
Abstract
Introduction:
The diffuse sclerosing variant (DSV) of papillary thyroid cancer (PTC) is considered an aggressive histotype associated with poor prognosis. However, the available data for both the outcome and best management of this disease are inconsistent.
Methods:
This study reviewed the current literature by searching PubMed up to November 30, 2015, using the search terms “diffuse sclerosing variant” and “papillary thyroid cancer (or carcinoma)” and selecting only studies evaluating recurrent/persistent disease and cancer-related mortality in both DSV and classic PTC (cPTC). The association with some features of aggressiveness at diagnosis, the risk of recurrence or persistence, and the risk of cancer-related death were reported as odds ratio (OR) with confidence intervals (CI). Meta-regression analysis was used to assess the effect of covariates across the studies.
Results:
Ten studies met the eligibility criteria and contributed 585 DSV and 64,611 cPTC patients. Relative to patients with cPTC, patients with DSV exhibited a higher risk of extrathyroidal extension and lymph node and distant metastases. The risk of persistent/recurrent disease was three times higher in patients with DSV than it was in cPTC patients (OR = 3.19 [CI 1.86–5.49]). This risk was not different when only studies where post-surgical 131I was routinely administered were considered (OR = 2.07 [CI 0.88–4.90]). The risk of cancer-related mortality was not different between DSV and cPTC (OR = 1.34 [CI 0.76–2.38]).
Conclusions:
This meta-analysis confirms the aggressive biological behavior of DSV thyroid cancer. When preoperatively suspected, total thyroidectomy with lymph node excision followed by radioiodine therapy should be the correct management for DSV.
Introduction
P
The diffuse sclerosing variant (DSV) of PTC is an uncommon histotype (0.7–5.3% of all PTC) (2 –7), first described in 1985 (8) and characterized by the diffuse involvement of thyroid tissue mimicking a chronic thyroiditis and without the presence of a dominant nodule. It tends to occur in young patients, and its typical histopathologic features include extensive lymph-vascular invasion, diffuse squamous metaplasia, dense lymphocytic infiltration, numerous psammoma bodies, and stromal fibrosis (9).
The recent American Thyroid Association (ATA) guidelines for differentiated thyroid cancer (10) suggest considering DSV as a PTC variant associated with a less favorable outcome. Prognosis and outcome of DSV, however, remain controversial. Some studies report that DSV is characterized by aggressive pathological features at diagnosis and poor outcomes (3,7,11,12), whereas other authors observed no difference in prognosis when comparing DSV and classical PTC (cPTC) (2,4 –6).
To investigate this issue, a meta-analysis was performed to evaluate the relationship between the thyroid cancer DSV, its clinicopathologic features at presentation, and its outcome in terms of persistent/recurrent disease and cancer-related death.
Materials and Methods
This study was carried out following the guidelines suggested in the PRISMA statement for the quality of reporting items in meta-analyses (13).
Data sources and search strategy
MEDLINE (PubMed database) was independently searched by two investigators (P.M. and M.R.) to identify relevant articles on pathological features at diagnosis and clinical course of patients with the DSV of PTC, and comparing these parameters with those observed in patients with cPTC. Studies published by November 30, 2015, were identified. The search used the terms “diffuse sclerosing variant” and “papillary thyroid carcinoma” or “papillary thyroid cancer.” Articles were independently selected by the two investigators by examining titles and abstracts, and only articles that potentially fulfilled our eligibility criteria (see below) were chosen. Selected articles were then further analyzed by a full-text evaluation.
Eligibility criteria
Only studies designed to compare the clinicopathologic features at diagnosis and the outcome (persistent/recurrent disease and cancer-related mortality) in patients with DSV and cPTC were considered eligible. Articles were included if they reported the surgical and post-surgical therapeutic approach and the subsequent follow-up, and if they included the number of patients with persistent/recurrent disease during follow-up and at last observation and the number of deaths for thyroid cancer. All types of articles were considered except Editorials and Letters. Articles with case reports or analyses of small series (five patients or fewer with DSV) were also excluded. Only articles published in the English language were considered.
Data extraction
Data on recurrence, persistent disease at last control, and tumor-related death were chosen as outcome indicators. Two investigators (M.R. and C.R.) independently evaluated the full text of the eligible articles to extract and record in an electronic data sheet all the potentially useful data. The two independently obtained data sheets were compared to identify inconsistencies. In case of discrepancy, the question was resolved by the evaluation of a third investigator (P.M.) and with the consensus of the three investigators. The data sheet included detailed information on the publication's first author and year, number of patients, mean age at diagnosis, female-to-male ratio, length of follow-up, pathological features at diagnosis (including multifocality, extrathyroidal extension, loco-regional lymph node, and distant metastases), number of patients with persistent/recurrent disease, and thyroid cancer-related death. All these data were recorded for both the DSV and cPTC histological variants.
