
Abstract
Background:
Thyroid nodular disease is a very common clinical problem. The diagnostic algorithm includes laboratory tests, thyroid ultrasound (US), thyroid scintigraphy, and, if necessary, US-guided fine-needle aspiration cytology. However, cytology results are reported as indeterminate in a not negligible number of patients. This is a central problem in the workup of patients, since about 55–85% of those undergoing surgery do not have thyroid cancer at final histology diagnosis. The aim of this study was to evaluate prospectively the role of 99mTc-methoxy-isobutyl-isonitrile (99mTc-MIBI) thyroid scintigraphy in differentiating malignant from benign thyroid nodules with indeterminate cytology using quantitative analysis.
Method:
One hundred five patients affected by nodular thyroid goiter and with a euthyroid or hypothyroid functional status were prospectively evaluated. All patients had a suspicious nodule ≥15 mm in maximal diameter on US. All nodules were “cold” on 99mTc-pertechnetate scintigraphy and had a cytological diagnosis of class III or IV according to the Bethesda system. Planar images of the thyroid were acquired 10 and 60 minutes after 99mTc-MIBI administration. All cold nodules were MIBI-positive. Using quantitative analysis, the MIBI washout index (WOind) was calculated as a percentage reduction value of mean MIBI nodular uptake between early (+10 minutes) and late (+60 minutes) scans.
Results:
Subdividing the patients into positive and negative for malignancy (either including or excluding patients with Hürthle cell adenoma) and performing receiver operating characterist curve analysis, the optimal WOind cutoff in differentiating malignant from benign follicular lesions was set at −19%. The overall sensitivity and specificity of 99mTc-MIBI quantitative analysis in identifying patients with malignant lesions was 100% and 90.9%, respectively. However, after excluding patients with Hürthle cell adenomas from the negative patient group, the overall sensitivity and specificity both reached 100%.
Conclusion:
The use of MIBI scintigraphy using quantitative analysis in the workup of cold nodules with indeterminate cytology is suggested in order to stratify patient risk for a malignant lesion better, thus reducing the number of patients referred to surgery. Surgical treatment should be planned in those patients with a WOind up to −19%.
Introduction
T
The diagnostic evaluation of thyroid nodules includes thyrotropin (TSH) measurement and thyroid ultrasonography (US) as a first step. Thyroid scintigraphy with either 123iodine or 99mTc-pertechnetate is also performed to characterize hyperfunctioning (i.e., “hot”) nodules that need no further diagnostic tests. In other cases, US is used to select the nodule(s) requiring US-guided fine-needle aspiration cytology (FNAC) (4,5).
This diagnostic algorithm has proven to be accurate in detecting and excluding thyroid cancer, thus avoiding inappropriate surgical interventions in many cases. However, faced with follicular-patterned lesions, cytopathologists cannot discriminate benign from malignant lesions, since detection or exclusion of capsular and/or vascular invasion cannot be done on cytological specimens (6,7).
As the large majority of such lesions are benign, the risk of inappropriate thyroid surgery is relevant. In order to improve accuracy and reproducibility of cytological diagnoses, two main classification systems are now used in daily practice (8,9). To stratify the risk of malignancy better, both systems subdivide nodules with indeterminate cytology into two subclasses (III and IV, and IIIa and IIIf, respectively). However, the number of unnecessary surgeries remains quite high.
Indeed, about 55–85% of patients who underwent thyroid surgery due to IV or III Bethesda class nodules (suspicious for follicular neoplasm or follicular neoplasm [SFN/FN] or atypia of undetermined significance/follicular lesion of unknown significance [AUS/FLUS], respectively) turned out to have a benign lesion at histological evaluation (9 –13).
Some authors have already reported on the role of 99mTc-methoxy-isobutyl-isonitrile (99mTc-MIBI) in thyroid disease (14) and in particular in differentiating malignant from benign lesions in patients with non-diagnostic/indeterminate cytology (4,15 –18). Overall, a negative MIBI scan (i.e., absent uptake in a nodule) excludes malignancy, while a positive MIBI scintigraphy (i.e., present uptake in a nodule) can be found both in malignant and benign lesions (4,15 –17). Quantitative analysis of thyroid scans has proven to increase accuracy (6,18).
