
Abstract
Background:
The role of thyrotropin (TSH) on the cardiovascular system has been poorly investigated. It is unknown whether the changes in the vasculature associated with thyroid diseases result from altered thyroid hormone action or whether they are a consequence of a direct effect of TSH on endothelial cells. The present study was designed to evaluate the endothelial response of coronary flow to TSH in patients with differentiated thyroid cancer (DTC) without cardiovascular risk factors.
Methods:
The study population consisted of three men and seven women (M age = 32.6 ± 8 years) who underwent total thyroidectomy for DTC. All were receiving therapy with L-thyroxine to maintain TSH within the reference range. No patient was obese, or had hypertension, diabetes, or dyslipidemia. Patients underwent standard echo-Doppler examination with evaluation of the coronary flow reserve (CFR) of the distal left anterior descending artery obtained by cold pressure test (CPT) before and 24 h after the second recombinant human TSH (rhTSH) injection.
Results:
Left ventricular morphology and systolic and diastolic function were normal in all patients. Levels of thyroid hormones and thyroglobulin and antithyroglobulin antibodies did not differ significantly pre- versus post-rhTSH treatment, whereas TSH levels were higher after rhTSH administration. Blood pressure and heart rate were not affected by rhTSH. Coronary flow peak velocity at rest (22.3 ± 6 vs 23.2 ± 8.7; p = 0.66) did not differ between baseline and 24 h after rhTSH, while post-CPT velocity (29.3 ± 6.8 vs 34.4 ± 10.9; p < 0.05) and the CFR were higher after rhTSH administration (1.32 ± 0.2 vs. 1.53 ± 0.2; p < 0.01).
Conclusions:
rhTSH administration may improve the CFR after the non-pharmacological stressor CPT in DTC patients. The increase of coronary blood flow after rhTSH suggests that TSH may exert a protective effect on the coronary endothelium.
Introduction
T
Thyroid hormone deficiency reduces NO availability and increases system vascular resistance and arterial stiffness, thereby resulting in endothelial dysfunction (6 –8). This effect can occur also in the coronary endothelium of patients with subclinical hypothyroidism without associated cardiovascular risk factors (9). Early and reversible atherosclerosis has been reported in patients with subclinical hypothyroidism (10 –12), which can lead to an increased risk of coronary heart disease events and mortality in untreated patients (13).
The potential pathophysiological role of the thyrotropin (TSH) receptor in the cardiovascular system is unclear because it has been poorly investigated in vivo. In fact, only a few studies have assessed the expression of the TSH receptor in the cardiovascular system in humans, mainly because of the difficulty in separating its cardiovascular effects from those exerted by thyroid hormone in patients with thyroid dysfunction (14 –17). In vitro studies identified the TSH receptor in extrathyroidal tissues (18). In the heart, the TSH receptor has been found in ventricular myocytes, in smooth muscle cells of the vessel walls, and in endothelial cells from human aorta and cardiac tissue (19 –24).
Thyroidectomized patients with differentiated thyroid cancer (DTC) represent an ideal experimental model with which to assess the acute effects of TSH on the cardiovascular function. In fact, replacement doses of L-thyroxine (LT4) enables these patients to maintain euthyroidism, so that one can evaluate the effects of serum TSH without stimulating TSH-dependent thyroid hormone secretion. The studies conducted so far to evaluate the effects directly exerted by TSH in the peripheral vascular endothelium in thyroidectomized patients have produced conflicting results (15 –17). Moreover, the effect of TSH on coronary endothelial cells has never been directly studied in humans.
The aim of this study was to investigate the endothelial response of coronary flow to recombinant human TSH (rhTSH) in disease-free patients with DTC without cardiovascular risk factors in order to assess the effects of TSH on coronary endothelium.
Methods
Study population
The study population consisted of 10 consecutive patients (three men and seven women; M age = 32.6 ± 8 years) who underwent total thyroidectomy for DTC attending the outpatient thyroid cancer clinic at the Federico II University Hospital of Naples. The study protocol was approved by the Ethics Committee of the Federico II University Hospital of Naples, and all patients provided informed consent to the study. All enrolled patients had low-risk DTC according to the American Thyroid Association guidelines (25). No patient had antithyroglobulin antibodies. Patients were receiving LT4 in order to maintain TSH within the reference range (M dose = 1.97 μg/kg/day; range 1.68–2.16 μg/kg/day). Strict patient selection was carried out in order to exclude any factors that could confound the evaluation of the coronary flow reserve (CFR) (26 –29).