Quality of selected studies and assessment of the risk of bias
The Newcastle–Ottawa Scale was used to estimate the quality of the selected articles (
Statistical analysis
Persistent or recurrent disease during or at the end of follow-up and cancer-related death were the outcomes of interest. Secondary outcomes were the occurrence of multifocality, extrathyroidal extension, lymph node metastases, and distant metastases. The number of patients with or without the outcomes of interest was obtained from the selected articles in both groups (DSV and cPTC), and a 2 × 2 table was constructed to estimate the Mantel–Haenszel pooled odds ratios (M–H pooled ORs) and confidence intervals (CIs). For studies with zero events in both groups, an empirical continuity correction was added to each cell of the 2 × 2 table. The continuity correction was calculated by estimating the pooled effect size from the remaining studies without zero cells, as previously described (15). This method is the least biased when applied to data on sparse events from studies with imbalanced sizes of the study arms. The between-study heterogeneity was investigated by calculating the I2 index, and values of ≥50% were considered as evidence of high heterogeneity. In this case, the random-effects model was used to pool the result. The fixed-effects model was used when the I2 index was <50%. Egger's test and visual inspection of a funnel plot were used to evaluate publication bias. Subgroup and meta-regression analysis were performed considering the potential effect of covariates known to be associated with the main outcomes. Selected covariates included mean age at diagnosis, percentage of male patients, percentages of patients with multifocality, extrathyroidal extension, lymph node and distant metastases, and percentages of patients who had undergone total thyroidectomy, lymph node excision, and post-surgical radioiodine therapy. The leave-one-out method was performed for sensitivity analysis to calculate a pooled estimate of the remaining studies. Two-sided tests were used, and a p-value of <0.05 was considered to be statistically significant. All analyses were conducted using Stata v13.1 (StataCorp, College Station, TX).
Results
Description of included studies
As of November 30, 2015, 147 articles were retrieved using the described search strategy. Of these, 10 studies met the eligibility criteria (2,4,7,12,16 –21). The detailed procedure for the study selection is described in Figure 1. Overall, selected studies contributed a total of 65,198 patients: 585 with DSV and 64,611 with cPTC. Clinicopathologic features of the patients included in the meta-analysis are summarized in Table 1.

Flow chart showing the meta-analysis study selection.
Standard error of the mean (SEM).
Diffuse sclerosing variant and classical PTC.
NA, not available.
Assessment of the risk of bias
Using the Newcastle–Ottawa Scale to estimate the quality of the studies selected, it was found that the overall bias risk of included studies was low to moderate (Table 1). Briefly, the majority of the studies were monocentric with no relevant imbalance in the criteria used for the selection of cases (i.e., patients with persistent/recurrent disease or death) and controls (i.e., patients cured and alive). In addition, no major inconsistencies were observed for the comparability between cases and controls. Indeed, all studies evaluated possible confounding factors in both groups. Finally, the method applied for the exposure ascertainment was also the same for both cases and controls (i.e., pathological diagnosis to define the DSV or the cPTC histotypes). The publication bias across the studies was investigated by visual inspection of the funnel plots, where no substantial asymmetry was identified (Fig. 2A and B), and by Egger's linear regression analysis for the two studied outcomes: persistent/recurrent disease (p = 0.13) and cancer-related mortality (p = 0.23).
