
Abstract
Background:
Because of their increased need for iodine, pregnant women are among the high-risk groups for iodine deficiency. The purpose of this study was to evaluate the effectiveness of an educational program on the iodine nutrition status of pregnant women.
Methods:
In this randomized controlled trial, 100 pregnant women were randomly selected from five healthcare centers in the southern region of Tehran, the capital of Iran. In the intervention group, pregnant women received a four-month educational program, which included two face-to-face educational sessions, using a researcher-designed educational pamphlet in the second and third trimesters, and two follow-up telephone calls. Knowledge, attitude, and practice (KAP) scores, urinary iodine concentration (UIC), and salt iodine content were assessed at baseline and four months after the intervention.
Results:
At baseline, there were significant associations between knowledge and attitude (r = 0.38, p = 0.03) between practice and UIC (r = 0.28, p = 0.01) and between UIC and iodine content of salt (r = 0.24, p = 0.009). Although a significant difference was found in mean KAP scores between the two groups after the educational intervention, scores were significantly higher in the intervention group compared with controls (p < 0.01). There were no significant differences in UIC and iodine content of salt between the two groups at follow-up.
Conclusions:
Despite educational intervention increasing KAP among women regarding the importance of iodine and iodized salt consumption during pregnancy, their iodine status did not improve. Considering the main socio-environmental determinants of iodine deficiency, in particular, the monitoring of salt fortification, prescribing iodine containing supplements as well as improving health literacy in pregnant women seem essential strategies.
Introduction
I
The results of some educational programs show improvement in individuals' knowledge, attitude, and practice (KAP) on their health and nutrition status (11 –13). A body of evidence from some countries such as South Africa, Ethiopia, India, Nigeria, and Australia shows that lack of educational programs, poor knowledge, and inappropriate practices regarding the importance of iodine, dietary iodine sources, and consequences of iodine inadequacy are associated with iodine deficiency in these countries (2,14 –20). On the other hand, a mass media campaign regarding iodized salt among Turkish women had a positive impact on knowledge and consumption of iodized salt (21). In addition, the results of an educational program on iodized salt consumption circulated via daily text messaging had beneficial effects on improvement of knowledge and attitude scores (22).
In the 1960s, IDDs such as goiter were endemic in Iran, and years later, universal salt iodization programs were begun. Simultaneously, public health education programs regarding IDD and iodized salt utilization were conducted by health workers in healthcare centers, resulting in increased awareness among individuals and majority of households using iodized salt. Consequently, national surveys in 1989, 1996, 2001, and 2007 showed Iran to be free of IDD (23,24). Since then, there has been little or no health education advocacy of iodine consumption (22). In a recent study conducted in Iran, it was found that content of salt iodine and urinary iodine concentration (UIC) levels had declined in Iranian populations compared with previous findings, and their KAP regarding iodized salt consumption were moderate. In addition, there was a significant association between inappropriate practices and mild iodine nutrition insufficiency among Tehranian women (25,26).
According to recent data, one third of pregnant Tehranian women had iodine deficiency in the first trimester, a proportion that could increase twofold by the end of pregnancy (27). The first national survey conducted in 10 provinces of Iran by Delshad et al. showed that the median UIC of pregnant Iranian women is <100 μg/L, indicating that despite iodine sufficiency of the general population, pregnant Iranian women have moderate iodine deficiency (28). Therefore, given the importance and effectiveness of education on the health and vitality of iodine adequacy during pregnancy, the aim of the present study was to evaluate the effectiveness of an educational program regarding the importance of iodine during pregnancy in enhancing the KAP of pregnant women and improving their iodine nutrition status.
Materials and Methods
Sample size
With respect to the expected mean difference (Δμ = 12 μg/L) for UIC before and after the educational program in the intervention group (based on median UIC among Iranian pregnant women: 87.3 μg/L) (23), power = 1 – β = 0.90, α = 0.05, and accounting for an attrition rate of 25%, 50 participants in each group would be required to be recruited in the study.
