
Abstract
Background:
Several screening studies have indicated an increased prevalence of celiac disease (CD) among individuals with autoimmune thyroid disease (ATD), but estimates have varied substantially.
Objective:
The aim of this study was to examine the prevalence of CD in patients with ATD.
Method:
A systematic review was conducted of articles published in PubMed Medline or EMBASE until September 2015. Non-English papers with English-language abstracts were also included, as were research abstracts without full text available when relevant data were included in the abstract. Search terms included “celiac disease” combined with “hypothyroidism” or “hyperthyroidism” or “thyroid disease.” Fixed-effects inverse variance-weighted models were used. Meta-regression was used to examine heterogeneity in subgroups.
Results:
A pooled analysis, based on 6024 ATD patients, found a prevalence of biopsy-confirmed CD of 1.6% [confidence interval (CI) 1.3–1.9%]. Heterogeneity was large (I2 = 70.7%). The prevalence was higher in children with ATD (6.2% [CI 4.0–8.4%]) than it was in adults (2.7%) or in studies examining both adults and children (1.0%). CD was also more prevalent in hyperthyroidism (2.6% [CI 0.7–4.4%]) than it was in hypothyroidism (1.4% [CI 1.0–1.9%]).
Conclusions:
About 1/62 patients with ATD have biopsy-verified CD. It is argued that patients with ATD should be screened for CD, given this increased prevalence.
Introduction
C
The disease entity autoimmune thyroid disease (ATD) used in the majority of studies explored in this paper consists of two very different disorders (3). Autoimmune thyroiditis or Hashimoto's disease is a destructive autoimmune disorder with T-cells targeting the enzyme thyroperoxidase causing injury to the thyroid gland, which is often permanent. Autoantibodies against thyroperoxidase are clinically very useful, whereas autoantibodies against thyroglobulin have low specificity and are of little value. Graves’ disease is a non-destructive disease directly caused by autoantibodies binding to and stimulating the thyrotropin (TSH) receptor (4). Autoimmune thyroiditis and Graves’ disease probably have different etiologies, and while TSH receptor autoantibodies in pregnant women transferred over the placenta will cause neonatal thyrotoxicosis in the fetus, thyroperoxidase autoantibodies have no effect at all on the fetus. Autoimmune thyroiditis occurs in high frequency in patients treated with alpha interferons, for example patients with hepatitis C (5), and reports of CD induced by interferon alpha therapy have also occurred (6), suggesting common etiological mechanisms shared between autoimmune thyroiditis and CD.
In a registry-based study, CD was linked to both hypo- and hyperthyroidism (7). In this study, the odds ratios (ORs) for future CD were increased in both hypothyroidism (OR = 3.8) and hyperthyroidism (OR = 2.0). The prevalence of CD in patients with ATD has varied substantially. When Fanciulli et al. screened 231 individuals with ATD, none had CD (0%) (8). Meanwhile, a recent U.S. report found a CD prevalence of 9.9% (9).
The aim of this study was to examine the prevalence of CD in patients with ATD. It was hypothesized that CD would be more prevalent in ATD than the 1% prevalence reported in most screening studies of the general population. In sub-analyses, the aim was also to examine the prevalence of CD according to the characteristics of the ATD patients.
Methods
Search
PubMed and EMBASE were searched for papers indexed with CD and “hypothyroidism,” “hyperthyroidism,” or “thyroid disease” until December 1, 2014 (root words were used as well as MESH terms). The initial search was performed by librarians at the Karolinska Institutet Library, Sweden. Publications in all languages were included, but the manual review was restricted to papers with an English-language abstract. In all, 1899 publications were identified (PubMed: n = 514; EMBASE: n = 1385). After removing duplicates, there remained 1527 unique publications, of which 1490 were excluded based on title and abstract screening.
The current study has no review registration number and has not been registered in any database.
