
Abstract
Background:
A large proportion of global increase in thyroid cancer (TC) incidence has been attributed to increased detection of papillary thyroid cancer (PTC). Nonetheless, some reports support a real increase in incidence. This study aimed to perform a systematic review to evaluate the changing trends in TC incidence and summarize potential risk factors predisposing to this trend.
Methods:
Literature published in the English language between 1980 and August 2014 was searched via PubMed (MEDLINE) and OvidSP (EMBASE). Original studies on changes in TC incidence in defined geographic areas that described clear methods of case selection and population estimates were included. Data on incidence rates and risk factors were collected.
Results:
Of 4719 manuscripts, 60 studies were included, of which 31 were from Europe, 13 from North America, and the rest from Asia (n = 9), Oceania (n = 4), and South America (n = 3). Fifty-three articles reported a significant increase in incidence (highest was a 10-fold increase in South Korea), six reported stable rates, and one noted a decrease. PTC was the commonest type reported to have increased in incidence (in 10 studies with relevant data). Follicular TC increased in incidence (in four studies), albeit at a lower rate compared with PTC. Data on risk factors were sparse; factors discussed included ionizing radiation, iodine deficiency, and supplementation.
Conclusion:
This systematic review strongly supports a widespread and persistent increase in TC incidence. Evidence for over-detection of PTC as the predominant influence includes increased numbers of smaller size tumors and improved or unchanged survival.
Introduction
T
The reasons for the apparent rise in TC incidence are unclear. Improvements in detection and diagnosis of TC are thought to be one of the main reasons underlying this trend (4). A high prevalence of incidentally detected TC in autopsy studies (5) supports the presence of subclinical disease in the population. An increase largely due to incidental diagnoses is also supported by stable TC mortality rates (6), suggesting that a pool of undiagnosed, clinically insignificant cases of TC are now being increasingly identified.
The other explanation is a real increase in the incidence of TC, driven by changes to risk-factor exposure. Evidence in support of this view includes the increase in large TCs as well as smaller cancers (7). In addition, some authors have suggested that if over-detection alone is responsible for the rise, this should have resulted in a greater improvement in survival than has been observed in some studies (8).
Potential risk factors proposed in the literature that may predispose to TC include exposure to ionizing radiation, raised body mass index, and dietary and reproductive factors (9,10). Strong evidence in support of most of these factors is lacking. Exposure to ionizing radiation appears to be relatively the most important of all factors. Significant risks from childhood exposure to atomic bomb radiation have been shown to persist for several decades after the event (11). In addition, there are concerns about the increasing exposure to medical radiation, including diagnostic radiography, nuclear medicine, and radiation therapy (12).
Previous reviews on TC epidemiology (3) have focused on only a few studies. This systematic review evaluated published literature on the changes in the incidence of TC across the world, and sought to identify risk factors that have been studied alongside incidence trends.
Methods
The protocol for the review was registered with the PROSPERO register prior to commencement of the study. The protocol can be accessed at
The MEDLINE (via PUBMED) and EMBASE (Via OvidSP) databases were searched (1980–August 2014) using the terms “thyroid neoplasm,” “thyroid cancer,” “thyroid carcinoma,” and “incidence” or “epidemiology.” The search was limited to English language studies. All original studies that reported a trend or a series of incidence rates within a defined population were included in the review. Letters, editorials, commentaries, reviews, news stories, duplicate publications, studies with insufficient data, and manuscripts not including incidence rates for more than one time period or percentage change over time were excluded. Studies were also excluded if they reported incidence rates only in subgroups of populations. For example, a number of studies reporting the incidence of TC in patients with Hashimoto's disease were excluded. Conference proceedings and other sources of gray literature were excluded due the high risk of incomplete data.
The search was last performed on August 1, 2014. Studies that reported incidence as crude rates, age-adjusted rates, or as percentage change in incidence were included. Studies that only reported overall numbers of cases or proportions of different diseases without reference to the population cohort were excluded.
Titles and abstracts were reviewed by the primary researcher. A random sample of 10% of these studies was then blindly screened by a second researcher. Any discrepancies were discussed, and if necessary, a third researcher was consulted. Full texts were screened by the primary investigator. All excluded texts were independently checked by a second reviewer.
Several studies based on different versions of the Surveillance, Epidemiology, and End Results (SEER) database in the United States and covering different time periods were screened carefully to avoid inclusion of duplicate data in the review. Two studies based on data from SEER were included. One covered the largest population for the longest period of time (6). The other was used to collect incidence rates by ethnicity, which was not present in the previous study (13).
Data from each of the included manuscripts were extracted by one reviewer using a standardized proforma. A second reviewer extracted a random sample of 10% of the full texts, and any discrepancies were discussed with the third researcher.
Data collected from the studies included study characteristics (first author, journal, region, time period, and types of TC), incidence rates (described as crude rates, age standardized rates [ASR], or percentage change) for entire cohorts or for specific groups (such as sex, race/ethnicity, and histological type), details on standardization of incidence rates, the population used for standardization, risk factors, and authors' interpretation of the data.