The aim of this prospective study was to assess the role of 99mTc-MIBI thyroid scintigraphy in discriminating malignant from benign Bethesda class III and IV nodules using quantitative analysis.
Patients
One hundred five patients (80 female; M age = 47.9 ± 12.6 [range 20–80 years]; median age = 49 years; F/M = 3.2:1) affected by nodular thyroid goiter and referred to the Nuclear Medicine and Endocrine Units, “G. Martino” University Hospital, Messina (Italy) or the Department of Nuclear Medicine and Thyroid Centre, Oncology Institute of Southern Switzerland, Bellinzona/Lugano (Switzerland), respectively, from January 1, 2013, through March 31, 2015, were prospectively evaluated.
All patients fulfilled the following inclusion criteria: (i) age ≥18 years; (ii) TSH levels >0.40 mIU/L and calcitonin values <5 ng/L (women) and 10 ng/L (men); (iii) one solid thyroid nodule ≥15 mm in maximal diameter, solid on US and cold on 99mTc-pertechnetate scintigraphy; and (iv) a cytological diagnosis of class III or IV according to the Bethesda system.
Twenty out of all patients (19%; 16 female; M age = 52.3 ± 8.2) were hypothyroid: 15 (75%; 12 female; M age = 53.2 ± 6.8) had overt hypothyroidism, and the remaining patients (25%; 3 female; M age = 50.9 ± 5.8) had subclinical hypothyroidism. All overtly hypothyroid patients were treated with a replacement dose of levothyroxine (LT4; 1.7–2.0 μg/kg/day).
99mTc-MIBI thyroid scintigraphy was performed in all patients, and images were evaluated both qualitatively and quantitatively.
All patients underwent thyroid surgery (lobectomy or total/near-total thyroidectomy) in order to confirm or exclude a malignant lesion.
Finally, 99mTc-MIBI thyroid scintigraphy results were matched with histology findings in order to identify MIBI scintigraphy features (qualitative and mainly quantitative) of patients with malignant thyroid nodules (i.e., differentiated thyroid cancer [DTC]) compared to all remaining patients (i.e., non-DTC patients).
The study was approved both by the Ethics Committee of the University Hospital of Messina and the Oncology Institute of Southern Switzerland (Bellinzona, Switzerland), and written informed consent was obtained from each patient.
Methods
Thyroid US and FNAC
US examinations were performed by two well-trained physicians using a real-time 2D apparatus Logiq3 Expert (GE Healthcare, Little Chalfont, United Kingdom) or an ACUSON®3000 (Siemens, Erlangen, Germany), both equipped with a high-frequency linear transducer. Nodules were considered suspicious if they met the TI-RADS criteria, as already described (19).
FNAC was performed by two well-trained physicians under echo guidance using a 23-gauge needle attached to a 10 mL syringe.
Cytological and histological diagnosis
The material was air-dried, stained with Papanicolaou and Giemsa, and interpreted by two experienced cytologists. The adequacy of aspirates was defined according to the guidelines of the Papanicolaou Society (20).
If the number of large follicular cells with typical features was at least 50% of the total follicular cells, the lesion was considered an oncocytic follicular neoplasm.
Cytological results were classified according to the Bethesda system (9): class I non-diagnostic, class II benign, class III indeterminate/atypical, class IV SFN, class V suspicious for malignancy, and class VI malignant. Patients with a cytological reading of AUS/FLUS (class III) or SFN (class IV) were enrolled in the present study.
For histological diagnoses, formalin-fixed, paraffin-embedded surgical samples were stained by hematoxylin and eosin, and the diagnosis was made by the same trained pathologists.
Nuclear medicine
Thyroid scintigraphies were obtained by using a dual-headed gamma camera equipped with low-energy high-resolution parallel-hole collimators (LEHRPAR; Brightview-X, Philips, Cleveland, OH; and Symbia-T2, Siemens, Erlangen, Germany) and evaluated by two board-certified nuclear-medicine physicians with >20 years’ experience in the field. In patients treated with LT4, therapy was withdrawn 10–15 days before thyroid scintigraphy. Planar anterior images (magnification: 1; matrix 256 × 256; frame time: 100 Kcounts; energy peak: 140 ± 20 KeV) of the neck were obtained 15–20 minutes after intravenous injection of 99mTc-pertechnetate (74–111 MBq). Nodules were considered “cold” (i.e., hypofunctioning) if the tracer uptake was lower than in normal thyroid tissue.