Study selection
All potential studies were screened by M.L. and A.R., with J.F.L. verifying key data, including all data on CD prevalence. Disagreements were resolved through consensus. Thirty-seven papers were read in detail, and 11 were excluded for the following reasons: two studies were duplicates and reported the same data as separate publications (10,11); three studies were not primarily aimed at assessing the association between CD and ATD (12 –14); two studies focused on patients with non-ATD, including thyroid agenesis/hemiagenesis, or positive antithyroid antibodies of unclear clinical significance (15,16); one study focused on patients with a “risk” of CD based on antibodies without any further diagnostic evaluation (17); in two studies, diagnosed CD was based only on patient reports/surveys rather than on serologic or histologic criteria (18,19); and one study was excluded because it was based on a sample with high suspicion for selection bias (20). After an initial peer review, one more relevant paper was identified and included (21). In the end, 27 studies were hence entered into the meta-analysis (Table 1) (8,9,11,21 –44).
Histopathology stages: M1, Marsh 1; M2, Marsh 2; M3, Marsh 3.
ATD, autoimmune thyroid disease; CD, celiac disease; Hyper, hyperthyroidism; Hypo, hypothyroidism; AGA, antigliadin antibodies; EMA, endomysial antibodies; PMID, PubMed ID; TTG, tissue transglutaminase antibodies.
One of these studies (11) is presented divided by hypo- versus hyperthyroidism. In September 2015, the search was performed again starting from December 1, 2014 (PubMed: n = 16; and EMBASE: n = 93), but none of these papers was relevant to this meta-analysis.
None of the authors were contacted. Confidence intervals (CIs) were calculated anew for the proportion of individuals with CD in ATD. Wald estimates were used for CIs, except for the study by Fanciulli et al. (8) where exact CIs were used.
Data items and risk of bias
Information was retrieved on type of ATD (hypothyroidism, hyperthyroidism, and mixed), year of publication, country, proportion of antibody-positive individuals who underwent small intestinal biopsy, and whether the authors required villous atrophy (Marsh III) (45) for the CD diagnosis. When only a few individuals with positive celiac antibodies (endomysial antibodies [EMA], antigliadin antibodies [AGA], or tissue transglutaminase [TTG]) undergo biopsy, this will automatically decrease the prevalence of biopsy-verified CD (as opposed to when everyone with a positive celiac serology has a biopsy). Similarly, stringent histopathology criteria (Marsh III) is likely to decrease the prevalence of CD (46).
Where possible, studies were categorized according to the age of those screened. Specifically, studies were looked at where TTG, AGA, or EMA were used for the initial screening of CD in ATD. Studies were not graded according to study quality, but instead a choice was made to discuss various elements of quality in the discussion.
Summary measures, analysis method, and heterogeneity
First, a funnel plot was carried out (Fig. 1). The funnel plot suggested the existence of publication bias where smaller studies seem more likely to be published if they show high prevalence rates for CD. Therefore, a fixed-effects model was chosen when conducting the meta-analysis of the prevalence of CD in ATD, since a random-effect model assigns undue weight to the smallest studies. The authors have previously used fixed-effects models in such circumstances (47). Heterogeneity was calculated using I2. To examine heterogeneity, a number of sub-analyses were performed. The study explored if the prevalence of CD in ATD was influenced by: continent (Europe vs. other, but also excluding all Italian studies, since they made up 50% of all relevant studies) (8,9,11,20,25 –34), age (children, adults, both), proportion of serologically positive individuals undergoing small intestinal biopsy (≤90% [or unspecified] vs. >90%), and proportion of females (≤84% vs. ≥85%).