Incidence was usually reported as ASR; standardization was commonly performed to world or European standard populations. Trends in incidence rates were presented as annual percentage change (APC) or overall percentage change. A narrative synthesis of incidence rates, including comparison of rates by region and time period, was performed. Incidence rates by subgroup (such as TC types) were also compared if data were available. Data on the risk factors associated with changing TC incidence were limited and heterogeneous.
Given the absence of validated quality-assessment tools appropriate for incidence studies of this kind, a formal, tool-based quality assessment of the included studies was not carried out. However, the method of case selection was assessed and reported. This is a criterion of quality in the Newcastle–Ottawa Scale for observational studies (14).
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed in the reporting of this review (15).
Results
Of 4722 titles and abstracts included in the initial search, 60 studies were eligible for the final synthesis. The PRISMA flow chart (Fig. 1) details the reasons for exclusions at each level of the screening process.
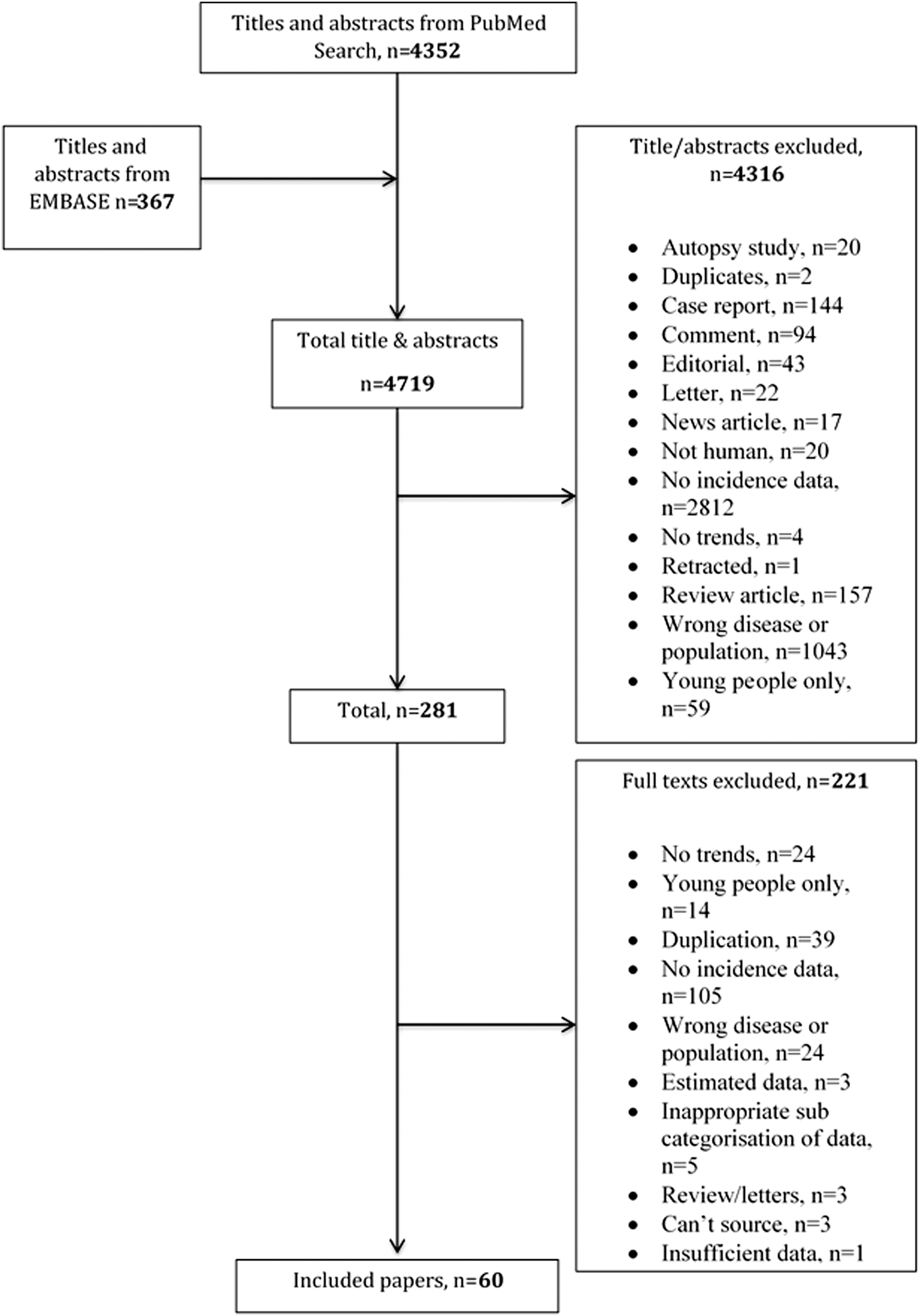
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow chart of the systematic review.