Additional planar images were acquired 10 and 60 minutes after intravenous administration of 99mTc-MIBI (200–400 MBq; magnification: 1 and 1.4; matrix: 256 × 256 and 128 × 128, respectively; frame time: 600 sec; energy peak: 140 ± 20 KeV). Images were evaluated qualitatively, in double-blind modality, comparing 99mTc-MIBI uptake and 99mTc-pertechnetate uptake within the nodule, respectively. The visual assessment used the following scoring system: pattern 1 = MIBI uptake ≤ 99mTc-pertechnetate uptake; pattern 2 = MIBI uptake > 99mTc-pertechnetate uptake on the early image: early MIBI uptake > late MIBI uptake; pattern 3 = MIBI uptake > 99mTc-pertechnetate uptake on the early image: early MIBI uptake = late MIBI uptake (Fig. 1).

Visual assessment of 99mTc-methoxy-isobutyl-isonitrile (99mTc-MIBI) scintigraphy. (
Pattern 3 was considered suspicious for malignancy, while both pattern 1 and pattern 2 were considered negative for malignancy.
A quantitative analysis was also performed by drawing regions of interest (ROIs) around the nodule and then mirroring the ROI outside the thyroid to subtract the background activity. ROIs were created on early images and successively copied on delayed ones.
99mTc-pertechnetate and 99mTc-MIBI images (early and late) were displayed on the same screen to be more precise in drawing the ROI.
Parameters derived from ROI analysis were: mean MIBI nodular uptake, pixel nodular number, mean MIBI background uptake, and pixel background number. Then, the MIBI washout index (WOind) was calculated as a percentage reduction value of mean MIBI nodular uptake between early (+10 minutes) and late (+60 minutes) scans.
The formula employed to calculate WOind is:
Mean nodular MIBI uptake (early scan) – mean background MIBI uptake (early scan) = early result (ER)
Mean nodular MIBI uptake (late scan) – mean background MIBI uptake (late scan) = late result (LR)
LR/ER × 100 – 100 = WOind
Surgery and pathology
As per our clinical protocol, all patients underwent thyroid surgery. Among 105 patients, 100 (95.2%) underwent (near-) total thyroidectomy and five (4.8%) lobectomy, respectively. Histologic analyses were performed and reported by experienced endocrine pathologists.
Statistical analysis
A preliminary power analysis was performed to calculate the minimum sample size required to accept the outcome of a statistical test, with a confidence level of α = 0.050. The sample size required to ensure a power level of 0.80 was >100 cases. Continuous variables are expressed as means and standard deviations (SD; or median and range in the case of non-normal distribution), and categorical variables as number and percentage.
Examined variables did not present normal distribution as verified by the Kolmogorov–Smirnov test. Consequently, the non-parametric approach was used.
Receiver operating characteristic (ROC) analysis was also performed to determine the WOind threshold below which malignant thyroid nodules could be detected. The area under the curve (AUC) was calculated to assess the overall accuracy of 99mTc-MIBI scan quantitative analysis.
The Kruskall–Wallis test and Mann–Whitney U-test were employed to compare intergroup distributions. In order to assess the association between categorical variables, the chi-square test was applied, or Fisher's exact test (i.e., only in cases in which a frequency in the contingency table was <5) or log likelihood ratio test (when a frequency in the contingency table was 0) if necessary.
Statistical analyses were performed using SPSS Statistics for Windows v17.0 (SPSS, Inc., Chicago, IL) and, for ROC analysis, Stats Direct v2.8 (StatsDirect Ltd, Altrincham, UK).
A two-sided p-value of <0.050 was considered statistically significant.
Results
The cytology results of 40/105 (38%) nodules were classified in class III and 65 (62%) in class IV according to the Bethesda classification system.
MIBI uptake exceeded 99mTc-pertechnetate uptake in all cases, with pattern 2 in 79 (75.2%) and pattern 3 in 26 (25.8%), respectively (Table 1).
Pattern 2 = increased nodular MIBI uptake (99mTc-MIBI > 99mTc-Pertechnetate) on early image that decreased on late image.