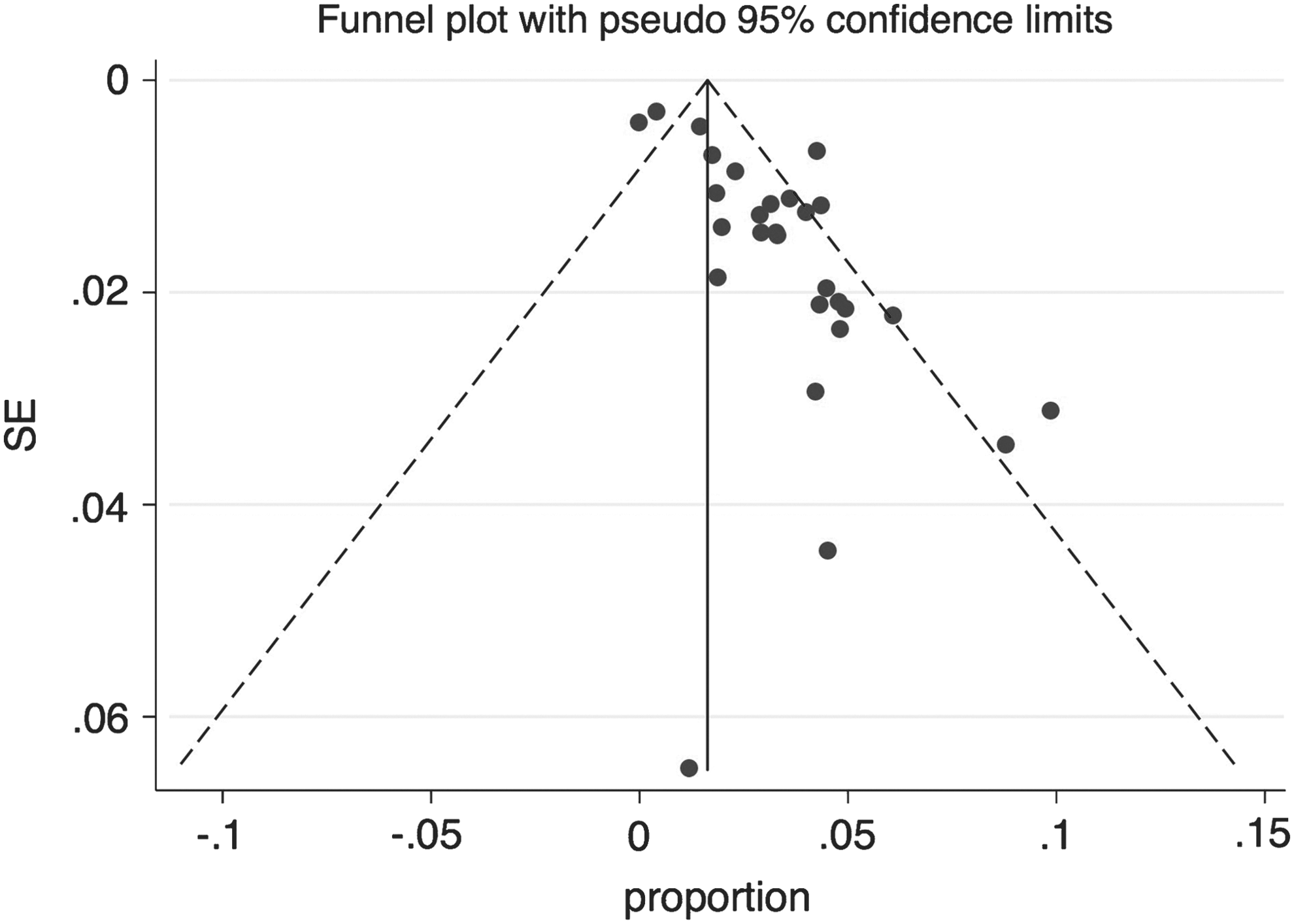
Funnel plot of included studies.
Furthermore, the linear relationship between the prevalence of CD in ATD and the prevalence of CD in the general population were studied. The underlying general-population prevalence of CD in the countries contributing ATD data in this study varied between 0.25% and 2%, and, where possible, the prevalence of biopsy-verified CD in the general population was calculated based on the following studies (2,48 –56). Italian and British prevalence data of CD were based on the so-called “prevalence B criteria” in the multi-European screening study by Mustalahti et al. (2).
Meta-regression is a regression-based statistical procedure used in meta-analyses to assess the impact of covariates at the level of the studies on study effect size. Meta-regressions were used to examine if the following factors influenced the prevalence of CD in ATD: age at CD testing, proportion of women with ATD, proportion of serologically positive patients with ATD who underwent biopsy, GDP per capita, year of publication, and study size (number of study participants). In the meta-regression of proportion of serologically positive patients with ATD undergoing biopsy, the study by Fanciulli et al. (8) was excluded, since no patient in that study was serologically positive (and hence it was not possible to calculate the proportion undergoing biopsy). The decision was made to analyze one factor at a time in the meta-regressions in order to increase the understanding of underlying study characteristics.