Exclusion criteria were pregnancy, obesity (body mass index [BMI] ≥30 kg/m2), arterial systemic hypertension, diabetes mellitus, insulin resistance, dyslipidemia, heart disease, cardiac rhythm abnormalities, hepatic or renal disorders, cigarette smoking, a personal or family history of coronary artery disease, and the assumption of any kind of medication apart from LT4. Dyslipidemia was defined as total cholesterol ≥200 mg/dL and/or triglycerides ≥160 mg/dL; and arterial hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg. Insulin resistance index, HOMA, was assessed with the homeostasis model of insulin resistance (insulinemia [mIU/L] × glycemia [mmol/L])/22.5) (30,31). Coronary artery disease was excluded based on clinical history and stress electrocardiogram. Hepatic and renal diseases were excluded on the basis of the history and laboratory tests (transaminases and creatinine).
Study protocol
This study was performed during the periodical monitoring of the DTC patients after the administration of rhTSH to determine stimulated thyroglobulin (Tg) levels. Following surgery, patients received two intramuscular injections of rhTSH at a dose of 0.9 mg each on two consecutive days. Serum TSH, thyroid hormones, Tg, antithyglobulin antibodies (TgAb), and metabolic parameters (weight, height, BMI, glycemia, total cholesterol, and triglycerides) were determined at baseline. Serum TSH, thyroid hormones and Tg were re-evaluated 24 h after the second injection of rhTSH. Replacement doses of LT4 remained unchanged throughout the study. Patients underwent standard Doppler echocardiography with the evaluation of the CFR of the left anterior descending artery by the cold pressure test (CPT) before and 24 h after the second rhTSH injection.
Assessment of thyroid status
Blood samples for circulating serum TSH, free triiodothyronine (fT3), free thyroxine (fT4), Tg, and TgAb were collected from the antecubital vein between 07.00 and 08.00 h after an overnight fast. TSH levels were measured with an electrochemiluminescence immunoassay (ECLIA; Elecsys and Cobas analyzers, Roche Diagnostics) that has a sensitivity of ≥0.005 mIU/L (reference range 0.3–4.2 mIU/L). Serum fT3 and fT4 were also measured with the ECLIA system. Sensitivities were <0.400 pmol/L and <0.300 pmol/L for fT3 and fT4, respectively. The reference ranges were 3.1–6.8 pmol/L and 12–22 pmol/L for fT3 and fT4, respectively. Serum Tg levels were also measured with ECLIA, with a sensitivity of ≤0.1 ng/mL (reference range 0.1–50 ng/mL). Serum TgAb levels were measured with ECLIA (reference range 0–115 IU/mL).
Standard echocardiographic assessment
Echo-Doppler examinations were performed with a Vivid Seven Sound machine (GE) equipped with a 2.5 MHz phased-array transducer with harmonic capability.
Echocardiographic quantitative analysis was done according to laboratory standards (32). Left ventricular mass was calculated according to the American Society of Echocardiography recommendations, and was normalized for height in meters powered to 2.7 (33). Left ventricular end-diastolic and end-systolic volume was measured in apical four- and two-chamber views, and left ventricular ejection fraction calculated according to the standard formula. Standard pulsed Doppler imaging of mitral inflow was recorded in the apical four-chamber view. Early (E) and atrial (A) peak velocities (m/s) and their ratio, E velocity deceleration time (ms), and isovolumetric relaxation time (ms) were measured. Pulsed tissue Doppler-derived early diastolic velocity (e′) of septal and mitral annulus were measured and averaged. The E/e′ ratio was derived as a non-invasive estimate of left ventricular filling pressure. Echo-Doppler methods and the reproducibility of the laboratory are reported elsewhere (34 –36). All images were analyzed offline by two observers who were blind to the patients' clinical characteristics.
CFR
Coronary flow was visualized in the distal left anterior descending artery by transthoracic Doppler echocardiography with a 5 MHz shallow-focus phased-array transducer. Doppler sample volume was placed on the color signal of the left anterior descending artery, and the spectral pulsed Doppler signal was recorded to look for the characteristic biphasic flow pattern with a larger diastolic and a smaller systolic component both at rest and after the CPT. Coronary diastolic peak flow velocities (cm/s), heart rate, and blood pressure were measured at rest and soon after the CPT at maximal endothelial induced hyperemia. The CFR was calculated as the ratio of hyperemic-to-resting diastolic peak velocities. The CPT was performed according to a standardized protocol by placing the subject's hand and distal part of the forearm in an ice water slurry for 4 min (9,27). The highest three spectral Doppler signals were averaged for each parameter. The reproducibility of our CPT-derived CFR measurements of the echo laboratory are: an intra-observer variability of 2.0% and an inter-observer variability of 4.5%, as previously reported (26). All images were analyzed offline by two observers who were blinded to the clinical characteristics of the patients. All examinations were performed between 08.00 and 09.00 h. All patients were fasting and abstained from coffee for at least 12 h before testing.
