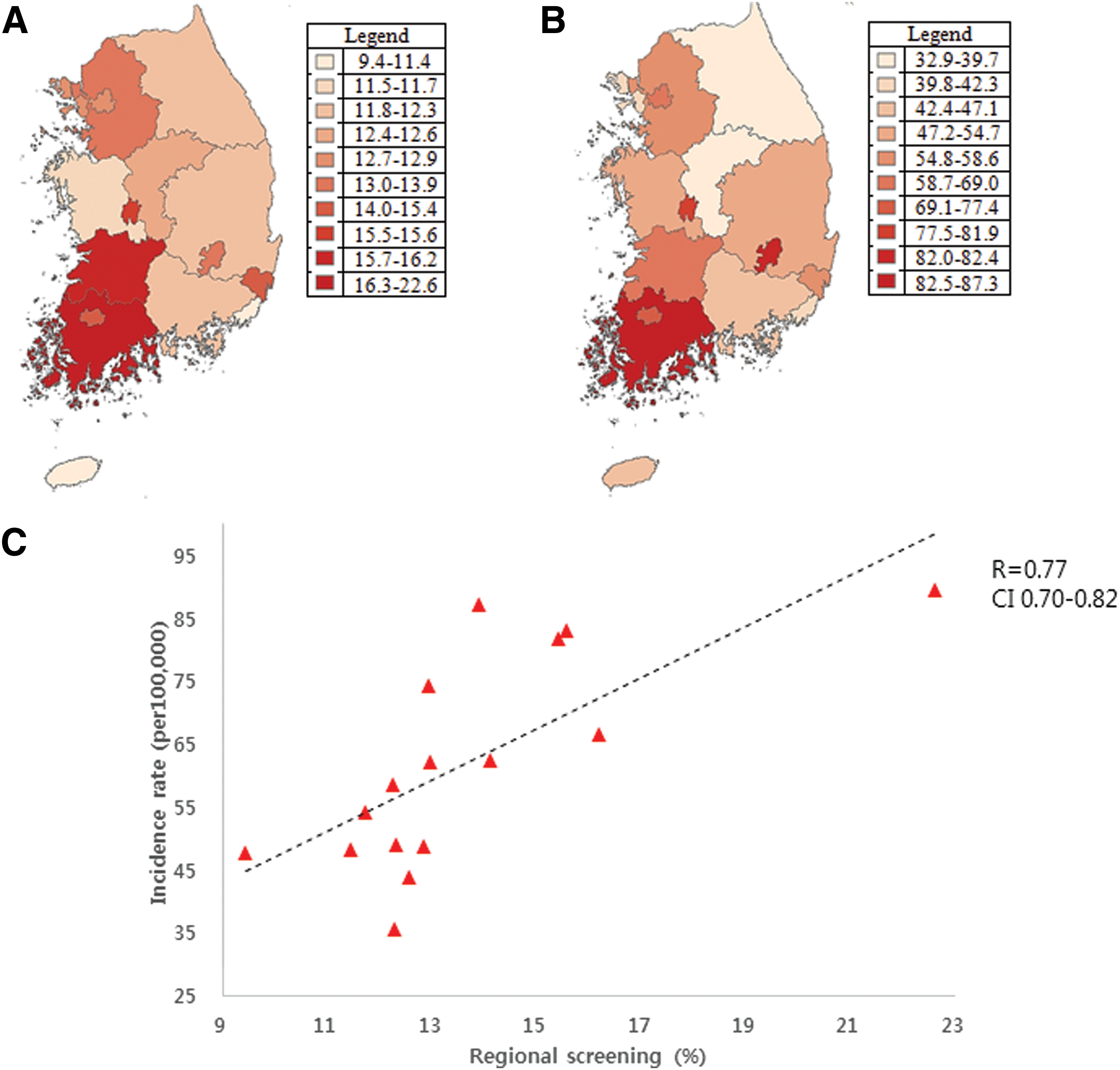
Thyroid cancer screening rate (
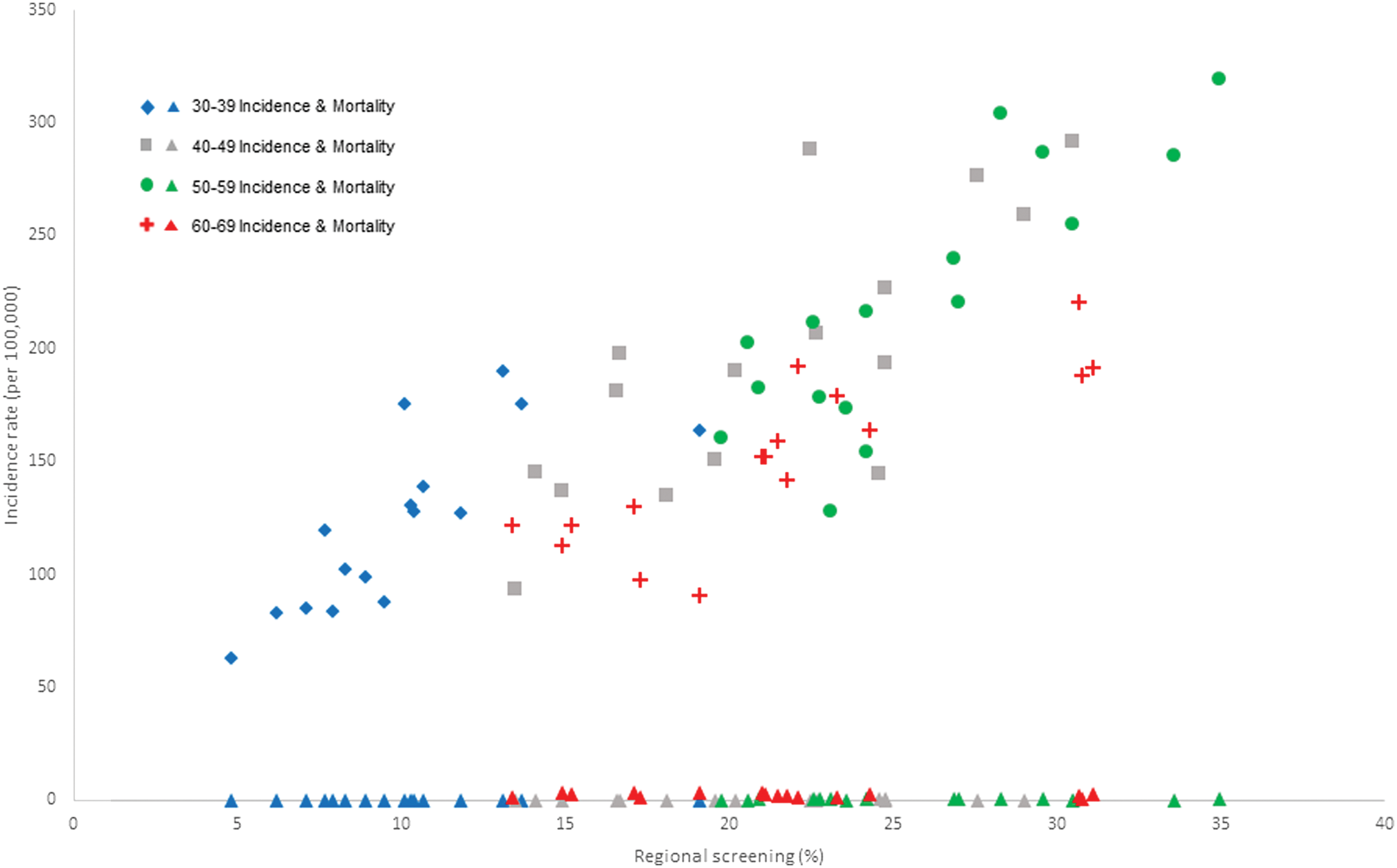
Regional screening rates and incidence and mortality of thyroid cancer by age (females). Each dot represents a region. Color images available online at
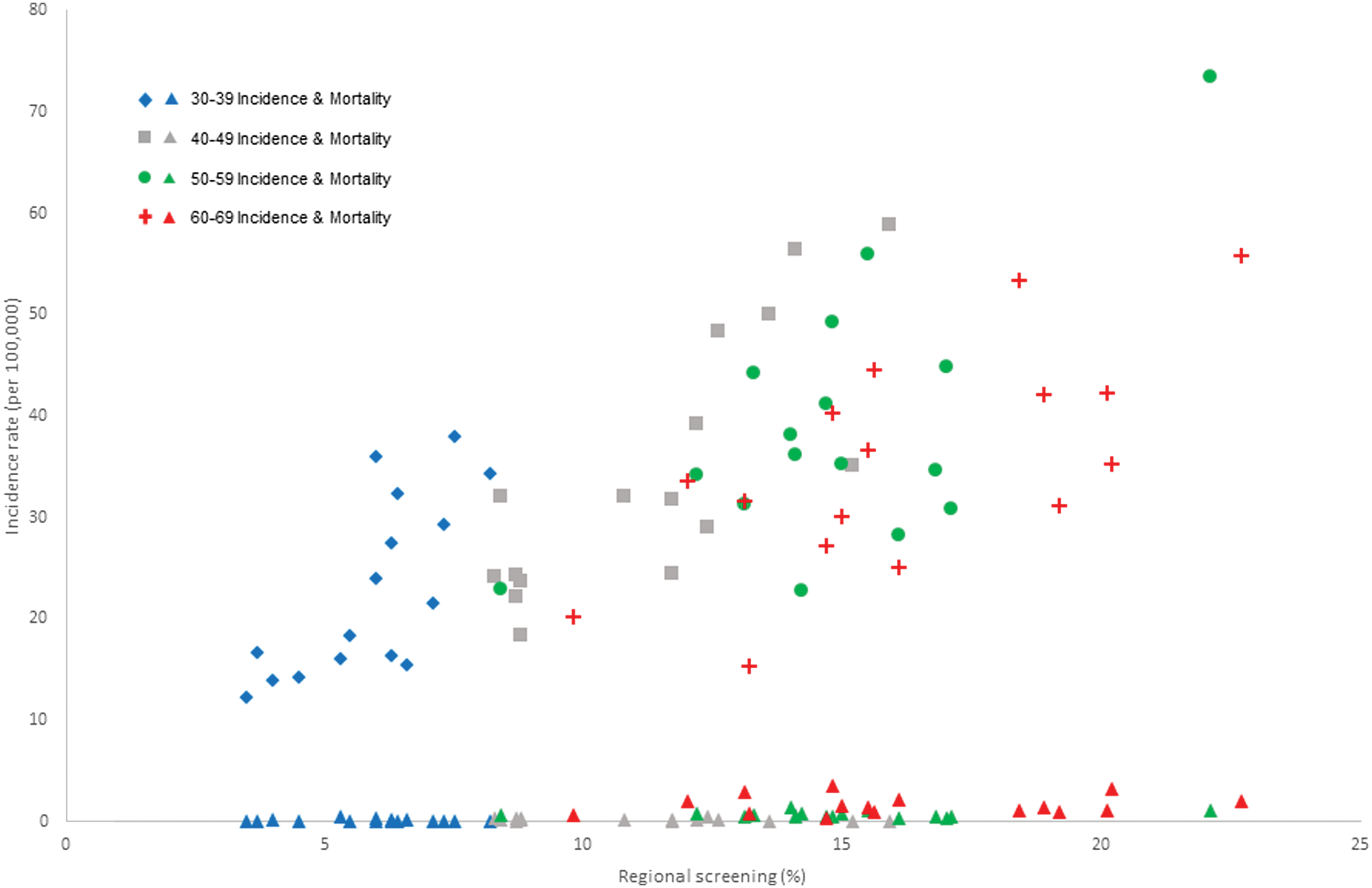
Regional screening rates, incidence and mortality of thyroid cancer by age (males). Each dot represents a region. Color images available online at
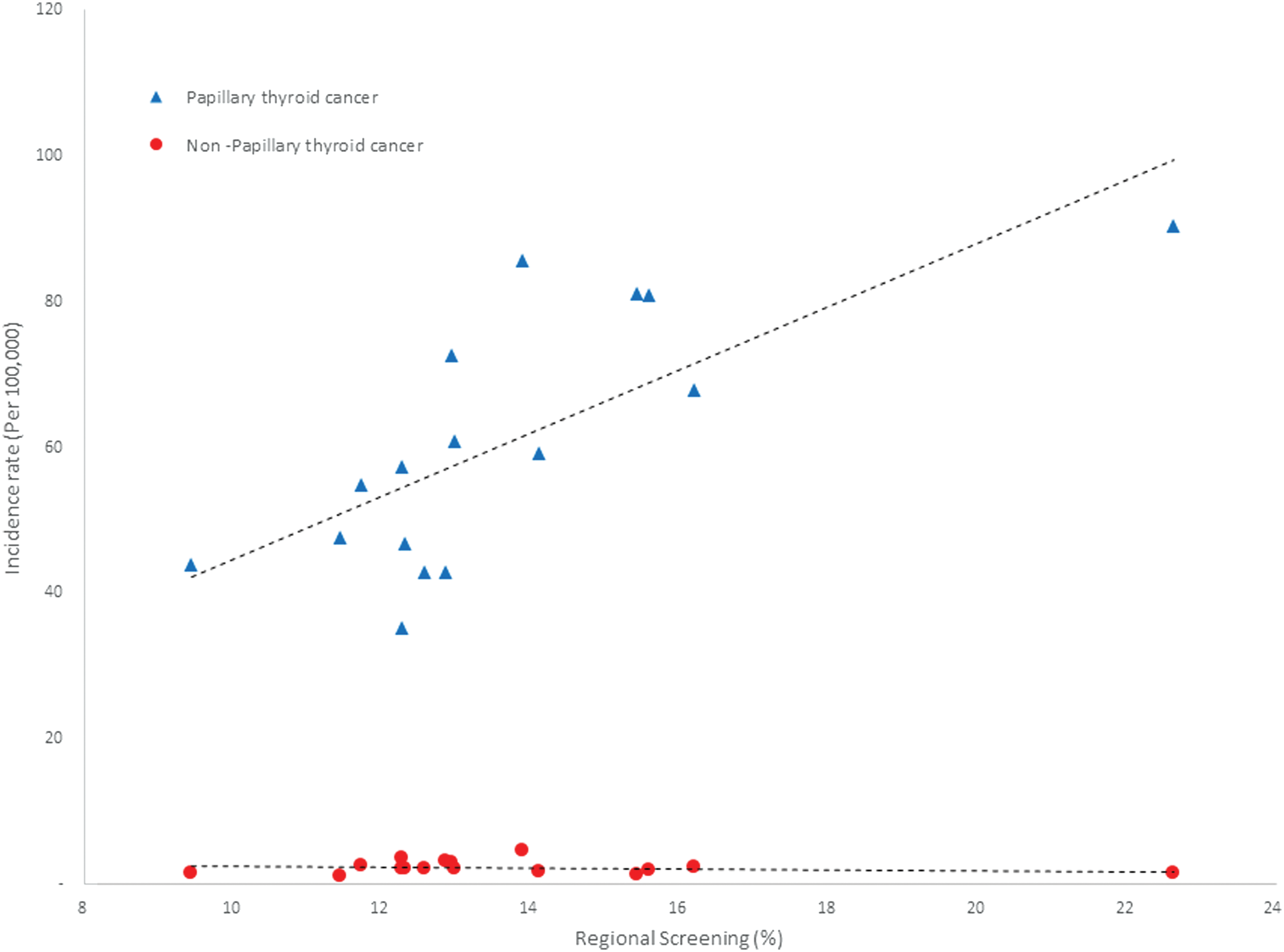
Correlations between regional thyroid cancer screening and incidence rate by type of thyroid malignancy. Each dot represents a region. Color images available online at
Discussion
Thyroid cancer incidence is increasing worldwide, but most rapidly and dramatically in South Korea. One potential driver of this epidemic is cancer screening. We found that the prevalence of thyroid cancer screening is 14%. Our confidence in this estimate is high, as it replicates the one reported from an analysis of 2000 adult Koreans in 2009 (screening prevalence 13.2%) (10). Additionally, we found that regional thyroid cancer screening was positively and strongly associated with the regional thyroid cancer incidence. Furthermore, the high prevalence of screening was also associated with higher incidence rates of papillary thyroid cancer but not with other histological types or disease specific mortality.
Although this ecological analysis does not us allow us to conclude causality between screening and thyroid cancer incidence, the lack of other risk factors for thyroid cancer in South Korea (radioactive fallout from nuclear weapons or power plant accidents affecting the entire population), the parallel increase of thyroid cancer cases at the time of initiation of the national screening program and the degree of association between screening prevalence and thyroid cancer incidence support the hypothesis that the main driver of the dramatic increase of thyroid cancer in this county is screening (4).