Subjects
In this randomized controlled trial conducted in the southern region of Tehran from February 2014 to January 2015, among eligible pregnant women referred to five healthcare centers, 100 mothers participated in the current study. Inclusion criteria were being between 4 and 18 weeks pregnant, no history of thyroid diseases (goiter or hypo- or hyperthyroidism), and providing informed consent. Exclusion criteria were having any thyroid diseases during pregnancy and premature labor. As a first step, the purpose and methodology of the study were explained by the main researcher, following which pregnant women were invited to participate. At baseline, demographic characteristics including age, gestational age, education level, gravidity, parity, use of iodine-containing supplements, and a history of abortion were documented using an interviewer-administered questionnaire. Eligible women signed an informed consent form, and the ethical committee of the Research Institute for Endocrine Sciences (RIES) approved the study.
In each healthcare center, pregnant women were allocated 1:1 to intervention and control groups (n = 50 in each group) using a random-number table. Randomization was conducted by a researcher not directly involved in data collection. For equal allocation to two groups, the direction to read the table was predetermined to the right, and an arbitrary starting point was selected. Then, the researcher equated the odd and even numbers to the intervention and control groups, respectively. The control group received the education usually provided in healthcare centers. In the intervention group, the educational program lasted for four months, and included two face-to-face educational sessions using a researcher-designed educational pamphlet in the second (30–60 minutes) and the third (20–30 minutes) trimesters. In addition, two follow-up telephone calls were made between educational sessions to answer any questions the mothers may have had (Table 1). The program mainly focused on essential information regarding the definition and consequences of iodine deficiency in pregnant women and their children, and the importance of iodine and iodized salt and its optimal storing methods. This clinical trial was registered in the Iranian registry of Clinical Trials (
Urine and salt samples collection
At baseline and follow-up visits, two tablespoons of salt samples used during cooking and/or as table salt were collected from each of the pregnant women. The samples were kept in lightproof, closed plastic cans and labeled with the code allocated to each woman. In addition, urine samples from both groups were collected in healthcare centers and transferred in screw-topped labeled plastic vials to the iodine laboratory of the RIES, the Shahid Beheshti University of Medical Sciences, and to the Reference Laboratory for the Eastern Mediterranean Region. The urine samples were kept frozen at −80°C until iodine measurement.
Laboratory measurements
The iodine content of the salt samples was determined using the iodometric titration method with 1 ppm sensitivity and 1% coefficient of variation. Values obtained are reported in parts per million. Iodine concentrations in urine samples were analyzed using the Sandell–Kolthoff (acid digestion) reaction, and results are expressed as micrograms of iodine per liter of urine. Intra-assay coefficients of variation at UIC values of 8.5, 17.5, and 36.0 μg/L were 8.5%, 6.2%, and 8.0%, respectively. The inter-assay coefficients of variation at concentrations of 8.5, 17.4, and 36.4 μg/L were 10.3%, 9.7%, and 8.0%, respectively.
KAP scores
The current study used the KAP questionnaire regarding the importance of iodine nutrition and use of iodized salt due to this being the only main dietary iodine source in all age groups in Iran. KAP was designed based on a review of the literature from national and international resources. This questionnaire, applied for assessing KAP scores in pregnant women, as well as women of child-bearing age (26), includes 24 items that contain knowledge (10 items), attitude (8 items), and practice (6 items) sections. Face validity was confirmed by 10 women who completed the questionnaire assessing their awareness levels on the importance of iodine consumption in their daily lives. An expert panel of 10 specialists in health education, endocrinology, nutrition, and sociology evaluated the KAP questionnaire and confirmed its content validity. Cronbach's alpha was determined for internal consistency of the questionnaire (Cronbach's α = 0.83). In the knowledge section, each yes (“true”), don't know, and no (“false”) answer received 2, 1, and 0 points, respectively. The attitude section was evaluated based on Likert criteria (0 = “completely disagree” to 4 = “completely agree”). Each question in the practice section scored one point. KAP variables were scored on a scale of 1–100 for uniformity of scales.