Fifty-six studies described age standardization. Of these, 19 studies used the direct method, and 37 studies did not state whether the direct or indirect method was used. In 24 articles, age was standardized to the world standard population, 11 to the European standard population, eight to the U.S. national population, one to the Italian national population, two to the Canadian national population, and one to the Puerto Rico national population. Nine studies did not state the population used for standardization.
The methods used for case selection are summarized in Table 1. The characteristics of the included studies are shown in Table 2. Overall, the majority of included studies (54/60) showed a significant increase in the incidence of TC over the past five decades. One study found inconclusive results (16). Of the four articles that reported no significant change in TC incidence, one study presented low crude incidence rates of <20 patients per year in Pakistan (17). The low incidence rates were attributed to poor education and poor access to healthcare. Another report (18) found increasing papillary thyroid cancer (PTC) and decreasing follicular thyroid cancer (FTC) rates in the Netherlands between 1989 and 2003. This was thought to be due to reduced radiation exposure, appropriate iodine intake, and a more conservative approach to incidental, asymptomatic thyroid nodules compared with other countries. Lee et al. also found stable incidence rates in Singapore between 1968 and 1977 (19). Farahati et al. also reported stable incidence rates in a German cohort (20), and postulated that the improved iodine status of the population resulted in a shift in histological subtypes of TC without a change in overall incidence.
Studies where ASR was not reported summarize the data by crude incidence rates or percentage change. Areas reporting incidence rates for multiple areas have been presented using rates from only one area. The area with the median ASR in males at the beginning of the study was chosen for presentation.
EAPC, estimated annual percentage change, calculated as average percentage change in ASR per year; ASR, age standardized rate (of incidence); APC, annual percentage change; SEER, Surveillance, Epidemiology, and End Results.
One study included in the review reported a decrease in TC incidence (21) in Bosnia and Herzegovina between 1999 and 2008, attributable to poor access to healthcare, probably related to war in the country at that time.
Geography
Figure 2 shows that the majority of published studies were from Europe (n = 31), followed by North America (n = 13), Asia (n = 9), Oceania (n = 4), and South America (n = 3).
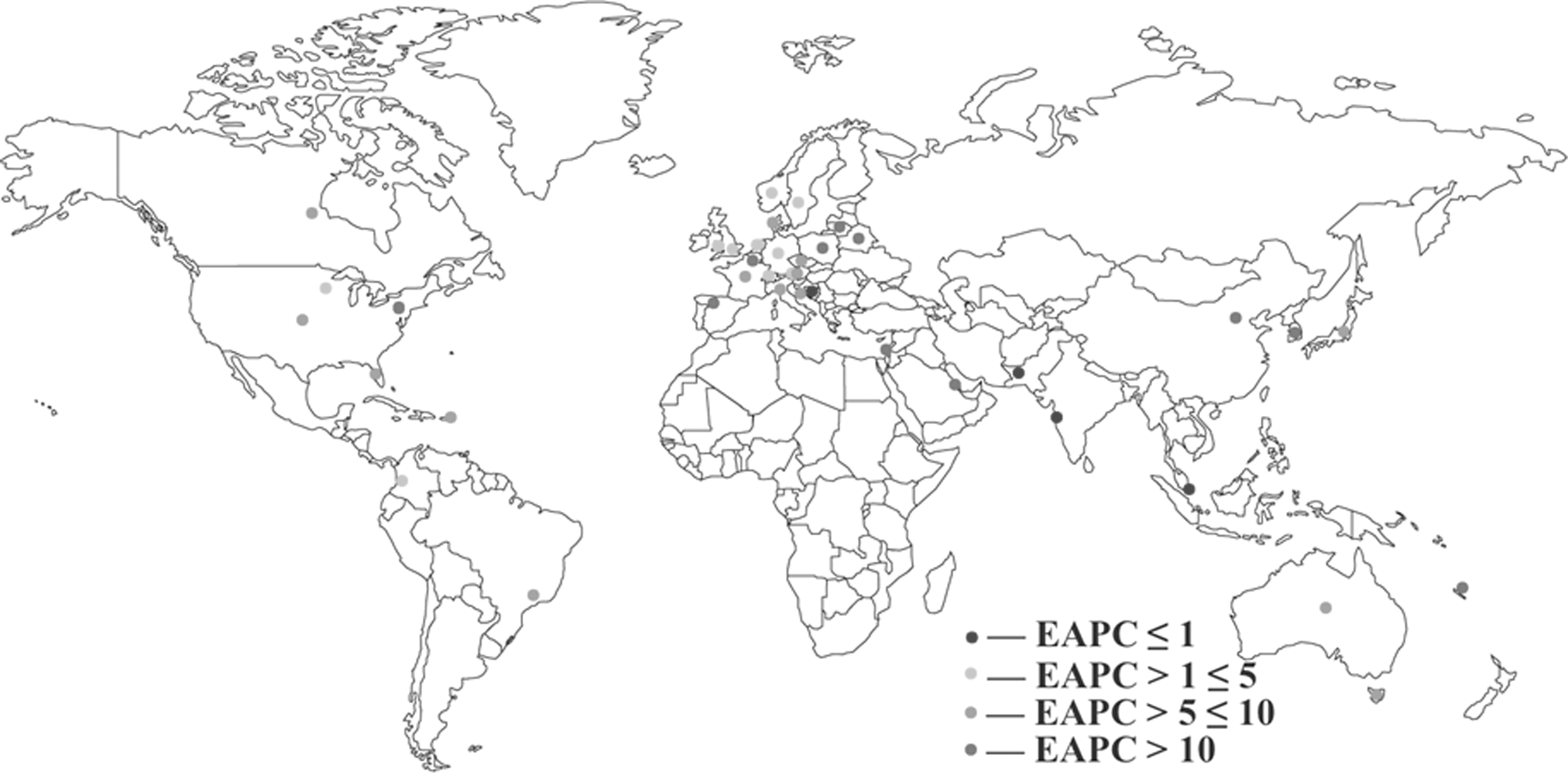
Map of expected annual percentage change (EAPC) in the age standardized rates (ASRs) of thyroid cancer.