The association of more papillary thyroid cancers with higher thyroid cancer screening prevalence strongly supports the hypothesis that new incident cases of thyroid cancer belong to a large reservoir of thyroid cancer (a large group of asymptomatic people who carry small papillary thyroid cancers) (1,11 –13). This increased detection of new thyroid cancer cases, unfortunately, has led to more patients undergoing thyroid surgery (13). The standard practice in South Korea is to treat every patient with thyroid cancer, regardless of size and type, by surgically removing the thyroid gland (14). This procedure, while safe for the majority of patients, will cause voice problems or low calcium levels in approximately 1–10% of the patients (15 –17). Likewise, these patients will be required to take thyroid hormone replacement for the rest of their lives.
Efforts to curtail the overdiagnosis and overtreatment of thyroid cancer have occurred in this country. On March 18, 2014, a group of physicians held a press conference to urge that ultrasonography screening for thyroid cancer be discontinued in Korea (5,18). Despite the large media coverage and several government hearings, there has been little impact on clinicians’ attitudes towards screening. This may be due to the longstanding belief that early detection and treatment is better. Indeed, a recent focus group revealed that the large majority of Korean women who had undergone thyroid cancer screening were unaware of the potential for overdiagnoses; moreover, information about overdiagnosis had little impact on their beliefs about thyroid cancer screening and their intentions to undergo future screening (19).
Implication for other countries
Similar to South Korea, evidence suggests that increased detection of a subclinical reservoir—rather than a true rise of the disease—drives the incidence of thyroid cancer in several countries. In the United States, for instance, several studies support the role of high tech imaging as a major trigger of this detection (20 –23). An analysis of the National Program of Cancer Registries demonstrated that the employment of cervical ultrasonography in a geographic area was strongly associated with thyroid cancer incidence (24). Similarly, annual computed tomography scan volume is also correlated with the incidence of subcentimeter thyroid cancers (r = 0.98, p < 0.01) (25). Finally, a retrospective study of 473 patients showed that 2 out of 5 patients undergoing thyroid surgery for thyroid cancer were diagnosed incidentally by the use of imaging studies (26). Interestingly, the latter study also showed that one third of tumors larger than 2 cm were first detected on an imaging study suggesting that the reservoir of thyroid cancers may also harbor tumors larger than 1 cm in size.
Although the role of the use of imaging technologies on thyroid cancer detection is known in the United States, the role of thyroid cancer screening is unclear. Recently, however, a population based study in Olmsted, Minnesota, found that one-third of all cases of thyroid cancers between 2000 and 2012 were found on physical exam on asymptomatic patients, implying that opportunistic thyroid cancer diagnosis also occurs outside of the South Korea (12). Thus, the screening and overdiagnosis of thyroid cancer in South Korea should serve as a cautionary tale for the rest of world, particularly among countries where the incidence of this condition rises rapidly, as in the United States.
Limitations
Our analysis has several limitations and the results reported here must be interpreted in light of the strengths and weaknesses of the study. This is an ecological analysis; therefore, our conclusions are at risk of ecological fallacy. Ecological fallacy occurs when conclusions about individuals are based only on analyses of group data. For instance, we were not able to correlate whether or not individuals reporting being screened in the survey were diagnosed with thyroid cancer, and thus, the exact frequency with which patients undergoing thyroid cancer screening are diagnosed with thyroid cancer is still unclear. Moreover, the survey asked the individuals about thyroid cancer screening with thyroid ultrasonography; however, thyroid cancer screening is also conducted with neck palpation. Thus, it is possible that the prevalence of thyroid cancer screening here may be underestimated.
Whether thyroid cancer screening prevents mortality of slow or nongrowing thyroid cancer could not be examined with this study design. Finally, the geographic distribution of thyroid cancer screening and higher incidence of thyroid cancer occurred in clusters, and showed significant geographic variation. However, the reason for this pattern could not be explored in this analysis.
Conclusions
The magnitude of association between thyroid cancer screening in South Korea and the incidence of thyroid cancer strongly suggests that screening is the most important driver of the epidemic of thyroid cancer, particularly among females. Thyroid cancer screening, however, was only associated with the increase of one tumor histology, papillary thyroid cancer, and it did not have any association with thyroid cancer mortality. The extent to which opportunistic thyroid cancer screening is converting thousands of asymptomatic persons to cancer patients without any known benefit to them needs to be examined carefully.
Footnotes
Author Disclosure Statement
No competing financial interests exist.