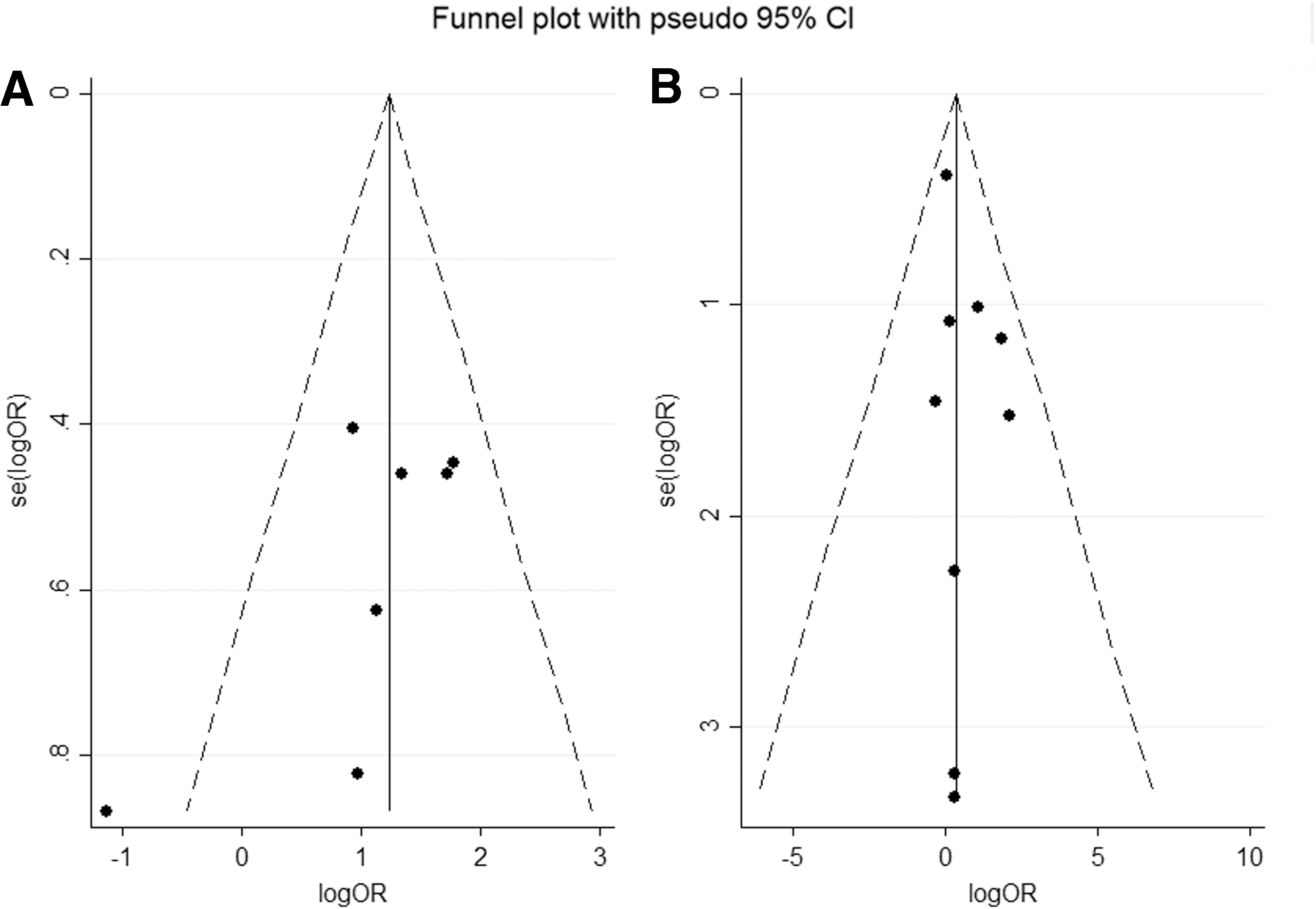
Funnel plots for publication bias considering both persistent/recurrent disease (
Meta-analysis of pathological features at diagnosis
At diagnosis, relative to patients with cPTC, patients with DSV had a higher risk of exhibiting features of cancer aggressiveness, such as extrathyroidal extension, lymph node metastases, and distant metastases (Fig. 3A, B, and C). The pooled OR was 2.13 [CI 1.74–2.59] for extrathyroidal extension, 2.91 [CI 1.88–4.50] for lymph node metastases, and 2.21 [CI 1.56–3.15] for distant metastases. Only multifocality was not different between DSV and cPTC [OR = 1.33 [CI 0.81–2.18]).