Definition of terms
According to criteria of the World Health Organization (WHO), the International Council for the Control of Iodine Deficiency Disorders (ICCIDD), and the United Nations Children's Fund (UNICEF), median UICs <150 and ≥150 μg/L represent iodine insufficiency and sufficiency in pregnancy, respectively (29).
Statistical analysis
Frequency distribution, mean ± standard deviation (SD), and median (interquartile range [IQR]) were reported according to the type of study variables. The chi-square test was used for qualitative variables. The assumption of normality for continuous variables was checked using the Shapiro–Wilk test. Basic categorical and continuous variables between the two groups were compared using the chi-square and Mann–Whitney U-test. The Wilcoxon signed rank test was used to compare baseline and follow-up measures for each group. Differences between the two groups for changes between baseline and follow-up in the continuous measures were compared using the Mann–Whitney U-test. Using Structural Equation Modeling (SEM), the path analysis method was utilized to test the interrelationship of KAP scores with UIC and the iodine content of salt. The hypothesized model is displayed in Figure 2. The maximum likelihood method was used to estimate path coefficients (β), and the bootstrap confidence interval (CI) was calculated using the “Bias-corrected percentile method.” Model fit indexes, including chi square, the ratio of chi square to degrees of freedom, comparative fit index (CFI), root mean square error of approximation (RMSEA), normed fit index (NFI), goodness of fit index (GFI), and incremental fit index (IFI), were calculated, and their acceptable levels were considered (30). The SEM model was conducted using IBM SPSS Statistics for Windows and AMOS v22 (IBM Corp., Armonk, NY).
Results
One hundred eligible pregnant women were randomly allocated into intervention and control groups (n = 50 in each group). Two months after educational intervention, the two groups were followed by the main researcher. In the intervention group, eight participants were excluded due to unexpected abortion, traveling, or refusing to participate in the study. In the control group, five participants were excluded for the above-mentioned reasons. Both study groups were followed for the next four months, during which 13 and 11 individuals were excluded from the intervention and control groups, respectively. Premature labor, traveling, or refusing to participate in the study were the main reason of exclusion. Finally, complete data of 29 and 34 individuals in the intervention and control groups respectively were analyzed (Fig. 1).
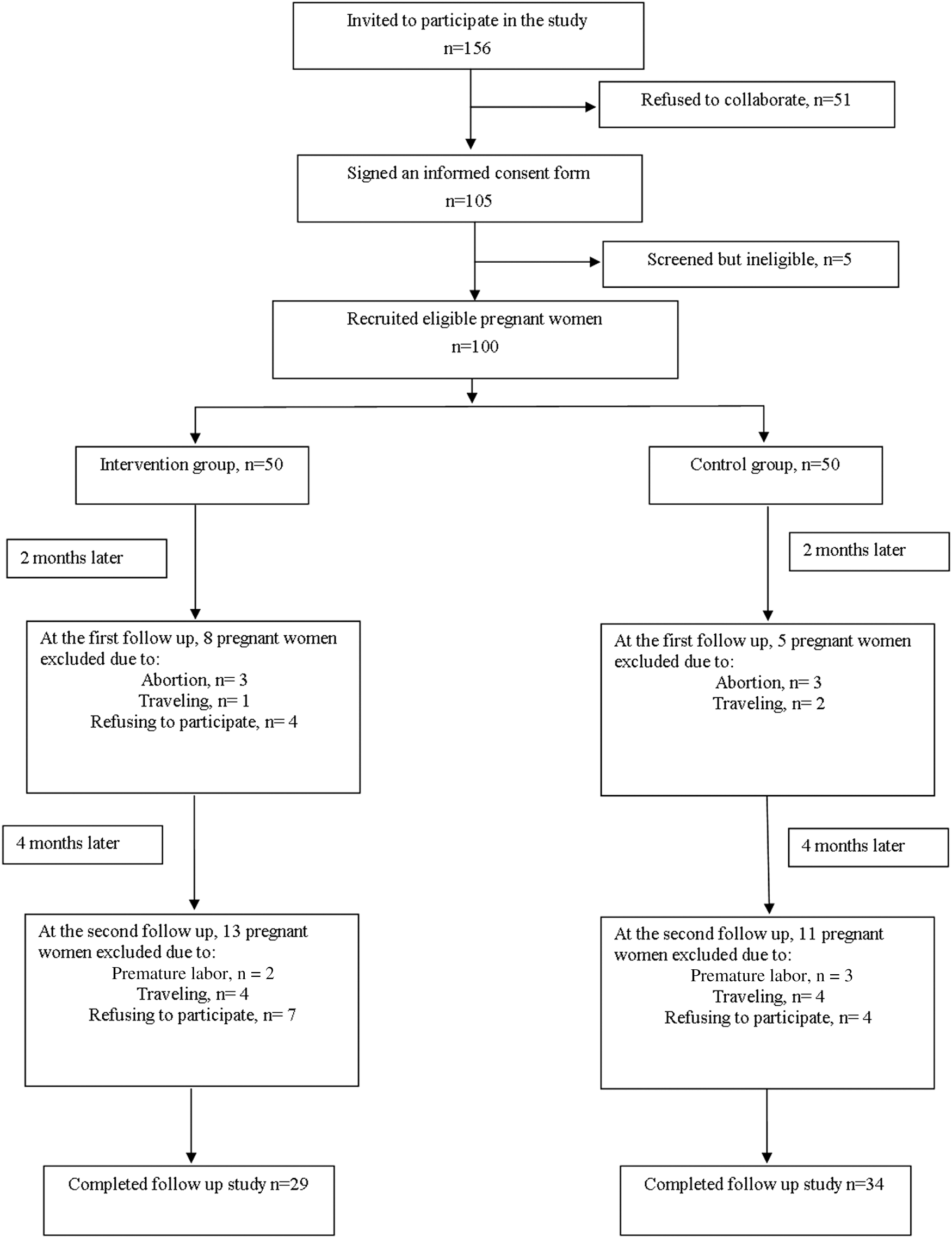