Pattern 3 = increased nodular MIBI uptake (99mTc-MIBI > 99mTc-Pertechnetate) on early image that remained unchanged on late image.
Seven oncocytic types.
MIBI, methoxy-isobutyl-isonitrile; SD, standard deviation; DTC, differentiated thyroid carcinoma.
Pattern 2 was significantly more prevalent in female patients (p = 0.001), while pattern 3 was more prevalent in male patients (p = 0.001).
Considering pattern 2 as negative for malignancy, the sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of visual MIBI analysis in differentiating malignant from benign nodules were 60.7%, 90.9%, 82.8%, 70.8%, and 86.4%, respectively.
Considering the quantitative MIBI analysis, the optimal WOind cutoff was set at –19%, and performing ROC curve analysis (including Hürthle cell adenomas), the overall sensitivity, specificity, accuracy, PPV, and NPV of 99mTc-MIBI quantitative analysis were 100%, 90.9%, 93.3%, 80%, and 100%, respectively (AUC = 0.96). Excluding patients with Hürthle cell adenomas, the overall sensitivity, specificity, accuracy, PPV, and NPV reached 100% (AUC = 1.00; Fig. 2A and B, respectively).
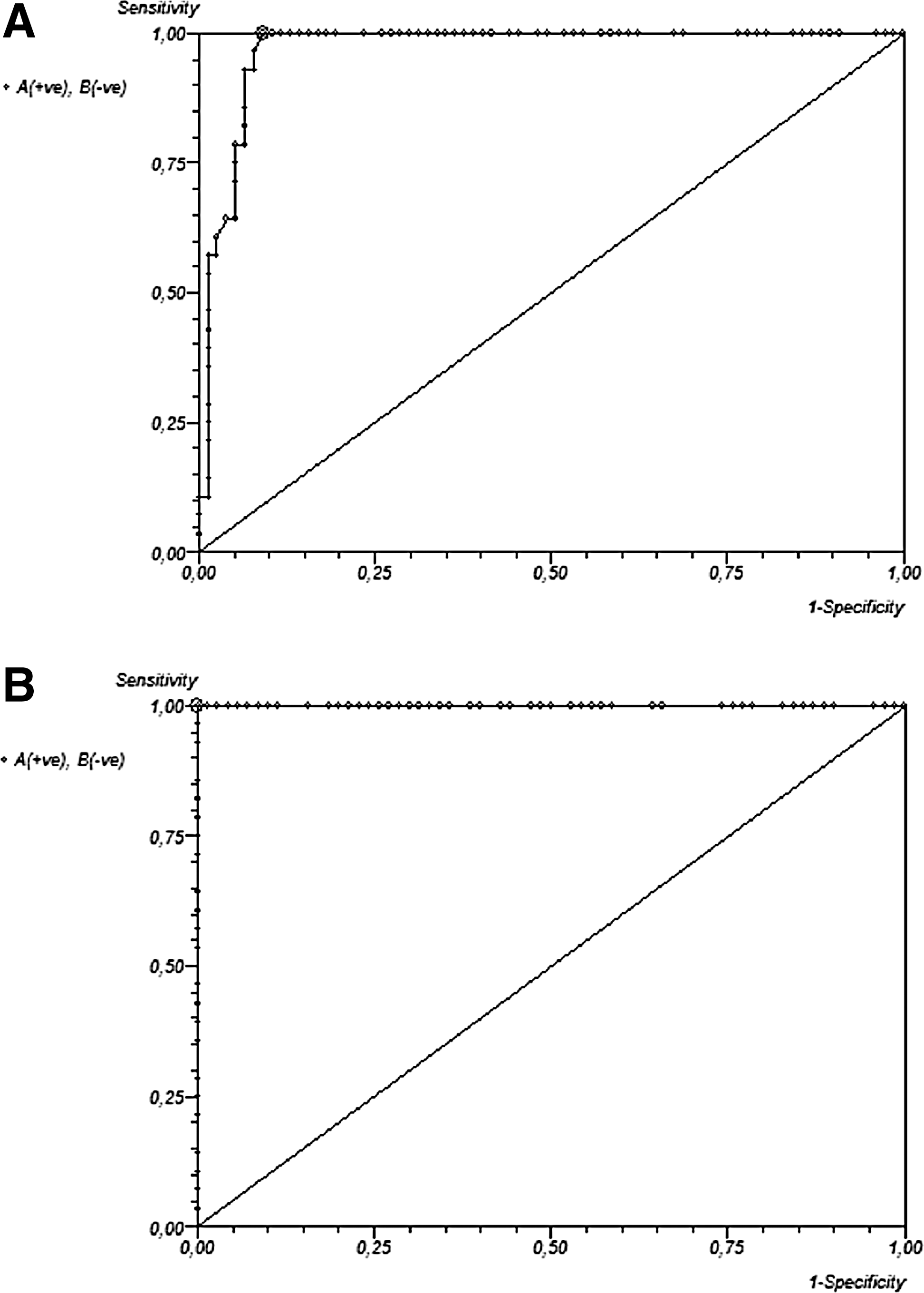
Receiver operating characteristic (ROC) analysis. (
Interestingly, all patients with a WOind ≤–40% had a benign final histology (i.e., colloid goiter; group A, n = 29; sensitivity and NPV: 100%).