Statistical analysis
IBM SPSS Statistics for Windows v20 (IBM Corp.) was used for statistical analyses. All data are presented as mean values ± standard deviation (SD). An analysis of variance was used to assess intergroup differences. Linear regression analyses and the partial correlation test using Pearson's correlation method were used to test univariate relations. Differences were considered statistically significant at p < 0.05.
Results
The clinical, demographic, and anthropometric characteristics of the patients at baseline (before the first injection of rhTSH) are shown in Table 1. In accordance with the exclusion criteria, no patient was obesity (BMI 24.51 ± 2.46 kg/m2), hypertension (SBP 115 ± 14.1 mmHg and DPB 68.5 ± 9.4 mmHg), dyslipidemia (total cholesterol 177.9 ± 16.5 mg/dL and triglycerides 66.2 ± 16.8 mg/dL), or hyperglycemia (84.8 ± 6.7 mg/dL). As a consequence of replacement doses of LT4, the TSH level at baseline was 1.25 ± 0.37 μIU/mL, and serum fT3 and fT4 were within the reference range. No patient had TgAb or elevated Tg values. The left ventricular structure and the systolic and diastolic function on echo-Doppler analysis were normal in all patients (Table 2).
Data are expressed as means ± SD.
TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine; TgAb, antithyglobulin antibodies; Tg, thyroglobulin; SD, standard deviation.
E, transmitral early peak diastolic velocity; A, transmitral atrial peak velocity; e′, early diastolic velocity of septal annulus.
Table 3 shows the results of the CFR at baseline and at 24 h after the second rhTSH injection. Of note, no adverse events were recorded during rhTSH administration. TSH levels were significantly higher than at baseline after rhTSH administration (147 ± 37 μIU/mL vs. 0.7 ± 0.3 μIU/mL; p < 0.001), whereas thyroid hormones, fT3 and fT4, and Tg and TgAb levels remained unchanged. Similarly, rhTSH administration did not affect SBP (115 ± 14.1 mmHg at baseline vs. 119 ± 13.1 mmHg after rhTSH), DBP (68.5 ± 9.4 mmHg vs. 73 ± 9.7 mmHg), mean blood pressure (85 ± 9.9 vs. 83 ± 6.4), or heart rate (75.9 ± 12.9 beats/min vs. 74.6 ± 12.2 beats/min). Coronary flow peak velocity at rest was similar at baseline and 24 h post rhTSH (22.3 ± 6 vs. 23.2 ± 8.7; p = 0.66), whereas coronary flow peak velocity after the CPT was higher after rhTSH administration (29.3 ± 6.8 vs. 34.4 ± 10.9; p < 0.05). As a consequence, the CFR was significantly higher after administration of rhTSH (1.3 ± 0:2 vs. 1.5 ± 0.2; p < 0.01). The increase in myocardial work, reflected by the increase in the rate pressure product (SBP × heart rate), was significantly higher after rhTSH administration (8887.1 ± 2883.4 vs. 9880.7 ± 2717.9; p < 0.05), and was associated with a proportionate increase in myocardial blood flow.
Data are expressed as means ± SD.
CFR, coronary flow reserve; rhTSH, recombinant human thyrotropin; CPT, cold pressure test; SBP, systolic blood pressure; DBP, diastolic blood pressure; NS, not significant.
Figure 1 shows the CPT-derived coronary flow at baseline and 24 h after the second rhTSH injection in one patient. Figure 2 shows changes in coronary flow velocities after the CPT at baseline and 24 h after the second rhTSH administration in each patient. It was found that coronary flow improved after rhTSH administration in 8/10 patients (80%). The CFR 24 h after the second rhTSH injection was not significantly related to heart rate (p = 0.4), SBP (p = 0.6), DPB (p = 0.5), left ventricular mass (p = 0.8), relative wall thickness (p = 0.5), indexes of left ventricular diastolic function (a peak velocity p = 0.7; e peak velocity p = 0.7; e/a ratio p = 0.7), systolic function (p = 0.1), fasting blood glucose (p = 0.6), total cholesterol (p = 0.8), triglycerides (p = 0.6), BMI (p = 0.2), or TSH (p = 0.7).