The subject sampling frame of the study.
At baseline, there were no significant differences in age, education levels, gravidity, parity, and history of abortion between respondents and non-respondents. However, a significant difference was observed in use of iodine-containing supplements between these two groups. In the control group, although no differences were observed in baseline characteristics between respondents and non-respondents, significant differences were found in the history of abortion and the use of iodine-containing supplements between these two groups in the intervention group. In addition, baseline characteristics of respondents as well as non-respondents did not differ significantly between control and intervention groups (data not shown).
Baseline characteristics of the intervention and control groups are reported in Table 2. Mean ± SD for age and gestational age were 27.2 ± 5.6 years and 12.5 ± 2.7 weeks, respectively. Less than half of the women (41%) had high school education levels, and 78% had multigravidity. In total, 48% of participants had one child, and 15% had a history of abortion. Only 10% of pregnant women used vitamin/mineral supplements containing 150 μg of iodine. There was no difference in the mean ± SD age between the intervention and control groups (26.3 ± 5.7 vs. 28.0 ± 5.3 years, respectively). Other demographic variables (gestational age, education level, gravidity, parity, use of iodine-containing supplement, and history of abortion) did not differ significantly between the two groups.
The baseline and follow-up values for KAP scores, iodine content of salt, and UIC in the intervention and control groups are reported in Table 3. At baseline, the mean ± SD KAP scores were 62.1 ± 19.9 (K), 84.8 ± 13.4 (A), and 65.7 ± 12.8 (P), respectively, in the intervention group. In the control group, the mean ± SD KAP were 62.7 ± 21.9 (K), 85.4 ± 11.0 (A), and 63.7 ± 15.7 (P), with no statistically significant difference between knowledge (p = 0.88), attitude (p = 0.80), and practice (p = 0.48) between the two groups. At baseline, the median (IQR) UIC was 112.0 μg/L (63.0–185.0 μg/L) in the intervention group and 110.0 μg/L (61.0–152.0 μg/L) in the control group, with no statistically significant difference (p = 0.61) between these groups. Median (IQR) salt iodine content was 26.4 ppm (14.5–29.6 ppm) in the intervention group and 25.4 ppm (22.2–30.2 ppm) in the control group, indicating no statistically significant difference between the two groups (p = 0.98). At baseline, there were significant associations between knowledge and attitude (r = 0.38, p = 0.03), between practice and UIC (r = 0.28, p = 0.01), and between UIC and salt iodine content (r = 0.24, p = 0.009).