While earlier research from Sweden has found no association between socioeconomic status (as a proxy for high income) and CD (57), data from other countries have shown socioeconomic gradients in the risk of CD (58). The relationship with GDP per capita and CD was therefore explored using GDP data from the International Monetary Fund from 2014 (
In the current meta-analysis, individuals with Marsh I histology were included in the diagnosis of CD (when histopathology grade was reported), but a sensitivity analysis was carried out with studies requiring Marsh III.
Stata v13 was used for all analyses. As none of the study participants were contacted, informed consent was not obtained.
Results
Background data
Twenty-seven relevant studies were identified, including 6024 individuals with ATD. Six of these studies had screened <100 patients with ATD (9,11,23,24,32,37). The prevalence of CD ranged between 0% and 10% (Table 1). The median prevalence of CD in ATD was 3.2%.
Prevalence of CD in ATD patients
Pooling data, a prevalence of CD in patients with ATD of 1.6% was found ([CI 1.3–1.9%]; Fig. 2). The heterogeneity was, however, high (I2 = 70.7%). To examine this heterogeneity further, a number of sub-analyses were conducted.
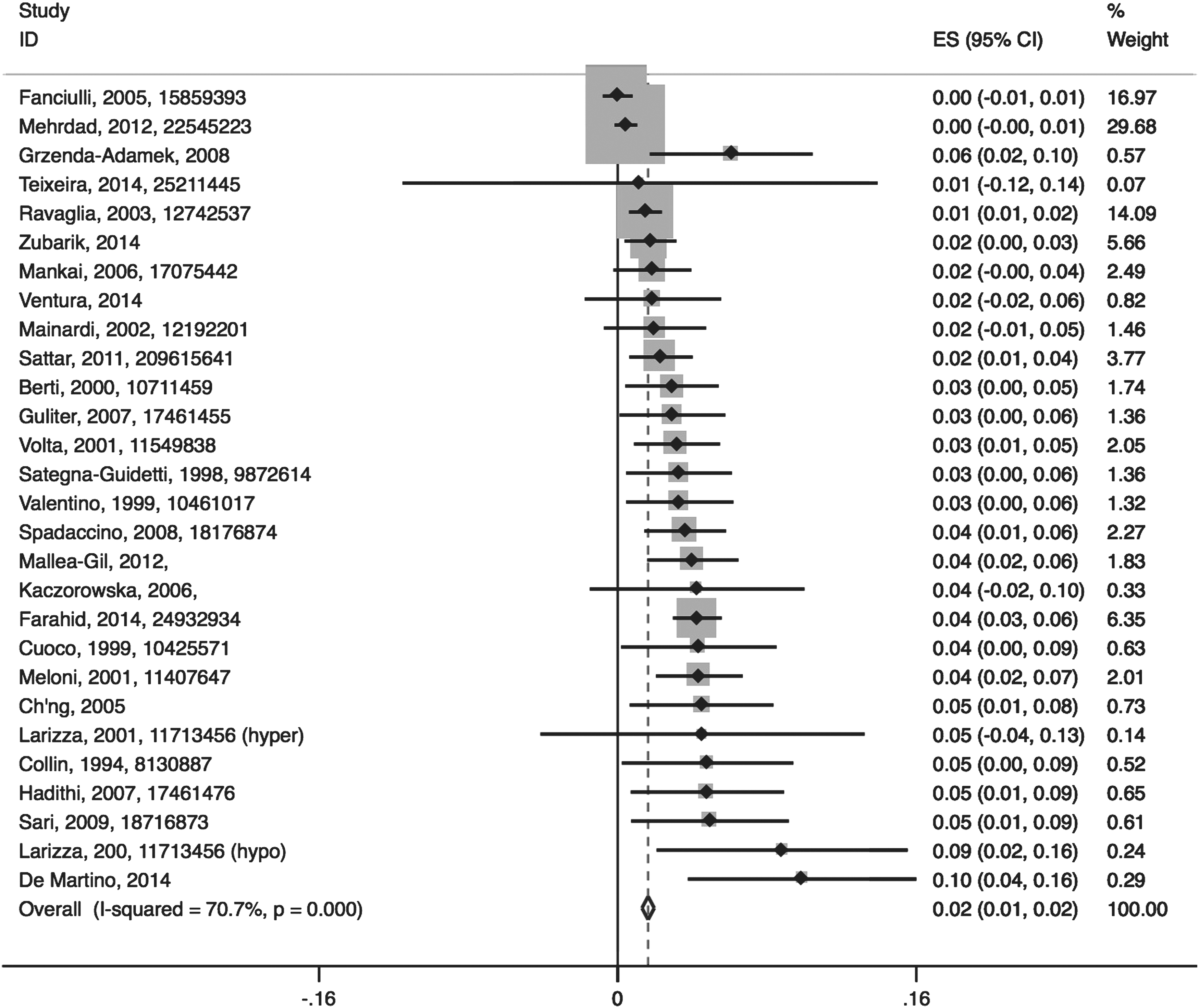
Prevalence of biopsy-verified celiac disease (CD) in autoimmune thyroid disease. Study names with first author, year of publication and PMID number (where available). The confidence intervals (CI) of this figure were based on ±1.96*Standard errors. They were recalculated by the authors, and only used to assign weight to individual studies. For this reason, the lower CI may be negative (<0).