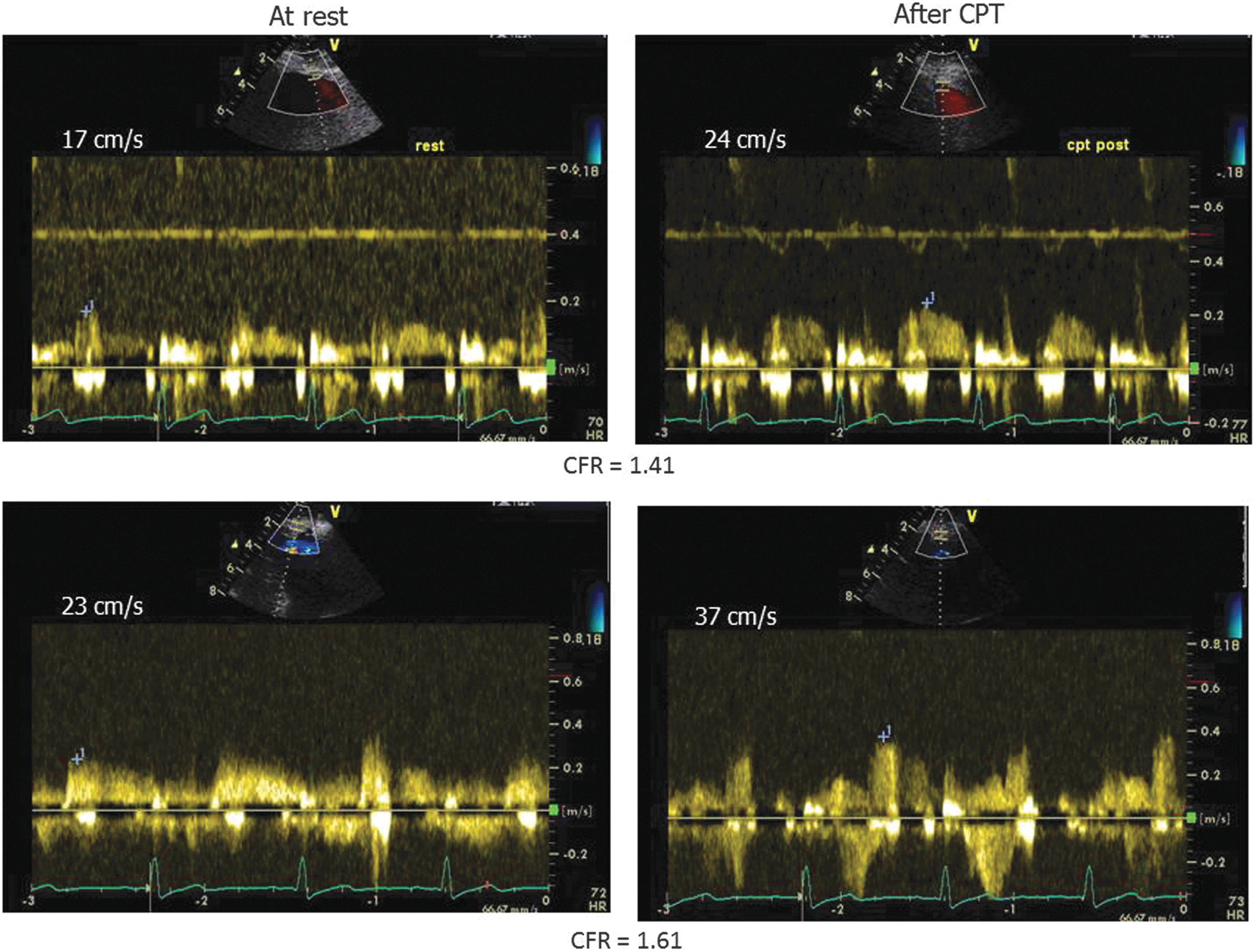
Cold pressure test (CPT)-induced coronary flow reserve at baseline and 24 h after the second recombinant human thyrotropin (rhTSH) injection in a single patient. Upper panel: Coronary flow velocities at rest and after CPT at baseline. Lower panel: Coronary flow velocity at rest and after CPT 24 h after the second rhTSH injection.

Changes in coronary flow after CPT at baseline and 24 h after second rhTSH administration in a single patient.