All except seven patients affected by benign adenomas had a WOind <–40% < WOind ≤ −20% (i.e., included between <–40% and ≤–20%; group B, n = 41; sensitivity: 85.4%). In this group, younger patients had a lower WOind compared with older patients (p = 0.04).
The WOind of patients included in groups A and B is reported in Table 2.
Suspicious for follicular neoplasm (SFN).
Follicular neoplasm (FN). TI-RADS classification: 1, normal; 2, benign; 3, probably benign; 4A, undeterminated pattern; 4B, suspicious pattern; 5, consistent with malignancy.
RL, right lobe; LL, left lobe; I, isthmus.
Finally, 28/35 patients with a WOind >–20% (group C) were affected by DTC (specificity and PPV: 80.0%; accuracy 93.3%; Fig. 3 and Table 3).
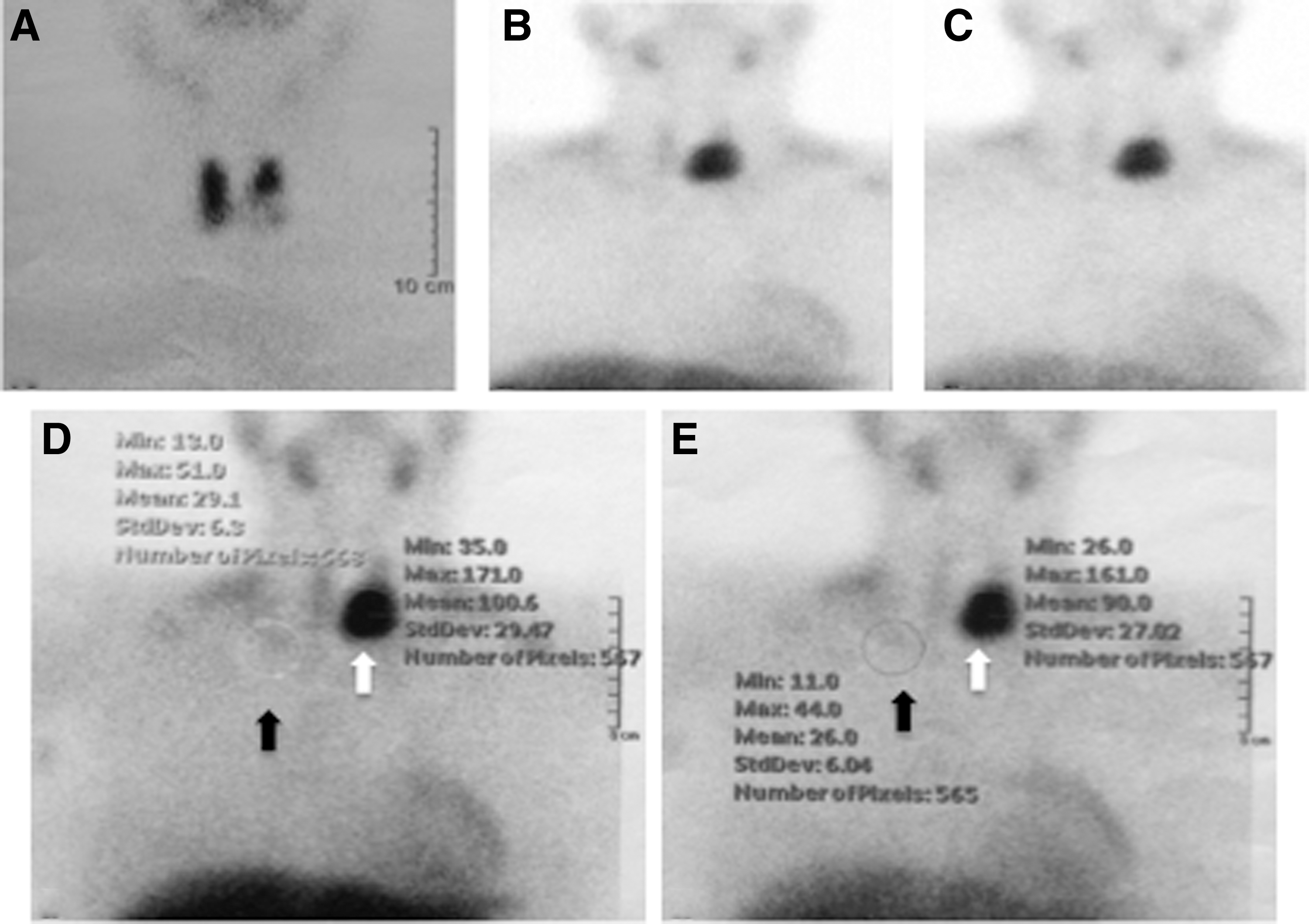
Twenty-year-old woman with a single nodule located in the left lobe. The nodule (34 mm in maximal diameter) presented a 4A pattern on ultrasound (US; TI-RADS classification). (
SFN.
FN. TI-RADS classification: 1, normal; 2, benign; 3, probably benign; 4A, undeterminated pattern; 4B, suspicious pattern; 5, consistent with malignancy.
The mean nodule size and WOind of group C patients were 27.2 ± 8.3 mm (median = 28) and −11.4%, respectively. Interestingly, all false-positive patients included in group C had benign Hürthle cell adenomas (on cytology, three were read as SFN while four were read as FN [oncocytic type in two of them]) and showed a pattern 2 MIBI uptake.
In patients affected by Hürthle cell adenomas (all women; M age = 48.7 ± 5.6 years; median = 48 years; range 39–56 years), the mean size of suspicious nodules and WOind were 23.7 ± 6.02 mm (median = 25) and –14.3%, respectively. These patients did not have any significant differences in term of WOind and/or mean size of lesions and/or clinical characteristics compared to patients affected by DTC (p = 0.187, and p = 0.301 and p = 0.205, respectively).