Of the nine studies from Asia, all but two—one from Pakistan (17) and one from Singapore (19)—described increasing incidence. Studies from Japan (22), China (23), and South Korea (24) reported increasing incidence of TC over recent decades. The Korean study reported the highest incidence rates in this review. ASRs in women increased from 10.4/100,000 in 1999 to 96.8/100,000 in 2011, corresponding to an estimated annual increase of 35.3%. The rates in men increased from 2.1/100,000 in 1999 to 20.2/100,000 in 2011, corresponding to an estimated annual increase of 24%.
All 13 reports from North America reported significant increases in TC incidence. Two of the largest studies from North America (6,25) showed similarly increasing rates of TC incidence, but the conclusions about the underlying causes were different. This will be discussed later.
The largest number of studies in this review was from Europe. Like other regions, the majority of these studies reported rising TC incidence, except the ones from Germany and Bosnia discussed earlier (20,21).
Other reports included three articles from South America, including two from Brazil. One reported very high rates, but only provided crude incidence data (26). The other study from Brazil found APC in incidence rates for men and women to be higher in Sao Paulo than that in the United States (27).
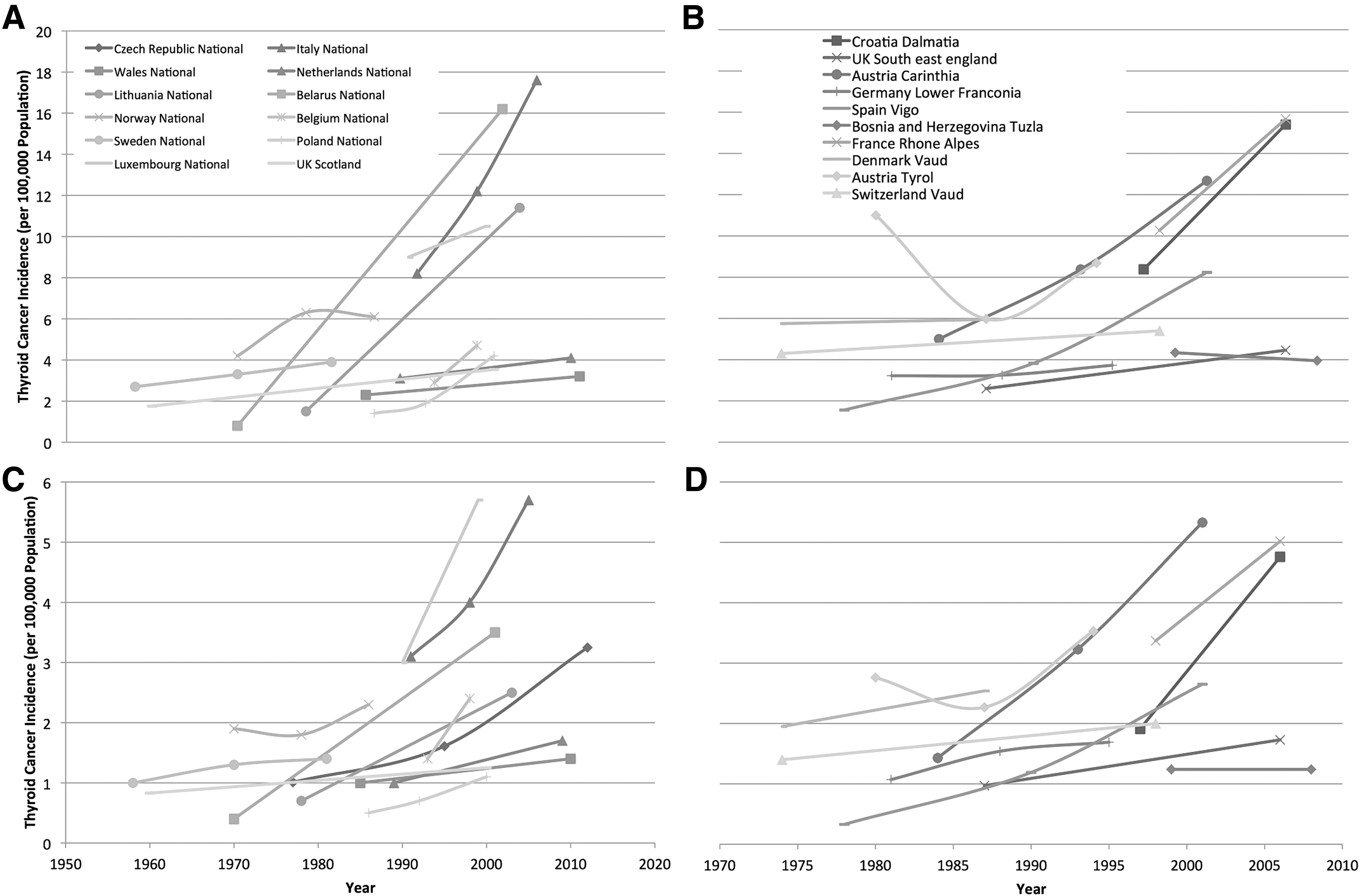
Figures 3 –5 show the trends in TC ASRs by geography. A highly variable but clearly upward trend can be seen in all regions presented. In each population, the incidence in females