Discussion
To the authors' knowledge, this is the first study to evaluate the effect of TSH on the coronary endothelial function in athyreotic patients without cardiovascular risk factors during treatment with replacement doses of LT4. Given the strict patient selection, the patients were young, non-obese, non-smokers with normal blood pressure, normal cholesterol levels, with no personal or family history of coronary artery disease. The administration of rhTSH did not change heart rate, cardiac rhythm, left ventricular structure, or systolic and diastolic function in the thyroidectomized patients, thereby confirming previous results (14). Moreover, the non-pharmacological stressor CPT improved the CFR after rhTSH administration in DTC patients. Studies on the effects exerted by rhTSH on endothelial function have produced conflicting results (15 –17). Acute intrabrachial administration of rhTSH enhanced endothelium-dependent vasodilatation but not endothelium-independent vasodilatation in thyroidectomized patients and healthy volunteers (15); rhTSH improved endothelial function in the small resistance vessels, irrespective of thyroid hormone secretion. Similarly, in another study, marked activation of the endothelial-mediated vasodilatation persisted five days after the administration of rhTSH, irrespective of systemic hemodynamic changes (16). This response was mediated by endothelial mechanisms as witnessed by the finding that rhTSH did not alter the response to nitroglycerin, which is a vasorelaxing agent that acts directly on smooth muscle cells (16).On the contrary, in another study, the administration of rhTSH acutely impaired endothelium-dependent vasodilatation possibly by inducing low-grade inflammation in patient with DTC (17). The discrepancy between these studies may be related to the different methods used to evaluate endothelial function. In fact, flow-mediated dilation is an indirect index of NO bioavailability that analyzes the conduit arteries (17), whereas plethysmography is an accurate, sensitive method with which to explore resistance vessels (15). Furthermore, one study evaluated patients with DTC receiving long-term therapy with replacement doses of LT4 (15), whereas the other assessed the acute effects of rhTSH in patients receiving TSH-suppressive doses of LT4 (17).
The present study demonstrates that the non-pharmacological stressor CPT can improve the CFR after rhTSH administration in patients with DTC receiving replacement doses of LT4 (Table 3). The improvement of the CFR was mainly due to a significant increase of CPT-derived coronary flow. The increase of post-CPT coronary blood flow after rhTSH administration could be related to the direct vascular effect of rhTSH on the coronary endothelial cells. It is noteworthy that this increase was not associated with a similar increase at rest, which would suggest a direct thyroid hormone effect on the vascular coronary wall. This effect could not be considered a reflex response or a consequence of rhTSH action exerted elsewhere in the cardiovascular system because no alterations in cardiac morphology or function or changes in arterial blood pressure and heart rate were found. The lack of TgAg in the study population excludes the possibility that inflammation and autoimmunity affected endothelial function.
Study limitations
One limitation of this study is the small size of the study population, which may have resulted in the lack of statistical significance of some parameters. It was difficult to enroll young patients with low-risk DTC without cardiovascular risk factors or a family history of coronary disease, who were willing to undergo coronary reserve flow evaluation during rhTSH administration. Another limitation of this study is the lack of a well-established cutoff point for the CPT-derived coronary reserve flow. In this context, the CPT is less powerful than pharmacological stimulation, and cutoff values can be considered lower (<2) than the cutoff used by pharmacological stimulation (adenosine or dipyridamole). CPT were chosen instead of pharmacological stressors because the latter induce an increase of coronary flow, which is only partially endothelium-dependent. CPT stimulation has been validated in previous studies (26,36).
Conclusions
The present data demonstrate that acute administration of rhTSH is associated with a significant improvement in the CFR. This occurs in response to a CPT-induced physiological stimulus consequent to increased vascular reactivity mediated by a mechanism of endothelium-mediated vasodilatation. The results suggest that TSH itself exerts a protective effect on the coronary endothelium. The protective effect of TSH on the coronary endothelium is direct and not mediated by modification of thyroid hormones because no change in serum thyroid hormone levels was observed after rhTSH. In a recent study, patients with DTC had a higher risk of cardiovascular mortality (37). Moreover, low TSH levels predicted cardiovascular mortality (37). A meta-analysis of large prospective studies of patients with persistent subclinical hyperthyroidism demonstrated that undetectable serum TSH levels (<0.1 mIU/L) can be associated with an increased risk of coronary heart disease mortality (38). However, the mechanism leading to this amplified vascular risk is unclear because thyroid hormone excess has positive effects on endothelial function and metabolic parameters (5). The present data could support the concept that persistent TSH suppression in patients with subclinical hyperthyroidism could have negative effects on coronary endothelium, despite the slight increase in thyroid hormones at the tissue level.
Footnotes
Acknowledgments
We thank Jean Ann Gilder (Scientific Communication srl., Naples, Italy) for editing the manuscript.
Author Disclosure Statement
The authors declare that they have no conflict of interest.