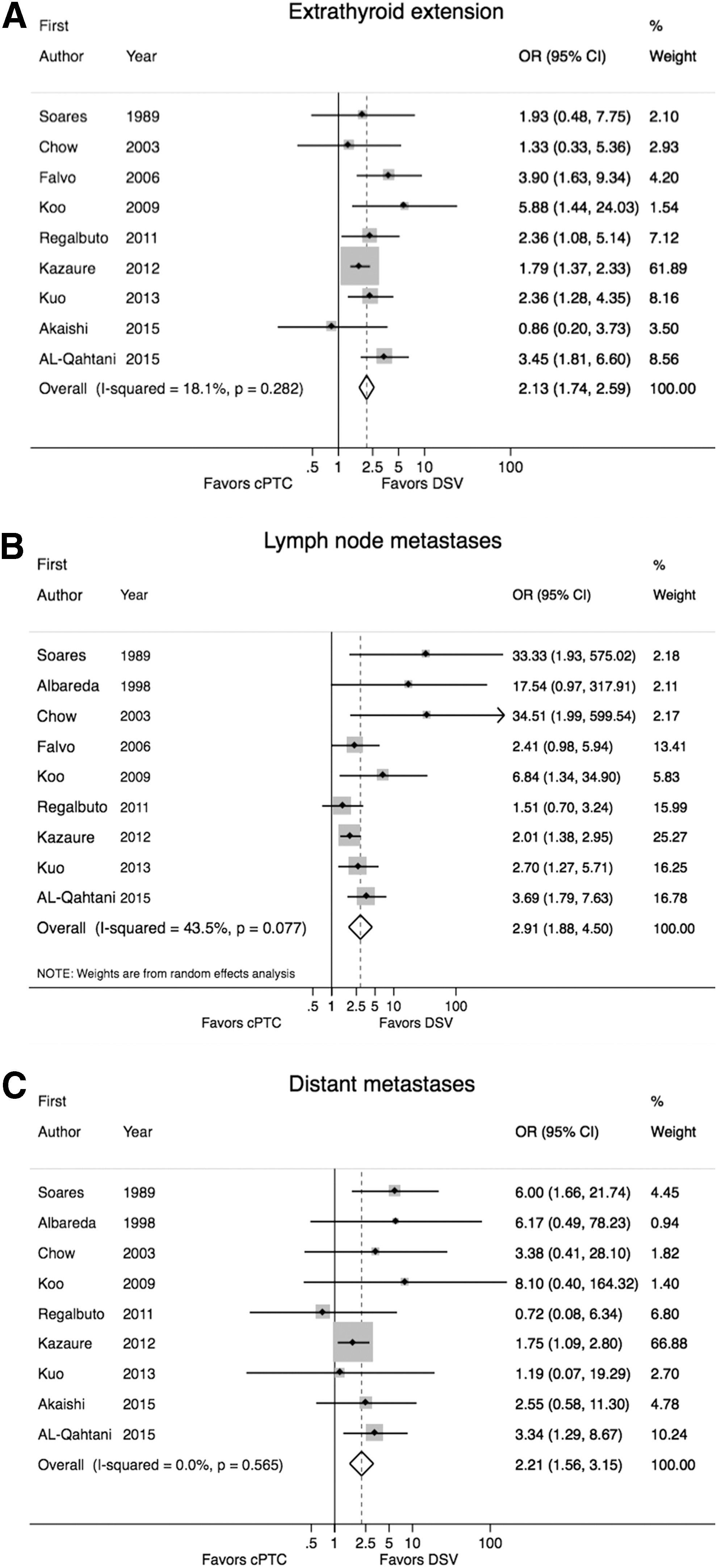
Forest plots of odds ratios (OR) for extrathyroidal extension (
The meta-regression analysis indicated a non-statistically significant inverse relationship between the age at diagnosis and the occurrence of either lymph node (p = 0.08) or distant metastases (p = 0.14; Fig. 4A and B).
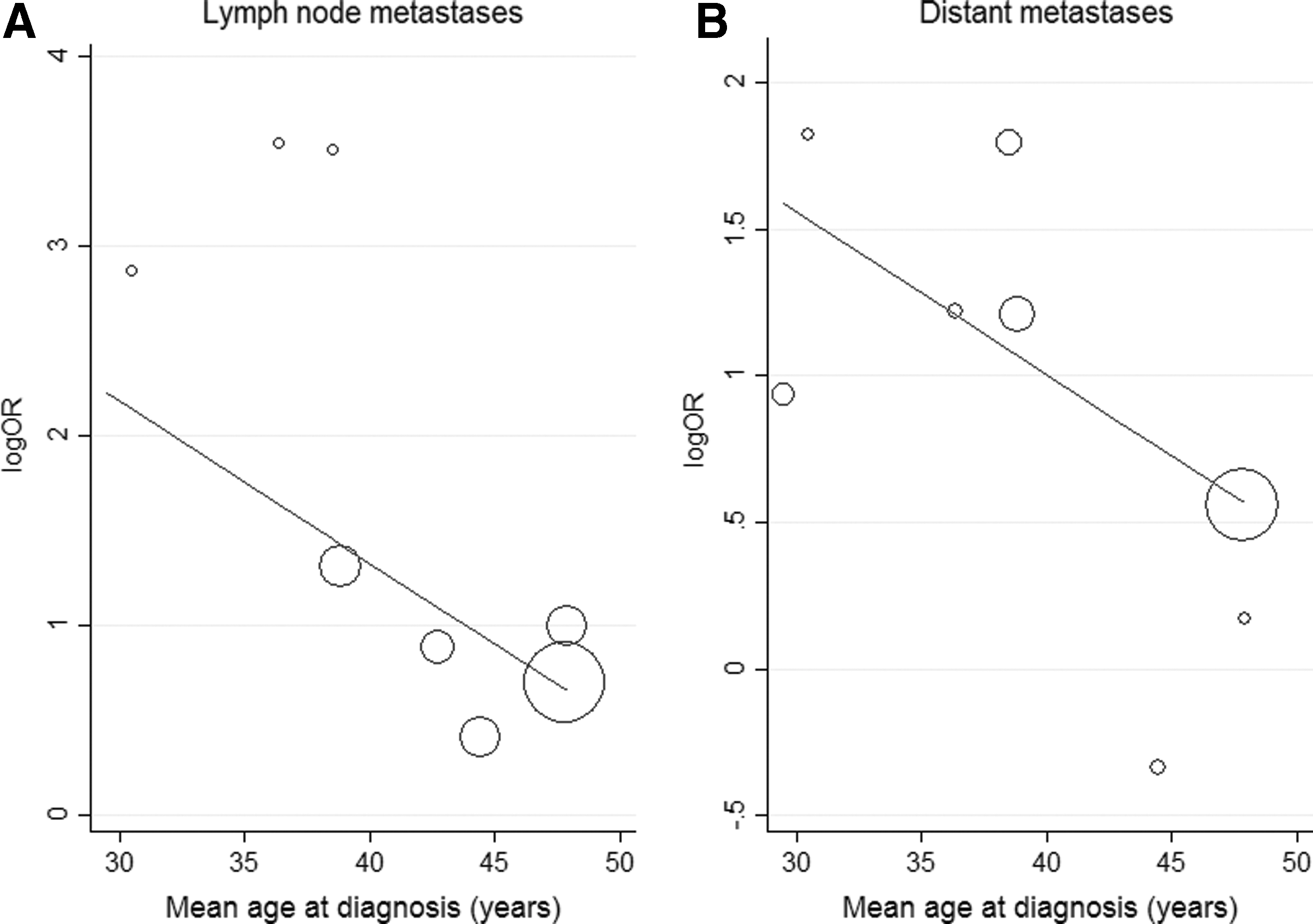
Bubble plot for meta-regression analysis between age and logOR of lymph node (
Meta-analysis of outcome in DSV versus cPTC
Data on recurrent and persistent disease were available for 7/10 studies. Patients with DSV were at higher risk of persistent/recurrent disease (OR = 3.19 [CI 1.86–5.49]; Fig. 5). When the analysis was carried out stratifying for 131I treatment (selective vs. routine post-surgical 131I administration), the risk of persistent/recurrent disease was higher in patients with DSV who did not receive routine 131I treatment (OR = 5.09 [CI 2.91–8.90]), whereas the risk was not significantly different when patients routinely received post-surgical 131I treatment (OR = 2.07 [CI 0.88–4.90]).
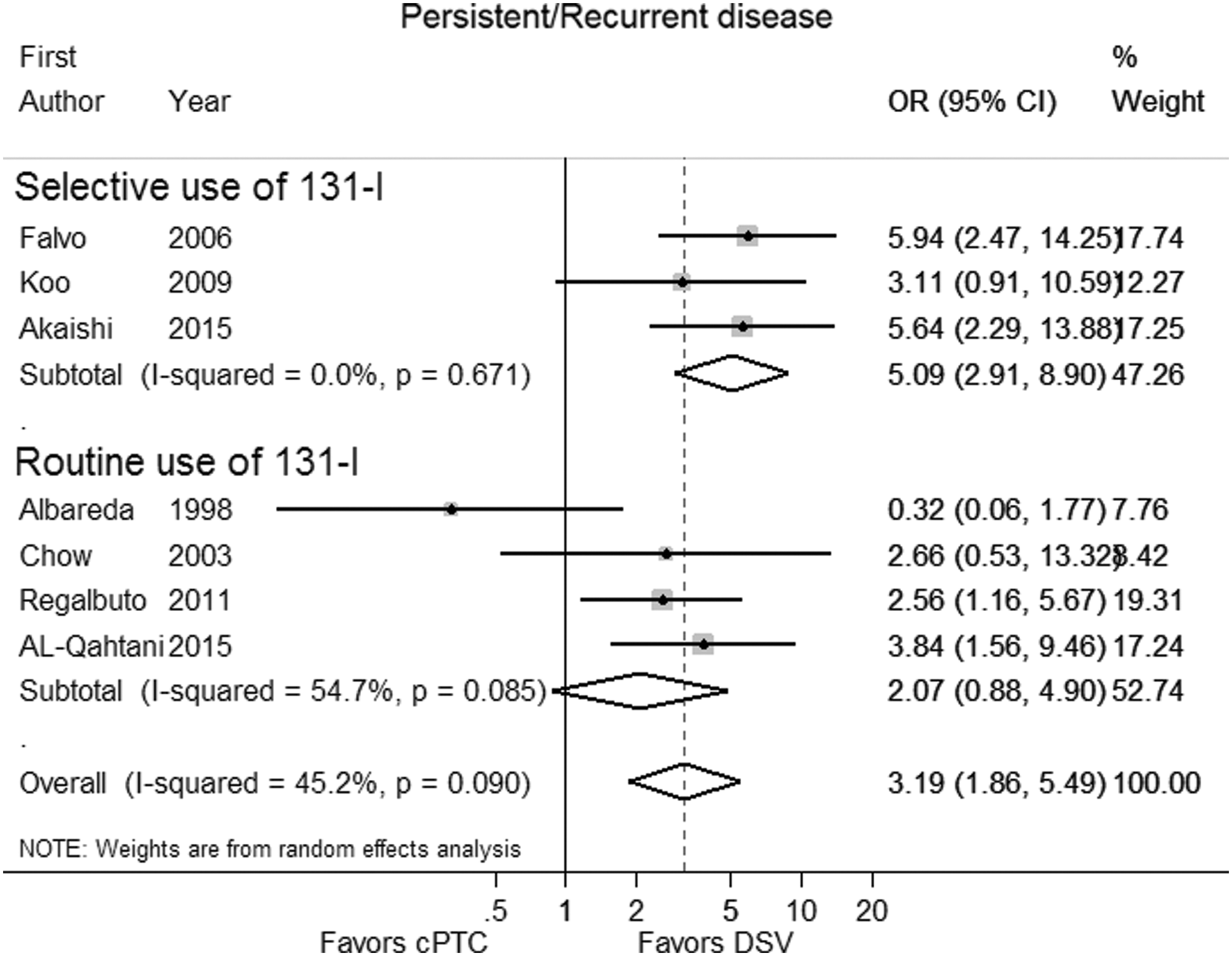
Forest plots of OR for recurrent/persistent disease associated with papillary thyroid cancer, cPTC versus DSV. Routine use of 131I therapy results in not different OR of recurrent/persistent disease between DSV and cPTC patients. Squares and lines indicate the same parameters as in Figure 3.