is higher than that in males, and this difference varies between regions as well. In some regions, ASRs in females increased much more than they did in males, and in other regions, the opposite is seen. Overall, the trend of increasing incidence is similar in both sexes, suggesting they may share a common cause.
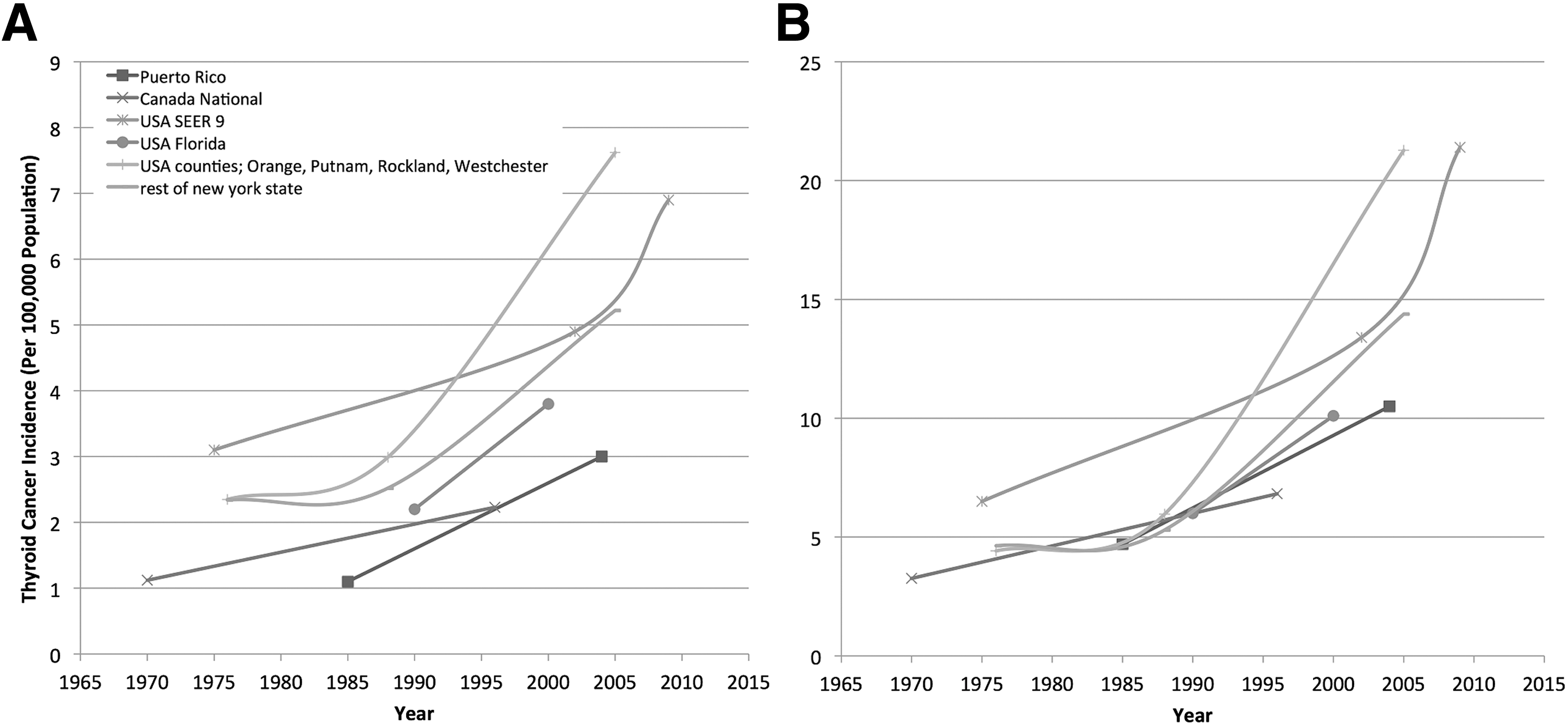
ASRs of thyroid cancer in (
ASRs of thyroid cancer by year. (
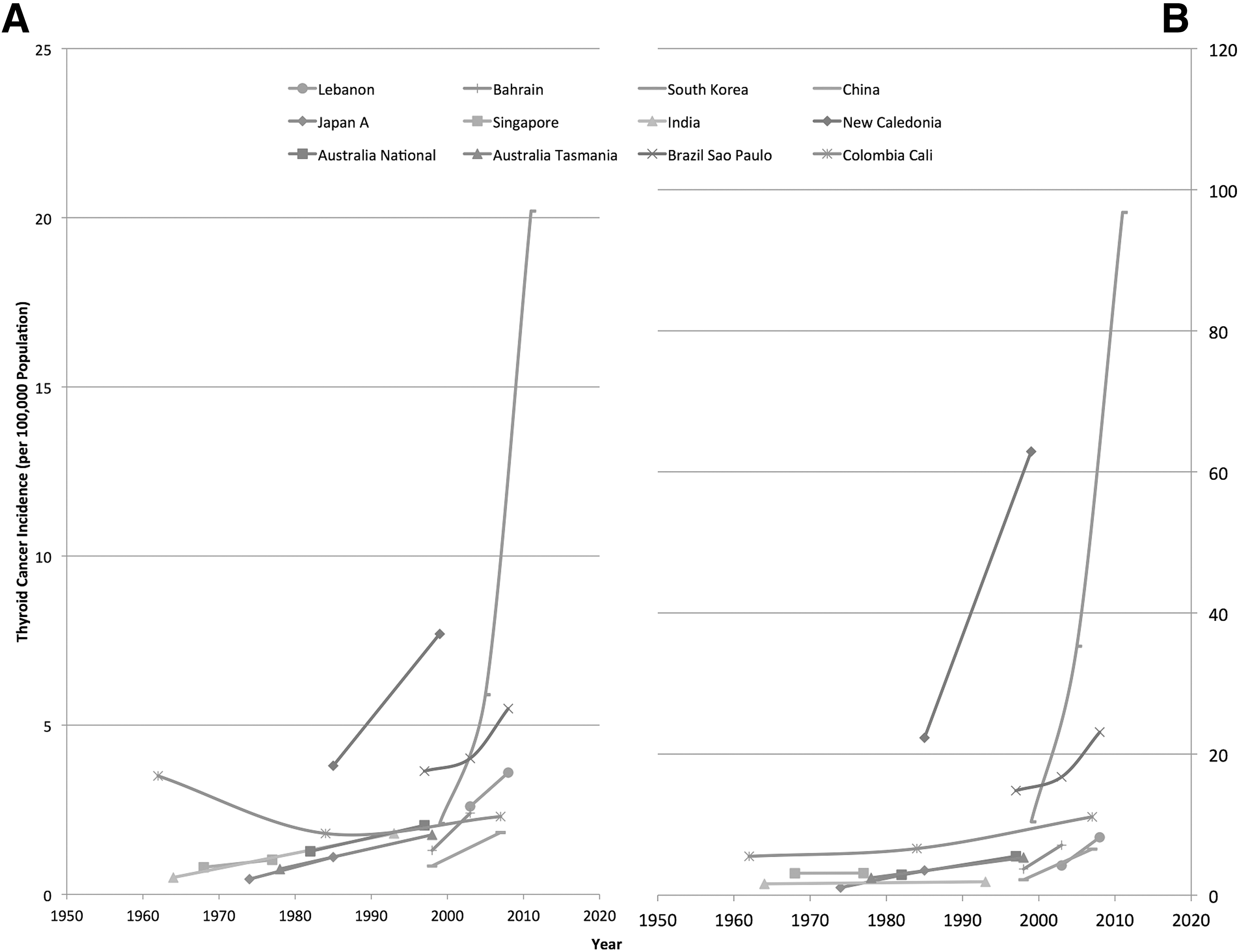
ASRs of thyroid cancer in (
Subtypes of TC
Of 10 studies that reported incidence trends for TC subtypes in adequate detail, all reported significant increases in the incidence of PTC. One article demonstrated a rise in ASR for PTC from 0.93/100,000 to 6.68/100,000 people per year in Manitoba, Canada, over the period 1970–2010 (25).