Data shown as mean ± SD.
Data shown as median (interquartile range [IQR]).
UIC, urinary iodine concentration; ppm, parts per million; SD, standard deviation.
At follow-up, mean ± SD KAP scores were 97.9 ± 4.9 (K), 98.3 ± 4.0 (A), and 87.5 ± 14.0 (P) in the intervention group. In the control group, mean ± SD KAP scores were 72.9 ± 22.9 (K), 90.5 ± 10.6 (A), and 71.5 ± 17.3 (P), respectively. Statistically significant differences were found in KAP scores between the intervention and control groups at follow-up (p < 0.01). Median UIC was 121.0 μg/L (50.0–190.0 μg/L) in the intervention group and 78.0 μg/L (36.0–156.0 μg/L) in the control group. The iodine content of salt was 28.6 ppm (22.8–32.8 ppm) in the intervention group and 26.1 ppm (21.0–32.1 ppm) in the control group. At the end of the study, no significant differences were observed in UIC and iodine content of salt between the two groups. In addition, there was no change in percentage of prenatal supplements containing 150 μg of iodine used in the intervention or control group over the course of follow-up. At follow-up, there were significant associations between knowledge and attitude (r = 0.60, p < 0.01), between knowledge and practice (r = 0.41, p < 0.01), between practice and attitude (r = 0.50, p < 0.01), and between UIC and the iodine content of salt (r = 0.37, p < 0.01).
In both the intervention and control groups, significant increases were found in KAP scores, although no significant increases were found in UIC and the iodine content of salt between baseline and follow-up (Table 3). Compared with baseline values, at follow-up, the educational program increased KAP scores (p < 0.001) significantly. However, it did not affect median UIC (p = 0.37) and salt iodine content (p = 0.71) in the intervention group.
