
Abstract
Background:
The use of thyrotropin and free thyroid hormone assays to evaluate thyroid function is widespread, but in some situations the results are inconsistent with the patient's thyroid status.
Summary:
A 35-year-old woman with a known diagnosis of chronic autoimmune thyroiditis was referred to the authors' clinic at week 26 of her second pregnancy. The patient was clinically euthyroid. Consistent with this, her serum thyrotropin (TSH) was normal (0.79 mIU/L), but she had elevated free thyroid hormones—free triiodothyronine (fT3) and free thyroxine (fT4)—as determined by a one-step chemiluminescent assay. The patient was taking levothyroxine replacement therapy (125 μg/day), and the dose was confirmed. Previous blood tests showed concordance between TSH and free thyroid hormone values. The patient was followed up throughout gestation and at 12 months postpartum. During gestation, her free thyroid hormones remained high using one-step methods, while the total thyroid hormone concentration values were within the reference range, in agreement with the TSH values. Postpartum fT4 and fT3 values returned progressively to normality, in agreement with the TSH values. The presence of circulating thyroid hormone autoantibodies (THAb) was hypothesized, which are known to interfere, although to a variable extent, with thyroid hormone one-step assays. Using stored frozen sera, this hypothesis was confirmed indirectly by measuring normal levels of fT3 and fT4 with a two-step method, and directly by demonstrating THAb against the two hormones.
Conclusion:
Despite their relative rarity, circulating THAb may be suspected when laboratory data are not consistent and contrast with the clinical picture. To the authors' knowledge, no previous case of transient appearance of THAb in pregnancy has been described.
Introduction
T
Abnormality in thyroid function tests can occur in patients with physiological or pathological conditions: altered thyroid hormone serum binding proteins (thyroxine binding globulin, albumin, transthyretin) (3); drug interferences (among others, iodine-containing medications, thionamides, thyroxine, steroids, propranolol, and antiepileptic drugs) (4 –6); resistance to thyroid hormones (7); thyrotropin (TSH)-secreting pituitary adenoma (8); nonthyroidal illness (9); and assay interference. The latter can be caused by the presence of heterophilic antibodies that can bind the assay antibody (10); thyroid hormone autoantibodies (THAb), which can bind the tracer (11); variant thyroid hormone binding proteins with altered affinity for thyroxine (T4) (12); heparin that can displace T4 and triiodothyronine (T3) from their carrier proteins (13); or biotin, which can interfere with several immunoassays (14). A more detailed discussion, particularly on THAb, is available elsewhere (15 –26).
Here, the sudden appearance of THAb during the second part of gestation in a woman with autoimmune thyroiditis who was taking levothyroxine is described.
Methods
Biochemical evaluation was performed on serum obtained after an overnight fast. TSH, free T4 (fT4), and free T3 (fT3) were measured using a commercial one-step chemiluminescent assay (ECLIA Roche) and/or a two-step chemiluminescent assay (Architect; see below). The reference ranges for TSH, fT4, and fT3 are 0.27–4.2 mIU/L, 9.3–17.0 pg/mL, and 1.8–4.6 pg/ml (ECLIA Roche), and 0.4–4.0 mIU/L, 7–14.8 pg/mL, and 1.71–3.71 pg/mL (Architect). Total thyroid hormones were measured with a two-step chemiluminescent assay (Architect), the reference ranges being 4.5–12 μg/dL (T4) and 80–180 ng/dL (T3). Antithyroid peroxidase antibodies (TPOAb) were measured by enzyme-linked immunosorbent assay, and anti-TSH receptor antibodies (TRAb) were measured with a radio-receptor assay.