Only four of the included articles provided adequate information on the incidence trends for FTC (28 –31). Interestingly, all four studies reported increasing incidence, albeit with a slower rate of increase compared with PTC. Two studies reported incidence rates of medullary TC: one study from 2006 showed a stable rate (28), and the other showed a slight increase in incidence from 1978 to 1997 (30). The incidence of anaplastic TC incidence was reported in three studies. One report with data from 1970 to 2010 (32) and another with data from 1978 to 1997 (30) showed decreasing rates, while the third report with data from 1997 to 2006 showed stable incidence rates (28).
Risk factors
Only a few of the studies in this review studied the effect of risk factors on TC incidence trends. Six reports investigated the association between exposure to ionizing radiation and TC (33 –38). These studies investigated incidence rates by time periods or geographic areas associated with increased exposure due to a nuclear reactor or accident. While three studies did not demonstrate an association (33 –35), three others did. One was a study from Belarus, close to the Chernobyl accident where incidence rates in children and adolescents has been shown to have increased following the nuclear disaster (36). The other two studies support an association between proximity to nuclear reactors or an exposure event from one of the nuclear reactors in the United States and the incidence of TC (37,38). Another study demonstrated a correlation between increasing TC incidence and increased iodine levels in the population over the years since iodine supplementation began (16).
Discussion
This systematic review found a trend of increasing incidence of TC, over the last 40 years in the majority of included countries. The commonest subtype, PTC, contributes the most to this increase in incidence. Few risk factors were studied and reported alongside changes in TC incidence. Exposure to ionizing radiation was the most common risk factor assessed. Several studies supported the association and others found no such link between ionizing radiation and TC.
The results of this study are in concordance with other reports in the literature. In one published analysis of the 1973–2002 Cancer In 5 Continents (CI5) data (39), Kilfoy et al. concluded that there had been a sustained, worldwide increase in TC incidence, which was neither restricted to particular areas nor influenced by underlying rates. This was with the exception of Africa, which reported a low incidence. This systematic review provides an update on incidence rates, and includes both studies based on cancer registry data and independent studies.
Another similar publication, based on GLOBOCAN data from 2002 and 2008, reported on the trends of TC incidence (40). The authors describe an increase in incidence in three-quarters of the countries studied. The focus of the GLOBOCAN report was on whether the characteristics of a healthcare system affected the incidence of TC. The authors used a statistical model to estimate the association of gross domestic product (GDP) and private health expenditure with TC incidence. They conclude that both GDP and the amount of private healthcare expenditure correlate with the incidence of TC, especially in females. GLOBOCAN is based on estimates of incidence rates, which are based on various methods, some of which may not provide reliable data. Examples of such methods include using rates from neighboring countries to estimate rates (33/184 countries), and estimating incidence from mortality rates using modeled survival (32/184 countries) (41). Another limitation of such database studies is the accuracy of the data. Each database consists of multiple data sources. Although there are minimum requirements for the standard of data they provide, data quality is liable to known risks such as case duplication, reporting delays, and misclassification or coding errors (42 –45). Furthermore, the cancer databases mentioned above do not provide incidence data stratified by disease subtype or associated risk factors, limiting further investigation into the cause of changing trends. Also, these databases may not include data from regions where no cancer registry has been established.
The primary cause for the increase in incidence is likely to be improvements in the identification and treatment of subclinical disease, which would not otherwise have progressed. This is supported by the results of this systematic review. PTC is the primary cause of the increase in the majority of studies that reported incidence for each subtype. A compelling argument in support of this hypothesis is the trend toward increasing detection of smaller tumors, as described in a number of reports in this review (6,46 –48). After many years of over-detection and treatment of small tumors, the number of large tumors would be expected to be in decline. However, a number of studies in the review highlight a concurrent increase in larger tumors (48 –50). One of these studies is a study from Spain that reported a significant increase in the proportion of both PTC micro- and non-microcarcinomas. The incidence of microcarcinomas increased from 16.7% in 1978 to 43% in 2001 (49). Of these, 91% were diagnosed incidentally following thyroid surgery for another cause. Another study from Tasmania also found that both micro-PTC and larger tumors have increased in number over a 20-year study period (48). Finally, the study from Canada presented the strongest evidence in support of the increase in larger tumors (7). The authors reported a non-significant change in the proportion of TCs ≤1 cm (microcarcinomas), and reported increasing numbers and relative proportions of the largest tumors (>4 cm). The rising numbers of larger tumors in these studies supports the probability of a true increase contributing to the increased incidence.
Another argument supporting the hypothesis of over-diagnosis is stable mortality rates (6). If incidence has increased due to advanced disease, it is highly unlikely for improvements in survival to have matched this increase so closely as to produce stable mortality rates. It is more likely that the increase in incidence is attributed largely to detection of subclinical disease that would not affect life expectancy. A study (8) challenging the above argument (6) reported slightly increased survival rates (for all TC combined), which was in line with a shift in the distribution of TC subtypes from FTC to PTC (8). The authors ascribe this to the better prognosis of PTC compared with FTC, but argue that there should be an even greater improvement in survival rates if subclinical disease is responsible for increased incidence rates (8). The heterogeneity of measures used to describe mortality and survival in the various studies makes comparison and generation of pooled measures difficult.