Figure 2 shows the hypothesized path model and determinants of iodized salt and urinary iodine status; fit indexes reported below Figure 2 indicate the acceptable range. Based on estimated path coefficients and their bootstrapping CI, the iodine content of salt (β = 0.31 [CI 0.04–0.33]) and practice (β = 0.24 [CI 0.04–0.34]) had a significant direct effect on urine iodine status. The correlation between knowledge and attitude was significant (r = 0.36 [CI 0.17–0.52]). Because of non-significant correlations between knowledge–practice and between attitude–practice, their association pathways were excluded from the model, which resulted in the improvement of model fit indexes compared with their presence. No direct effect was observed in KAP levels on the iodine content of salt, indicating that the iodine content of salt does not play a mediator role for the effect of KAP on UIC.
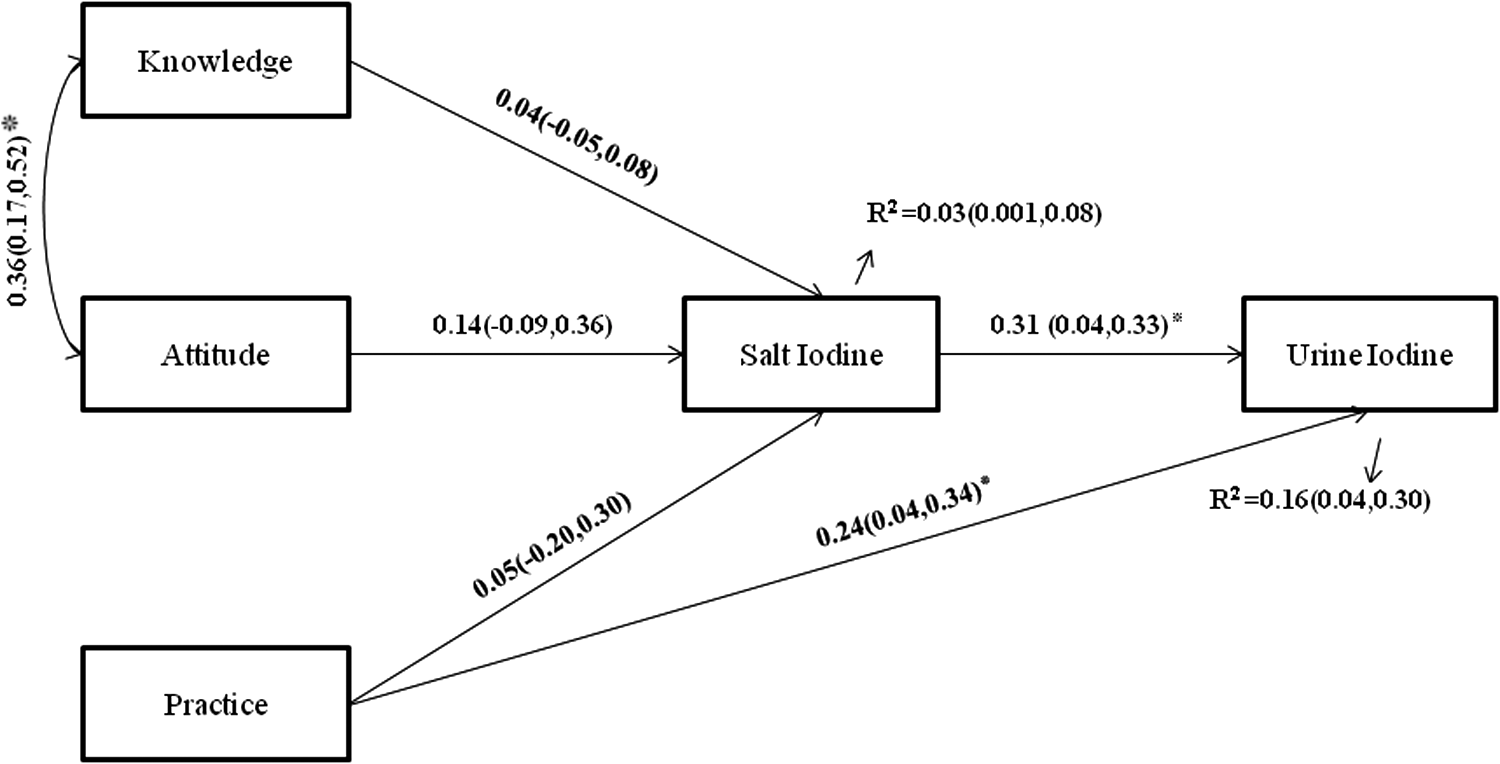
Hypothesized path model for testing association between knowledge, attitude, and practice (KAP), urinary iodine concentration (UIC), and iodine content of salt. Standardized estimations for path coefficients with bootstrapping confidence interval were shown. Important fit indexes of hypothesized model: χ2 = 4.11, df = 4, χ2/df = 1.03, RMSEA = 0.017, NFI = 0.99, CFI = 0.99, IFI = 0.99, RMR = 0.15, GFI = 0.98. *p < 0.01.
Discussion
The present trial was conducted to evaluate the effect of an educational program on providing iodine nutrition adequacy among pregnant Tehranian women. The results reveal that study participants suffer from mild iodine deficiency. Compared with the control group, pregnant women who participated in the educational program had more positive attitudes as well as higher levels of knowledge and practice. However, despite improvements in UIC and the iodine content of salt in the intervention group, the difference was not significant compared to the control group. In both study groups, UIC levels were below the recommended range for pregnant women.