Data on cancer-related death were available in 6/10 studies analyzed. Three additional studies of the 10 considered were included in the analysis after continuity correction, as described in the Methods. Therefore, overall, nine studies were available for mortality analysis. The risk of mortality was not significantly different between DSV and cPTC patients (OR = 1.34 [CI 0.76–2.38]; Fig. 6). Similarly, the risk of mortality was not different when post-surgical 131I was administered either selectively (OR = 1.41 [CI 0.76–2.62]) or routinely (OR = 1.05 [CI 0.24–4.65]).
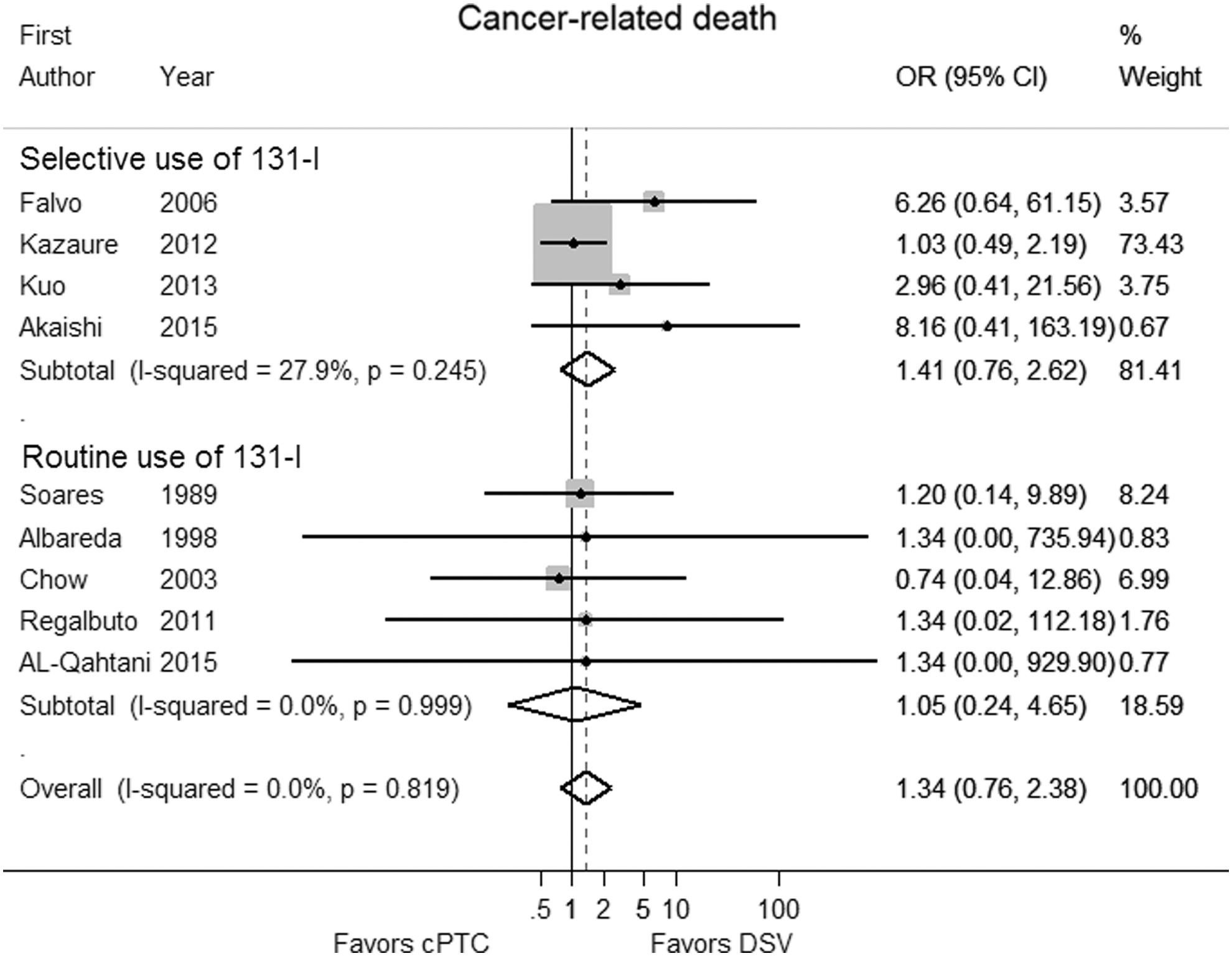
Forest plots of OR for cancer-related death associated with papillary thyroid cancer, cPTC versus DSV. Squares and lines indicate the same parameters as in Figure 3.
By using the meta-regression analysis, no significant association was observed between persistent/recurrent disease or cancer–related death and several covariates, including mean age at diagnosis, percentage of male patients, percentages of patients with multifocality, extrathyroidal extension, lymph node and distant metastases, and percentages of patients who underwent total thyroidectomy, lymph node excision, and post-surgical radioiodine therapy.