The factors underlying over-detection may be described in three categories: increased diagnostic imaging, increased rates of thyroid surgery, and increased scrutiny of histopathology specimens. First, increased use of and advances in imaging technology has resulted in an increased ability to detect incidental thyroid lesions. Examples include cross-sectional imaging of the head and neck for thyroid and non-thyroid diseases (51) and functional radio-isotope imaging used in cancer staging and rheumatological diseases (52,53). Second, the number of thyroid operations for benign diseases has increased (54). Autopsy studies have demonstrated high rates of incidental TC in the normal population. Thyroid specimens following surgery for benign disease are therefore likely to reveal incidental cancers. This will increase incidence rates, but not affect the prognosis of the individual patient. In addition to the increase in thyroid operations, the scrutiny with which specimens are assessed varies between centers and may have increased over time, contributing to over-detection (5).
As mentioned above, the prevalence of TC in autopsy series is high and ranges from 0.01% to 35.6% (55). Another interesting observation is the striking sex disparity in TC incidence. In all of the studies included in this review, there is a much higher rate in women than men, with a ratio of around 3:1. This difference has been a major impetus for research into the role of hormonal and reproductive factors in the etiology of TC. Studies have so far failed to demonstrate a strong association (10,56 –59). The sex distribution in autopsy series is, however, 1:1, with some studies reporting higher rates in males (60). It is therefore suggested that the apparent higher incidence of TC in women may be artefactual and primarily due to over-detection. If this is artefactual, this may be attributed to the increased risk of autoimmune thyroid disease in women (61) and increased contact with healthcare in women (62). This hypothesis is supported by the better prognosis of TC in females (63,64), perhaps a result of more subclinical disease being detected and treated in women.
Despite the evidence for over-detection being the main cause for rising TC incidence, there may also be a true increase in incidence, at least in some regions. The cause of this real increase is, however, unclear. Exposure to ionizing radiation is the most likely “candidate” risk factor accounting for this. A study in a Belarusian population (residing close to Chernobyl) showed the highest increase in TC incidence in the young (36). Other literature supporting the risks associated with nuclear disasters/weapons include other studies from Chernobyl, the nuclear bomb detonations in Japan, and the Three Mile Island nuclear meltdown in the United States (11,38,65). However, some other studies did not demonstrate such associations with radiation exposure from nuclear accidents (35,37).
More evidence for ionizing radiation as a risk factor for TC includes case-controlled studies in children who underwent ionizing radiotherapy treatment for benign conditions such as tinea capitis in the past (66). There appears to be a strong inverse relationship between age at exposure to radiation and risk of TC (67). A recent retrospective cohort study investigating exposure to diagnostic radiography and TC reported an increased risk of papillary microcarcinoma with increased imaging exposure in adults (67). However, multiple methodological limitations in this study limited the strength of the authors' conclusions (68).
A dose–response relationship between radiation and TC has been demonstrated previously. PTC has the strongest association with ionizing radiation (66). As demonstrated above, PTC appears to account for the majority of rising incidence trends.
The United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) estimated a worldwide average total exposure of 3.01 mSv per person per year (12). This report emphasized that medical diagnostic imaging makes up a significant proportion of exposure, and has increased significantly since the 1980s, probably related to the increased availability and reduced cost of imaging.
Other proposed risk factors explored in the literature include female reproductive factors (58), iodine deficiency and or supplementation (69), exposure to a volcanic environment (70), lifestyle factors (71), and diet (72). However, available evidence is limited, of poor quality, and variable, making it difficult to attribute specific risk factors to the changes in reported TC incidence.
Future research should focus on comparing the diagnostic approach to TC in different regions and the effect this has on incidence rates. More data are also needed from developing countries, where incidence rates are largely unknown. A validated framework for reporting on epidemiological data would allow for direct comparison and meta-analysis. For example, if each study reported using the world standard population, as well as their own standardization, rates could be more accurately compared. Further work on the risk factors associated with TC is also warranted, given that the reason for increased “true” incidence is unknown.
Conclusions
This systematic review is an up-to-date synthesis of the literature, and demonstrates widespread and sustained increase in TC incidence. The increase appears to continue into the most recent reports from 2014. Overall, there is substantial evidence to support the hypothesis of increased detection of subclinical disease accounting for the increase in incidence. Additionally, a concurrent small but real increase is proposed, at least in some regions.
Increasing exposure to ionizing radiation may be more likely than any other identified factor to be contributing to any real increase in incidence rates. The magnitude of the effect is, however, unclear.
The sex disparity in incidence of detected TC may be artefactual and not reflected in autopsy series. This suggests that the problem of over-detection disproportionally occurs in women, which warrants further investigation.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to disclose.