Health education during pregnancy provides essential information to promote maternal and fetal health and to address problems encountered during pregnancy (31,32). Based on knowledge, no educational program regarding the importance of iodized salt consumption in pregnant women has hitherto been implemented in Iran. The results of two previous studies conducted in Tehran demonstrated poor knowledge and inappropriate practices among individual regarding iodized salt consumption (33,34). Accordingly, public health educational programs regarding the importance of IDDs and iodized salt consumption conducted by health workers in healthcare centers resulted in increased public awareness regarding the importance of iodine deficiency, as well as approximately 80% of households using iodized salt (24,26). Evidence reveals an improvement in iodine-related KAP via mobile text messages among Tehranian women (22). Consistently, although the current educational program had significantly higher effects on mothers' knowledge and attitudes, and in particular on their practices, compared with controls, significant improvements in KAP scores have also been observed in the control group. This can be explained by the following reasons. First, all Tehranian pregnant women receive some information regarding iodine intake through their routine prenatal care in the public health centers. Hence, some improvement of KAP scores in the control group would be expected. Second, due to high sensitivity of pregnant women, it is reasonable that explaining the current research program, followed by obtaining the salt and urine samples, and particularly completion of KAP questionnaires through pretest evaluation makes them more sensitive to the subject, and this may result in obtaining more information. However, similar to results reported by Mehran et al. (22), this study shows that iodine status of participants was not significantly improved after education as initially hypothesized.
Existing data show that increasing knowledge and positive attitude does not necessarily lead to accomplishment of targeted healthy behaviors (26,35 –37), findings implying that beyond personal characteristics, different interpersonal, cultural, and environmental factors can negatively or positively affect individuals' nutritional patterns (38 –41). Furthermore, for iodine nutrition adequacy, the iodine content of salt should be within the recommended range of 20–40 ppm. Therefore, the adequate amount of iodine for a pregnant woman can only be ensured by a daily intake of 6 g of 40 ppm iodized salt. The results indicate that despite pregnant women reporting adequate intakes of iodized salt, the iodine content of salt consumed was closer to the lower recommended limit of 20 ppm. In agreement with previous studies (25,42), the illegal production and distribution of less-expensive non-iodized or inadequately iodized brands of salt could be a major contributor to the lack of association between practices and iodine content of salt found in this study. On the other hand, it appears that pregnant Tehranian women receive contradictory/mixed messages regarding salt consumption from various social media. To assure adequate iodine intake, they were encouraged to consume iodized salt as the only main dietary iodine source. However, they were also advised to reduce salt intakes to prevent hypertensive disorders during pregnancy. Hence, this discrepancy may result in confusion among pregnant women, and they are faced with making difficult decisions.
Path analysis indicates that there was a weak but significant positive association between iodine content of salt and maternal UIC. As shown in this study, data available from countries where iodized salt is the main dietary iodine source (43,44) reveal that the iodine requirements of the most susceptible groups (i.e. pregnant women and lactating mothers) are not always adequately met by iodized salt. In this regard, the European Thyroid Association (ETA), the American Thyroid Association (ATA), and the Endocrine Society (ES) recommend that besides universal salt iodization programs, additional complementary strategies such as iodine supplementation with 150 μg of iodine in daily prenatal vitamin/mineral supplements be considered to ensure optimal iodine nutrition for these groups (45 –47). However, in Iran, there is a lack of emphasis on using iodine supplemented multivitamin and/or mineral tablets during pregnancy and lactation in addition to the longstanding, well-established universal salt iodization program.
In summary, this study aimed to evaluate the effect of an educational program on the iodine status of Tehranian pregnant women. Furthermore, associations among mothers' KAP scores, iodized salt content, and UIC were assessed via path analysis. Due to significant daily variations in UIC, using a single random urine sample to determine an individual's iodine status can be considered a limitation of this study. The results show that despite the positive effect of the educational program on iodine intake–related KAP scores in pregnant women, it did not have a significant positive effect on iodine status as initially hypothesized. The current findings emphasize the necessity of adopting a comprehensive approach to plan health promotion programs aimed at improving iodine status during pregnancy. Considering the main socio-environmental determinants of iodine deficiency, essential strategies particularly include monitoring of salt fortification, prescribing iodine containing supplements, as well as improving health literacy in pregnant women.
Footnotes
Acknowledgments
The study was supported by financial grants from the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We would like to thank the laboratory personnel of the Endocrine Research Center at Shahid Beheshti University of Medical Sciences for their assistance. We wish to acknowledge Ms. Niloofar Shiva for critical editing of the English grammar and syntax of the manuscript.
Author Disclosure Statement
None of the authors has any personal or financial conflicts of interest to declare.