Sensitivity analyses
Using a sensitivity analysis to evaluate the influence of omitting individual studies, no relevant change of the pooled ORs was observed. The resulting ORs ranged from 2.78 [CI 1.51–5.13] to 3.91 [CI 2.63–5.81] for persistent/recurrent disease and from 1.15 [CI 0.61–2.18] to 2.32 [CI 0.88–6.15] for cancer-related death.
Discussion
Papillary thyroid cancer has a good prognosis, and surgery either alone or followed by radioiodine therapy is effective in most cases to cure even those patients with advanced disease at diagnosis. The aggressive histological variants of PTC are not common but are frequently associated with less favorable outcomes. However, existing data on the outcomes of patients with aggressive variants of PTC are controversial because published studies comparing patients with these aggressive variants with patients with classic PTCs are often retrospective analyses of small series of patients treated and followed up with different protocols.
DSV is a rare variant of PTC with well-defined histological features, and is commonly considered more aggressive than cPTC. This study reviewed the pathological characteristics at diagnosis and the outcome of DSV and cPTC patients by performing a meta-analysis of 10 studies examining a total of 585 DSV patients and evaluating the outcome in terms of persistent/recurrent disease and cancer-related death.
In the selected studies, the patients with DSV were younger than the patients with cPTC: the age at diagnosis ranged from 23 to 48 years for DSV and from 33 to 48 years for cPTC. This is not surprising, given that DSV is considered a frequent variant of PTC in young patients and that the median age at diagnosis is often in the third decade of life (20,22). The present analysis also confirms that DSV is associated with an advanced stage of the disease at diagnosis, as evidenced by a higher rate of extrathyroidal extension and lymph node and distant metastases compared with cPTC. Multifocality was not more frequent in DSV thyroid cancer patients, probably because this variant is characterized by diffuse involvement of the thyroid gland, without one or more dominant localized lesions (23). Interestingly, DSV in younger patients was associated with a higher risk of local and distant metastases (Fig. 4), a common behavior of thyroid cancer occurring at a young age that is characterized by extensive disease at clinical presentation (24).