Serum THAbs were assayed by the radioimmunoprecipation technique described previously in other studies (11,18,19), using antihuman IgM or antihuman IgG serum (Sigma-Aldrich) and [125I]T3 or [125I]T4 (Johnson & Johnson). IgMT3, IgGT3, IgMT4, and IgGT4 are expressed as % bound/total, and the cutoff for positivity is considered >3.9, >3.6, >3.4, and >3.9%, respectively. Internal controls for negative tests (sera negative for all four THAbs) and positive tests (sera positive for T3IgM only, T3IgG only, T4IgM only, or T4IgG only) were assayed for THAb together with the patient's sera, and their corresponding THAb status was confirmed. The authors had shown previously (20,21) that searching THAb in the isolated immunoglobulin fraction of serum does not increase sensitivity compared with a THAb search in serum per se.
Rheumatoid factor, total IgG, total IgA, and total IgM were measured with the Beckman ICS-II turbidimetric method (reference ranges <37 IU/mL, 650–1600 mg/dL, 70–400 mg/dL, and 40–230 mg/dL, respectively). Antinuclear antibodies (ANA), antimitochondrial antibodies (AMA), anti-smooth muscle antibody (ASMA), and antiparietal cells antibodies (PCA) were measured by indirect immunofluorescence (normal value title <1:80).
The patient provided written consent for publication of the case report.
Case Report
A 35-year-old woman was referred to the authors' clinic at week 26 of her second pregnancy. The reason for referral was a significant elevation of both serum fT3 (fourfold) and fT4 (threefold) with a drop in serum TSH in the lower part of the reference range compared with eight weeks earlier. The patient was taking 125 μg of levothyroxine daily but no other drugs or vitamin supplements. Five years prior to the observation, she received a diagnosis of chronic autoimmune thyroiditis. She reported a normal pregnancy, during which she was taking levothyroxine, and natural childbirth about two years before the observation. Except for that, her past medical history was unremarkable. Her family history revealed that her sister has chronic thyroiditis, presumably of autoimmune origin, but she has not been pregnant so far.
At the initial visit, the patient was clinically euthyroid (subjective and objective well-being, normal heart rate), in agreement with her TSH level of 0.79 mIU/L but at odds with the aforementioned elevation of both fT3 (13.2 pg/mL; reference range 1.8–4.6 pg/mL) and fT4 (65.6 pg/mL; reference range 9.3–17.0 pg/mL), as determined by a one-step chemiluminescent assay (ECLIA Roche). The assay was repeated in two different laboratories using the same method with consistent results (Table 1). Previously, at week 18 of gestation and using the same assay kits, TSH (3.14 mIU/L) and free thyroid hormone values (fT4 11.1 pg/mL; fT3 2.24 pg/mL) were normal and congruent. Retrospectively, the slight elevation of TSH compared to the 2nd trimester target level of 3.0 mIU/L, prompted an increase of the daily dose of levothyroxine from 100 to 125 μg/day. Antithyroid peroxidase antibodies (TPOAb) and anti-TSH receptor antibodies (TRAb) were undetectable (data not shown). Based on the clinical findings and the TSH value, the current levothyroxine treatment was found to be appropriate.
The numbers in square brackets indicate the reference range of the hormone. Serum levels of fT4 or fT3 that were above the upper normal limit are highlighted in bold.
TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; LT4, levothyroxine; NA, not applicable.
The patient was followed up at 12 months postpartum (Table 1 and Fig. 1). Free thyroid hormones were constantly elevated (in two controls, up to 34 weeks of gestation) using a one-step method (ECLIA Roche). However, the values of total thyroid hormones recorded at week 26s and 30 of gestation (T4 = 8.8 and 8.2 μg/dL; T3 = 114 and 101 ng/dL) were in agreement with the TSH values (1.4 and 1.5 mIU/L). At gestational week 40, she delivered a healthy boy. Subsequently, her fT4 and fT3 values returned progressively to the reference range and became congruent with the TSH value (Table 1 and Fig. 1).

Free thyroid hormones measured with a one-step method, thyrotropin, and corresponding levothyroxine treatment. Normal values of free triiodothyronine and free thyroxine are indicated by the two solid bars on the corresponding vertical axes.