Type of ATD
The prevalence of CD was slightly higher in hyperthyroidism (2.6% [CI 0.7–4.4]) (11,39,42) and in mixed populations (1.7% [CI 1.2–2.2]) (8,9,20 –24,26 –28,31 –34,37,38,40,43) than among individuals with hypothyroidism (1.4% [CI 1.0–1.9]) (11,19,25,29,30,35,36,41,44).
Age
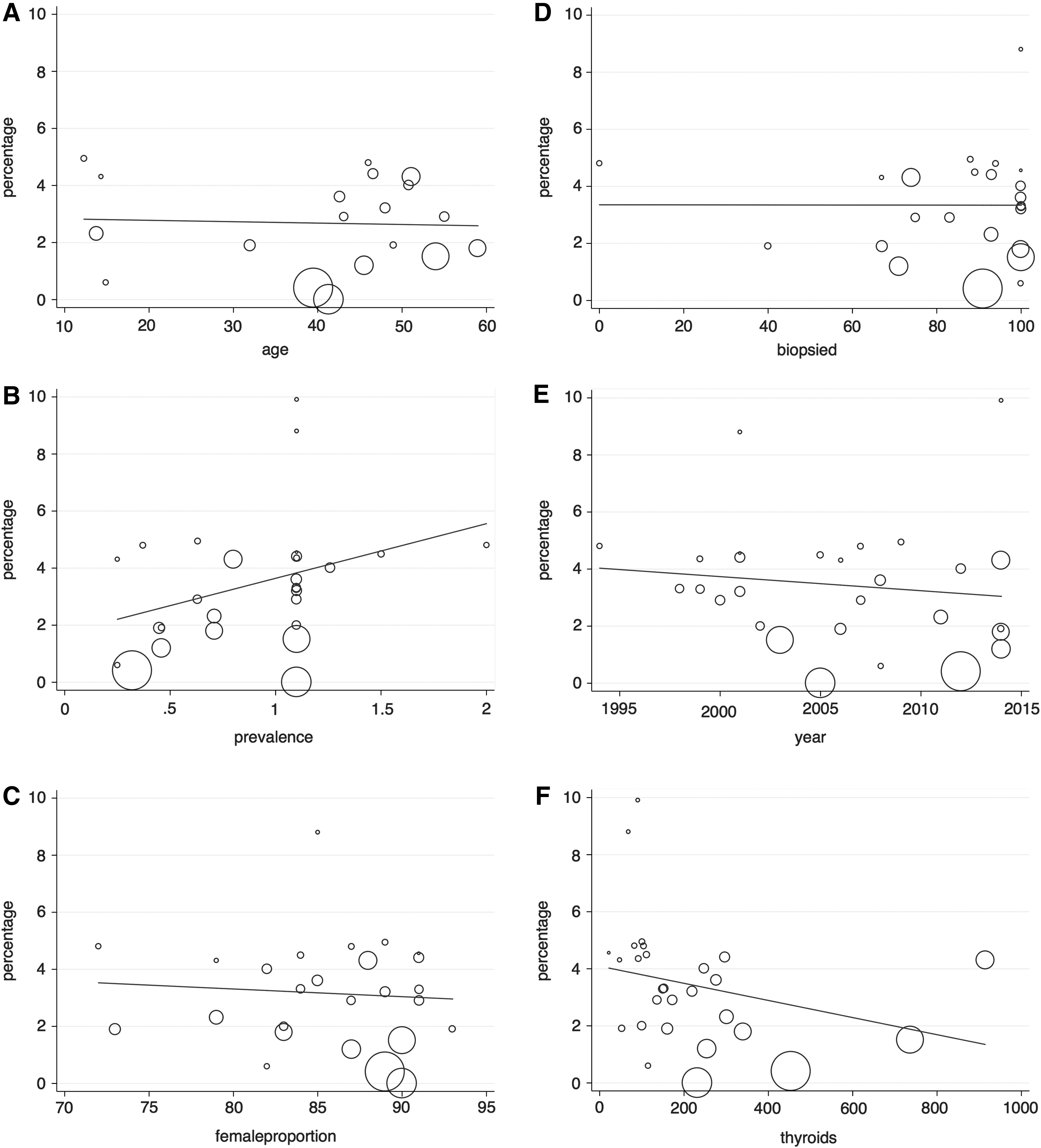
The prevalence was higher in children with ATD (6.2% [CI 4.0–8.4%]) (9,11,37,38,41) than in adults (2.7% [CI 2.1–3.4]) (19,21,22,24,27,29,34 –36,40,42,44) or in studies examining both adults and children (1.0% [CI 0.6–1.4]) (8,23,25,26,28,30,31,33,39,43). The highest pooled prevalence was, however, seen in one study where the age of participants was unclear (9.0% [CI 5.3–12.8%]) (32). Figure 3A shows that there was no relationship between age at testing for CD and CD prevalence in ATD.
Prevalence of CD in the general population
There was no difference in the prevalence of CD between countries in Europe and elsewhere (data not shown). In a sensitivity analysis, the data were restricted to studies outside Italy (given the large number of included studies from Italy), but prevalence was similar in Italy and elsewhere (data not shown). The meta-regression suggested a positive association between the prevalence of CD in the general population and the prevalence of CD in patients with ATD, but the results were not statistically significant (p = 0.065; Fig. 3B).