Subdividing group C patients on the basis of age (<50 or >50 years), it emerges that the risk of having DTC was about 21% higher in older compared with in younger patients (odds ratio = 2.17).
In the present series, the prevalence of DTC was slightly higher in male patients (p = 0.050) and in nodules located in the isthmus (p = 0.023). Isthmus nodules and adenomas were significantly smaller compared with those located in the lobes and DTC nodules, respectively (p < 0.001 and p = 0.028, respectively). Considering sex, women had smaller nodules than male patients had (p = 0.013). Finally, patients with final histologic diagnosis of colloid goiters had significantly greater nodules compared with other patients (p = 0.001).
Discussion
To date, the prevalence of nodules with indeterminate cytology (i.e., AUS/FLUS or SFN/FN) ranges from 20% to 30%. Many published data have demonstrated that up to 85% of patients with an indeterminate cytology do not have a malignant tumor on final histologic diagnosis (9,10).
The recently published 2015 American Thyroid Association ATA) Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer discussed the possible role of 18F-FDG-PET/CT in differentiating malignant from benign lesions (5). According to the ATA guidelines, the use of PET/CT is not routinely recommended in this setting (5).
However, several authors (4,17,18) have already reported on the possible role of 99mTc-MIBI. In particular, the very high sensitivity and NPV of a negative MIBI scan in ruling out malignancy has been reported. In their prospective study, Giovanella et al. (4) showed how sensitivity and the NPV of a negative MIBI scan was 100% in ruling out malignancy. Similar results were published two years later by Brukner et al. (17). In their retrospective study, conducted on a very large cohort of patients, the sensitivity and the NPV of a negative MIBI scan in ruling out malignancy were 88.2% and 95.1%, respectively.