Based on history and clinical status, pathological conditions (resistance to thyroid hormones, TSH-secreting pituitary adenoma, and nonthyroidal illness) were excluded. Pharmacological interference, particularly biotin consumption, which can interfere with a subset of immunoassays (14) was excluded; the patient took only levothyroxine during the entire pregnancy. Instead, interference in the free thyroid hormone assays was suspected. The presence of familial dysalbuminaemic hyperthyroxinaemia (FDH) or transthyretin-associated hyperthyroxinemia was ruled out for three reasons: the absence of a familial history, the normal values of total thyroid hormones, and the sudden increase of the free thyroid hormone concentrations. Therefore, an acquired artifactual condition, such as the presence of THAb or heterophilic antibodies, was hypothesized. Indeed, either type of these circulating antibodies can interfere, although to a variable extent, with thyroid hormone one-step assays.
The hypothesis of spuriously high free thyroid hormones can be supported by the determination of both fT4 and fT3 in frozen stored patient sera by a two-step chemiluminescent assay (Architect), which gave invariably normal results (Table 1). Heterophilic antibodies in the serum sample can induce binding between the capture antibody and the signal antibody, even in the absence of the analyte, thus resulting in abnormally high values. Sometimes, the heterophilic antibody can bind only the capture antibody and block the binding of the analyte, resulting in abnormally low values (10). Although it has also been described for free thyroid hormones (22), this interference most frequently affects the measurement of TSH, while THAb most commonly interfere with fT4 and fT3 measurements (23).
Thus, it was hypothesized that this patient had circulating THAb. This hypothesis was tested with the direct determination of THAb of both the IgG and IgM class on frozen stored serum samples, starting with the first sample available (week 30 of gestation). Indeed, THAb were demonstrated (Figs. 2 and 3). Interestingly, IgMT3, IgGT3, and IgMT4 were positive in all samples starting from 30 week of gestation; IgGT4 became detectable only in the last weeks of gestation.
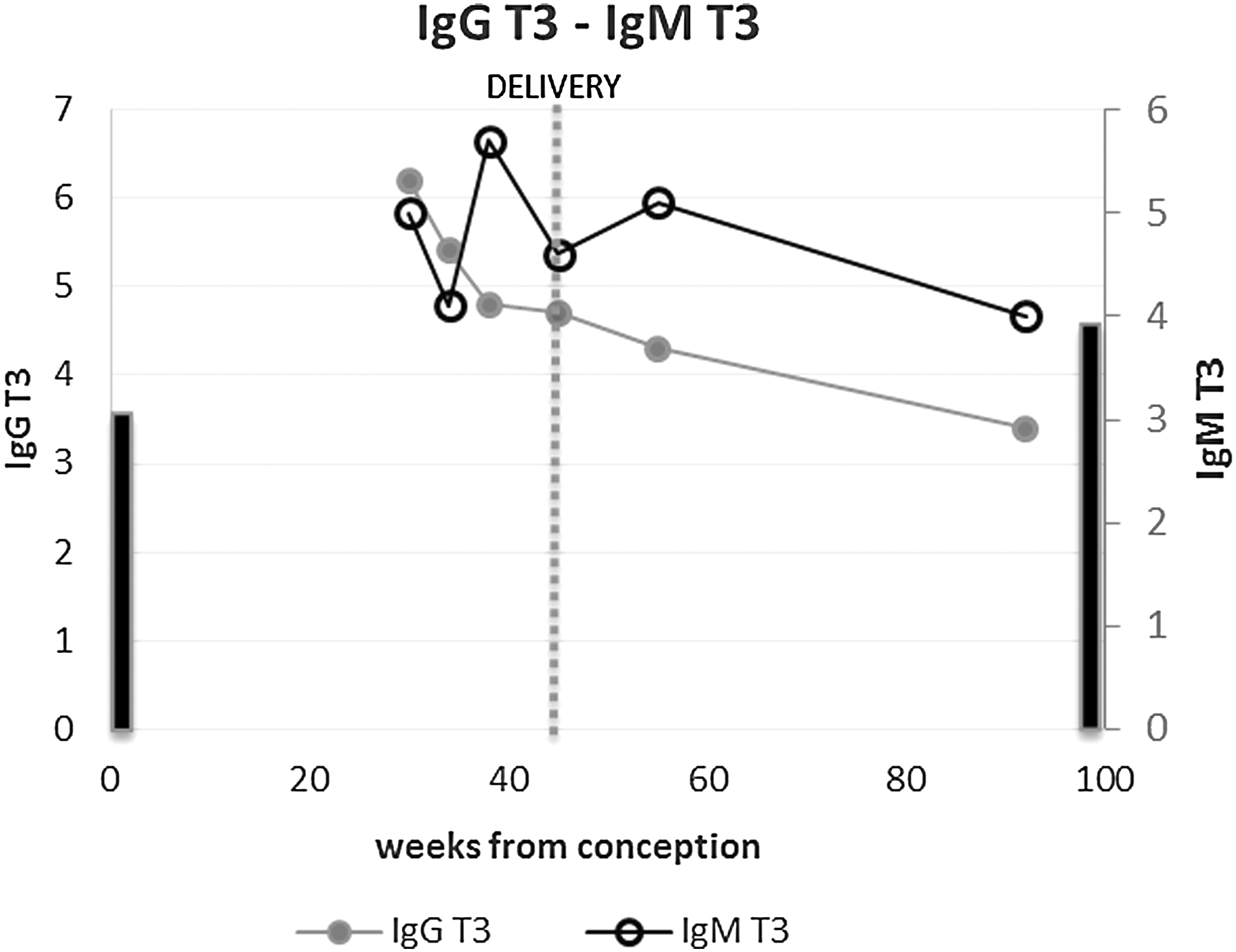
IgGT3 and IgMT3 (% bound/total). Normal values of IgGT3 and IgMT3 (% bound/total) are indicated by the two solid bars on the corresponding vertical axes.
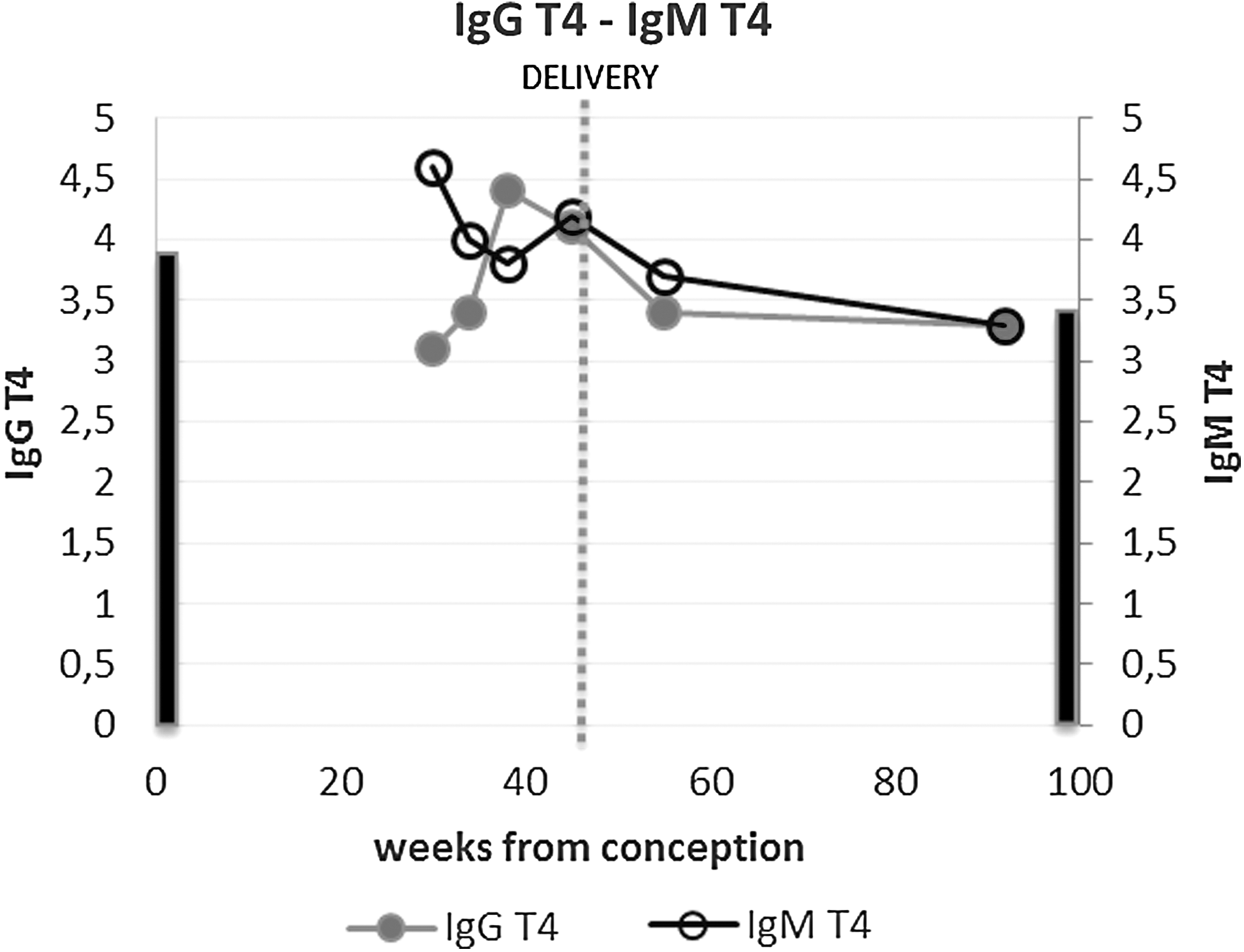
IgGT4 and IgMT4 (% bound/total). Normal values of IgGT4 and IgMT4 (% bound/total) are indicated by the two solid bars on the corresponding vertical axes.
Rheumatoid factor, ANA, AMA, ASMA, antiparietal cells, TPO, and TgA antibodies were negative in all sera of the patient.
Discussion
Despite their relative rarity, the presence of circulating autoantibodies able to interfere with free thyroid hormone assays may be suspected when laboratory data are internally inconsistent and contrast with the clinical picture. Knowledge of local laboratory methods is necessary in order to understand how misleading results may occur. THAb interference depends on the employed assay method: single- versus double-antibody procedure, analog versus non-analog tracer, and one- versus two-step assay. The one-step procedure shows the highest risk for interference by THAb because the assay antibody and the labeled tracer are directly in contact with the patient's serum (10). Two-step methods appear less susceptible to THAb interference because, in principle, there is no contact between serum components and the tracer (24 –26).
THAb may be directed against one or both thyroid hormones T3Ab, T4Ab, or T3/T4Ab (25). The frequency of THAb in the general population is 0–2% (27). The frequency of THAb has been described as increased in patients with autoimmune thyroid diseases, Hashimoto's thyroiditis, and Graves' disease. The rate of positivity for THAb also seems to increase in subjects with nonthyroid autoimmune diseases, such as primary Sjögren's syndrome and rheumatoid arthritis (27).