Sex
In this meta-analysis, the prevalence of CD was slightly lower in studies with a higher proportion of females (1.3% [CI 1.0–1.7]) than in studies with a higher proportion of males (2.6% [CI 1.8–3.4]); the highest prevalence was seen in those studies that did not report the sex of their patients (6.1% [CI 2.7–9.6]). However, the difference in CD prevalence between studies with more females and studies with more males was not statistically significant, as the meta-regression found no association between proportion of females and CD prevalence (Fig. 3C).
Biopsy data and Marsh III
Fifteen studies required Marsh III for the CD diagnosis (11,21,23,25 –30,33,36,38,39,41,42). The prevalence of CD in these studies was 1.4% [CI 1.0–1.8%]. In 13 studies, at least 90% of those with positive celiac serology had undergone small intestinal biopsy (11,22,25,26,28 –31,33,36,38,43,44), and the pooled prevalence of CD in these studies was 1.6% [CI 1.3–2.0%]. A meta-regression showed no association between the proportion of antibody-positive individuals undergoing biopsy and CD prevalence in ATD (Fig. 3D).
Other potential factors
No links were found between GDP per capita (Supplementary Fig. S1; Supplementary Data are available at
Discussion
The current meta-analysis is based on >6000 individuals with ATD, and a CD prevalence of 1.6% was found. Despite performing a number of sub-analyses, it was not possible to explain the high heterogeneity between studies.