On the basis of these clinical characteristics at presentation, patients with DSV should first undergo extensive surgery, including both total thyroidectomy and lymph node excision. This surgical approach may be planned during the presurgical assessment because the diagnosis of DSV should be suspected in a young patient with the typical ultrasound aspect referred to as “snowstorm appearance” (23) and the typical cytological features at fine-needle aspiration biopsy characterized by lymphocytes intermingled with nests of tumor cells, psammoma bodies, and squamous differentiation (25).
The present meta-analysis indicates that the features of aggressiveness observed at presentation in DSV patients are associated with a higher risk of persistent/recurrent disease during follow-up. The risk of recurrence or persistent disease was three times greater in DSV than it was in cPTC patients. None of the clinical or pathological features evaluated in the meta-regression analyses were significantly prognostic for the disease status during follow-up, and only the stratified analysis regarding radioiodine administration (selectively vs. routinely) demonstrated benefits for patients who were routinely treated with 131I (Fig. 5). These findings should support the routine use of 131I for the post-surgical management of patients with DSV, although the latest guidelines of the ATA (10) consider patients with DSV at intermediate risk of recurrence and therefore with a weak evidence for benefit from adjuvant therapy with 131I. In contrast, the Latin American Thyroid Society (LATS) guidelines consider all patients with aggressive histological variants at high risk of recurrence, and recommend the ablation of thyroid remnants in these patients (26). In high-risk PTC patients, classified according to the ATA or the LATS risk-stratification system, a different rate of persistent disease (both biochemical and structural disease) is reported after initial therapy: 59% versus 30%, respectively (27). In the studies selected for the present meta-analysis, the overall mean rate of persistent/recurrent disease was 28.4%, a value similar to that reported when using the LATS system. The different occurrence rates according to the two risk-assessment systems is mainly due to the higher rate of incomplete structural response to treatment in patients classified at high risk according to the ATA criteria. Indeed, this subgroup of patients mainly includes subjects with a relatively low probability of complete response to initial therapy (i.e., patients with distant metastases, incomplete tumor resection, or massive lymph node involvement).
In the present meta-analysis, mortality data were not different in DSV and cPTC patients. In their 35-year single-institution study, Lam and Lo (6) reported similar survival rates in patients with DSV and cPTC. Therefore, it is plausible that patients with DSV, despite having a more advanced disease at presentation, respond positively to treatment (including both surgery and 131I) because this histological variant typically occurs in young patients who, even in the case of persistent disease, usually have a more favorable outcome compared with older patients with persistent PTC (10). A better outcome was reported in patients with distant metastatic disease when the lungs were the only involved organ (28), and this may also explain why the mortality risk between DSV and cPTC is not different. In fact, the lungs were the predominant site of metastatic disease in the studies selected in this meta-analysis. A mortality rate similar to cPTC could also be explained by the mean length of follow-up (<10 years in almost all studies selected), a period that may not be sufficiently long for evaluating survival in thyroid cancer.
The major limitation of this meta-analysis is the relatively small number of studies included and their retrospective design. Moreover, this study provides no answer to the question of whether the high risk of recurrence of DSV patients is primarily due to the intrinsic biological behavior of this variant or to the frequent association with features indicating a more advanced cancer at presentation. The former hypothesis is more likely based on the observation that the diagnosis of DSV was an independent factor associated with poor outcome (in terms of either recurrence or death), as indicated in 4/10 studies selected in the meta-analysis (12,16,17,19). A different biological behavior from cPTC may also be secondary to the different molecular characteristics of DSV. When compared with cPTC, DSV is characterized by a higher occurrence of RET/PTC rearrangements and a lower rate of BRAF mutations (22).
To summarize, DSV patients present more unfavorable features at diagnosis and have more frequently persistent/recurrent disease during follow-up than patients with cPTC do. However, these unfavorable characteristics are not associated with a higher rate of mortality in the short or medium term, reflecting a good response to treatment. The analyzed data indicate that DSV should be considered a high-risk PTC, and treatment and follow-up strategies should be performed accordingly.
Footnotes
Acknowledgments
This work was supported by grants from the Associazione Italiana per la Ricerca sul Cancro (AIRC, Milan, Italy) to R.V.
Author Disclosure Statement
The authors declare that no competing financial interests exist.