In the literature, different conditions have been associated with transient THAb elevations, for example therapy with interferon alpha (21) and viral infections (28), but to the authors' knowledge no previous case of transient appearance of THAb in pregnancy has been described. An interesting report describes the detection of isolated elevated serum fT4 levels in a pregnant woman, but the cause was FDH (29). As explained above in the Case Report section, the possibility of FDH in this patient was excluded. Increased concentrations of free thyroid hormones have been described in three women from a cohort of patients with postpartum thyroiditis (30). All of them showed increased serum concentrations of thyroid autoantibodies. The antibody binding of radiolabeled analogs and its effect on fT4 and fT3 assays disappeared by 48 weeks postpartum. Approximately 2% of women who develop thyroid autoantibodies in the postpartum period display an antibody interference in the analog methods for measurement of free thyroid hormones (30). Unfortunately, it is not known whether these women had further pregnancies with recurring abnormalities in fT4 and fT3 measurements.
The reason for the formation of THAb during pregnancy in this patient remains unknown. Literature data concerning the possible occurrence of THAb during normal pregnancy are lacking. However, in the early 1990s, 72 healthy pregnant women with normal serum free thyroid hormone values were evaluated for the presence of THAb in the authors' laboratory with the same method as in the present report (Benvenga et al., unpublished). None of these 72 women tested THAb positive.
Of note, during her first pregnancy, the present patient had routine evaluation of thyroid function without any remarkable abnormality of free thyroid values measured with a one-step method (ECLIA Roche) both during pregnancy (fT4 13 pg/mL at 6 weeks; fT4 14 pg/mL and fT3 2.65 pg/mL at 11 weeks; fT4 11.9 pg/mL and fT3 2.24 pg/mL at 16 weeks; fT4 10.9 pg/mL and fT3 2.04 pg/mL at 19 weeks; fT4 11.8 pg/mL and fT3 2.32 pg/mL at 36 weeks) and at one year postpartum (fT4 12.5 pg/mL and fT3 2.6 pg/mL). Indeed, the positive history for Hashimoto's thyroiditis represents a risk factor for developing THAb. The fact that the patient was TPOAb-negative during her second pregnancy does not contradict the previous diagnosis of Hashimoto's thyroiditis, as these antibodies are not present in 100% of patients, and during pregnancy, the antibody levels tend to decline. In addition, the proportion of patients with Hashimoto's thyroiditis that are TPOAb-negative and/or TgAb-negative seems to have increased over the years in Italy (31,32). Moreover, screening for other unrelated autoantibodies, namely rheumatoid factor, ANA, AMA, ASMA, and anti-gastric parietal cell antibodies, was negative. Furthermore, the patient did not undergo thyroid fine-needle aspiration biopsy, which could cause the de novo appearance of THAb (18).
Interestingly, the presence of chimeric cells in pregnant women was demonstrated, with a variable distribution across different organs (33). Thus, one might speculate that the present patient came in contact with fetal thyroid epitopes, and this could have triggered the formation of THAb. This hypothesis could be supported by the fact that the patient underwent amniocentesis at the 16th week of gestation.
Considering the possible role of viral infections as a trigger event, the history excluded the occurrence of a symptomatic infection in the patient during pregnancy. However, a more thorough medical history highlighted that the eldest child had contracted symptomatic human herpes virus 6 (HHV6) infection while the patient was in the second trimester of her second pregnancy. This fact is interesting, as HHV6 belongs to the herpes virus family, like Epstein–Barr virus (EBV), which has been reported to induce the formation of THAb (28). Such EBV-induced THAb are transient (28). Unfortunately, it has not been possible to evaluate HHV6 IgM antibodies in the second trimester. There was only the possibility of demonstrating the presence of HHV6 IgG but not IgM antibodies at the end of the pregnancy (data not shown), which does not provide unequivocal evidence of a recent HHV6 infection. In contrast, it could be demonstrated that THAb included both T3IgM and T4IgM. At present, a hypothesis concerning the formation of THAb is only speculative, but amniocentesis and HHV6 infection of the eldest child are the only two events that could be identified as possible triggers.
In conclusion, the importance of recognizing assay interferences in order to avoid unnecessary and potentially harmful therapies is emphasized, especially at a delicate time such as pregnancy.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.