CD has previously been linked to a number of autoimmune disorders, including type 1 diabetes (59), Addison's disease (60), IgA nephropathy (61), and pernicious anemia (62). In 2008, Elfström et al. reported a two- to fourfold increased risk of ATD in patients with CD (7), and similarly that CD was more common in patients with ATD. A number of studies also report that thyroid-related antibodies are more frequent in CD (63).
The current study examined the prevalence of CD in ATD. Assuming that the CD prevalence in the general population in the countries contributing data to this study (Fig. 2B) was about 1%, roughly a 1.6-fold increased risk of CD in ATD is demonstrate. This is lower than expected, considering an earlier registry-based study (7), and lower than the median prevalence (3.2%) of the included studies in this meta-analysis. Perhaps this low prevalence can be explained by several limitations of the studies that were examined. Many of the studies included in the analysis incorporated the older AGA into their serologic screening protocols. It is now well-established that AGA has a low positive-predictive value, even in high-risk groups (64), and its use as a screening test may have led to an underestimation of the prevalence of CD in ATD. Complicating this problem is the fact that several of the studies included in this meta-analysis did not uniformly perform intestinal biopsies for patients with positive serologies—automatically lowering the prevalence of biopsy-verified CD. Lastly, ATD patients with positive serologies but normal intestinal biopsies were not routinely followed. A proportion of these patients may have so-called “potential CD” (1), and their diagnosis would only have been made with long-term serologic and histologic follow-up (65). Future studies aimed at determining the true prevalence of CD in ATD should focus on large-scale screening of patients with ATD using standard follow-up and a sequential screening strategy incorporating highly sensitive and specific serologic tests (TTG and EMA) and histologic evaluation that increase the positive-predictive value of screening (66). Despite the possibility that this study underestimates the prevalence of CD in ATD, the finding that 1/62 tested individuals were positive for CD leads us to argue that patients with ATD merit screening for CD. This recommendation is in line with recent reviews on the topic (67 –70).
Although some minor differences in CD prevalence were identified in subgroups, none of these were statistically significant. Neither were any linear relationships found between CD prevalence and the seven independent factors tested for in the meta-regressions. In an earlier meta-analysis of CD in T1D, age at testing for CD was a risk factor for high prevalence of CD (59). It is hypothesized that this could be due to more intense autoimmunity in those with early onset of autoimmune disease, a finding that could not be replicated in this study.
Strengths and weaknesses
The literature search was based on both PubMed and EMBASE. As can be seen from the Methods section, the EMBASE search yielded a large number of hits, including abstracts that would have been missed had we only relied on one data source. The PRISMA guidelines (71) were followed when carrying out this meta-analysis, and two authors (M.L. and A.R.) reviewed all abstracts independently of each other. In the end, 27 papers were included totaling >6000 patients. This resulted in a narrow CI [CI 1.3–1.9%].
Among the weaknesses of the study is the lack of full-text information on a small number of studies, although this does not seem to have influenced the CD prevalence in ATD. Furthermore, some studies were not explicit on their criteria for a biopsy-verified CD, and others failed to describe the kind of serology test they had used to identify individuals at risk of CD. Finally, some of this information might have been obtained had the authors been contacted, but from experience, it is known that the response rate is low from authors publishing in non-English journals (the majority of studies without available full text).