On the contrary, a positive MIBI scan can be found in both malignant and benign lesions, thus reducing its specificity and PPV, as reported in the series published by Giovanella et al. (4) and Brukner et al. (17), where the PPV values were found to be quite low (27% and 17.4%, respectively).
In the series presented here, all studied nodules were positive on visual MIBI analysis, but less than a third had DTC on final histologic diagnosis (specificity and PPV, 26.6%), findings that confirm the previously published data (4,17). However, after subdividing patients according to a visual scoring assessment (i.e., pattern 2 or 3), the specificity and PPV improved, reaching suboptimal values (90.9% and 70.8%, respectively). Furthermore, an overlap between malignant and benign lesions was noticed in nodules with pattern 2 on MIBI scanning (i.e., negative for malignancy). Consequently, it is confirmed that qualitative analysis of MIBI is not useful in reducing unnecessary surgery procedures.
In this setting, the use of semi-quantitative analysis for improving the diagnostic performance of MIBI thyroid scintigraphy has been previously evaluated. In a prospective study, Saggiorato et al. (18) showed how semi-quantitative analysis greatly improved the diagnostic accuracy of positive MIBI scans, showing a better sensitivity and specificity than visual analysis in differentiating between malignant and benign nodules in patients with non-oncocytic follicular lesions (100% and 90.48% vs. 73.33% and 80.95%). In the series presented here, quantitative analysis of MIBI washout significantly improved diagnostic accuracy in discriminating malignant from benign nodules. However, confirming previous data (18,21 –24), WOind of Hürthle adenomas did not show significant differences compared to that of malignant nodules. The delayed washout of tracer from Hürthle cells is likely related to the negative transmembrane mitochondrial electric potential; the amplitude is similar to that of malignant cells and larger than that of normal cells (25,26). Despite this limitation, the very high NPV of quantitative MIBI analysis allows surgery to be avoided in patients with non-oncocytic follicular-patterned lesions on cytological analysis.
Other methods and mainly molecular testing of FNA specimens (5,27) or core-needle biopsy (28,29) have been proposed to improve the diagnostic accuracy. However, neither core-needle biopsy nor current molecular testing allows malignancy to be ruled in or out in all patients with indeterminate cytology.
A MIBI scan has proved more cost-effective when compared with molecular testing, as already described (30). In the authors’ experience, the total cost of performing a MIBI diagnostic test (considering clinical evaluation, 99mTc-pertechnetate thyroid scintigraphy, thyroid MIBI scintigraphy, report on diagnostic findings) for each patient ranged from €93 to €205 (rounded). In contrast, the Afirma gene expression classifier has an average cost of €3000 (rounded). Thus, MIBI scanning may be a relatively cheap diagnostic test, and it may be significantly cheaper than molecular testing, although costs vary between different healthcare systems. In addition, Giovanella et al. (6) have recently demonstrated how semi-quantitative MIBI analysis was more effective than molecular testing was for differentiating malignant from benign nodules.
There are two possible weaknesses to the use of the proposed quantitative MIBI analysis. First, the WOind calculation is, at least in part, an operator-dependent method that requires defining and drawing of ROIs. Second, the method is partially dependent on the instruments used.
However, taking into account both the very high accuracy in differentiating malignant from benign lesions and the very low cost, it is believed that each nuclear medicine center could easily employ this method after an adequate training period, thus reducing the number of patients sent for unnecessary surgery procedures.
Conclusion
The present results support the use of quantitative MIBI analysis in patients with cold nodules reported as AUS/FLUS (class III) or SFN/FN (class IV) to exclude patients with MIBI-negative (i.e., WOind >–20%) nodules from surgery. Using the new ATA guidelines as reference, it is proposed that nodules with WOind <–40% < WOind ≤ −20% (i.e., included between <–40% and ≤–20%) and ≤–40% are considered as intermediate and low risk, respectively, and they may be followed with clinical and/or US follow-up.
Footnotes
Author Disclosure Statement
The authors disclose no conflict of interest, and no funding was received for this work.