Clinical implications
The importance of recognizing CD in a timely fashion cannot be understated. Although the prevalence of CD has increased fourfold in countries including the United States over the last 50 years (72), population based-studies suggest that only a small proportion of CD cases are clinically recognized—just 21% in a recent European study employing mass serologic screening (2). The potential health risks of unrecognized CD are multifold. In addition to the nutritional deficiencies (including iron, vitamin B12, folate, copper, and zinc), bone disease (osteopenia and osteoporosis), and reproductive disorders (including preterm birth and intrauterine growth restriction) associated with undiagnosed CD, there appears to be a direct correlation between gluten exposure and the incidence of autoimmune disorders and lymphoproliferative malignancy in patients with CD (73 –78). To what extent this is also true for asymptomatic CD (found through antibody screening) is still a matter of debate (70), as studies on quality of life (and whether it improves on a gluten-free diet) in screen-detected CD have been contradictory (76,79,80). Of special relevance to this study is whether treatment of undiagnosed CD in ATD can influence the course of ATD. Berti et al. have suggested that patients with both ATD and CD are more likely to develop other autoimmune diseases than those with only ATD (27). If that trajectory (toward more autoimmunity) could be influenced by a gluten-free diet is, however, unclear. A French research group reported that the risk of autoimmune disease in patients with CD was positively linked to dietary adherence, but this association disappeared when adjusting for confounders (p = 0.07) (75). While Ventura et al. reported that thyroid-related antibodies decreased in patients on a gluten-free diet (63), no such development was seen in the study by Berti et al. (34). One explanation for the diverging results is a lack of power and wide CIs. Another may be multiple testing leading to a type 1 error. Institution of a gluten-free diet will, however, increase the chances of mucosal healing. Considering that CD and other malabsorptive conditions are the most common cause of treatment-refractory hypothyroidism (81), this is likely to benefit the absorption of drugs used in ATD (e.g., levothyroxine). To what extent diagnosed CD may influence the prognosis of ATD is not known.
Based on the 1.6% incidence of CD in ATD found in this meta-analysis, the author support instituting screening for CD in this high-risk population. While a cost-effectiveness analysis of such a strategy is beyond the scope of this study, previous literature does shed some light on this subject. Two recent analyses have found that mass screening for CD is cost-effective, as the cost for each quality-adjusted life year (QALY) gained through CD screening is less than the generally accepted threshold of US$ 0,000/QALY (82,83). Although the findings from these studies must be interpreted based on various assumptions entered into the cost-effectiveness models for screening the general population (including the somewhat controversial mortality risk estimates between diagnosed and undiagnosed CD patients), both studies acknowledge that the cost-effectiveness of CD screening will be more pronounced in high-risk populations with a greater prevalence of CD. This meta-analysis is the largest scale study that demonstrates that patients with ATD fit this high-risk criterion with a 1.6-fold increased risk of CD compared with the general population. For a sense of how significant CD prevalence is to the cost-effectiveness of a screening strategy, we look to a sensitivity analysis comparing EMA-based screening to no-screening when the base case prevalence of CD was increased from 0.5% to 1% in the study by Shamir et al. (83). This change resulted in a decrease in the incremental cost-effectiveness ratio from US$44,941 to US$23,211, and one would expect an even more dramatic increase in cost-effectiveness if the prevalence were to be further increased to the 1.6% seen with ATD.
Taking a step back from mass screening, there is also strong evidence to support intestinal biopsies for CD in ATD patients undergoing upper endoscopy. A recent study assuming a 1% prevalence of CD in a cohort with gastroesophageal reflux disease (GERD) showed that routine duodenal biopsy analysis for CD during endoscopy for GERD is not cost-effective (with a cost of US$55,692/case of CD detected and US$121,875/QALY gained). However, the incremental cost-effectiveness ratio for the biopsy strategy met the target of <US$50,000/QALY when the prevalence of CD in patients with refractory GERD was >1.8%—very similar to the prevalence of CD in ATD that we find in this meta-analysis (84). While these data do not necessarily answer the question of generalized screening for CD in the ATD population, they at the very least support routine duodenal biopsies for the evaluation of CD when patients with ATD are undergoing upper endoscopy for any indication. Overall, while the difficulties of instituting and maintaining a gluten-free diet in asymptomatic, screen-detected individuals is acknowledged, CD screening in ATD is warranted based on preventing the significant morbidities (both thyroid-disease related and otherwise) and mortality associated with undiagnosed CD.
In conclusion, CD was found in 1/62 patients with ATD. It is argued that patients with ATD should be screened for CD given this increased prevalence.
Footnotes
Acknowledgments
J.F.L. was supported by grants from The Swedish Society of Medicine, the Swedish Research Council—Medicine (522-2A09-195), and the Swedish Celiac Society.
None of the funders had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Author Disclosure Statement
The authors have nothing to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.