
Abstract
Background:
This study aimed to establish the changes in the incidence and characteristics of iodine-induced hyperthyroidism (II-Hyper) and iodine-induced hypothyroidism (II-Hypo) in the two-year period before and the 10-year period after the increase in mandatory salt iodization from the previous 10 mg/kg of potassium iodide to 25 mg/kg in 1999. Furthermore, the aim was to determine the duration of treatment in II-Hyper patients, since no data regarding severity and treatment of II-Hyper with respect to iodine supply are available.
Methods:
This retrospective study reviewed medical records of 885 Slovenian patients first diagnosed with II-Hyper or II-Hypo between 1998 and 2009 at the Thyroid Department of the University Medical Centre Ljubljana. II-Hyper and II-Hypo were diagnosed by one out of 10 senior internal medicine specialists. The diagnosis was based on an adequate patient history, and laboratory measurements of thyrotropin, thyroid hormones, and thyroid antibodies. In most cases, thyroid ultrasound and thyroid scintigraphy were performed. Demographic characteristics and the type and the duration of treatment were also reviewed.
Results:
The incidence of II-Hypo was significantly higher after the increase in iodine supply than it was before (p < 0.001). After the increase in iodine supply, the incidence of II-Hyper was significantly lower than before the increase (p < 0.001). Furthermore, the portion of patients with overt hyperthyroidism decreased, predominantly due to the increased proportion of patients with subclinical hyperthyroidism (p = 0.007 and p = 0.015, respectively). The duration of treatment with antithyroid drugs and perchlorate was significantly shorter after the increase in iodine supply than it was before (p = 0.001 and p = 0.002, respectively). A significantly positive correlation between the year of the occurrence of excessive iodine intake (EII)-induced thyroid disease and the duration of treatment with amiodarone was found (R = 0.132; p = 0.048), suggesting that the longer the patients had an adequate iodine supply, the longer they could take amiodarone before EII-induced thyroid disorder developed.
Conclusions:
After the increase in iodine supply, a higher incidence of II-Hypo and a lower incidence of II-Hyper were observed than before the increase. Less severe II-Hyper, shorter duration of treatment of II-Hyper, as well as a longer thyroid disease-free period in patients on amiodarone are additional beneficial clinical consequences after the establishment of an adequate iodine supply.
Introduction
T
Excessive iodine intake (EII) should be considered when urinary iodine concentration is >300 μg/L (6). Individuals with a healthy thyroid gland can tolerate a daily intake of a few grams of iodine. However, in predisposed individuals or in patients with thyroid disorders, such an intake can cause or worsen thyroid disease. Most frequently, iodine-induced hyperthyroidism (II-Hyper) and iodine-induced hypothyroidism (II-Hypo) are caused by the antiarrhythmic drug amiodarone or by iodine-containing contrast media (ICCM). Rarely, they can be provoked by iodine-containing vitamin supplements (7,8). Amiodarone is structurally similar to thyroid hormones and has a half-life of 30–84 days (8,9). One 200 mg tablet of amiodarone contains 75 mg of iodine (10). ICCM, on the other hand, are predominantly water-soluble and are quickly eliminated from the body through renal clearance. Nevertheless, 100 mL of iomeprol-300 contains 30 g of iodine, which is bound to organic molecules. After the application, up to 6 mg of free iodine can be released from the organic molecules per hour (7).
Two types of II-Hyper have been described. Type 1 II-Hyper is more frequently present in areas with deficient iodine supply, and usually occurs in patients with underlying subclinical Graves' disease or subclinical thyroid autonomy. Type 2 II-Hyper is more common in areas with adequate iodine supply—pathogenetically, it is a destructive thyroiditis, for example caused by amiodarone (11 –13). Due to the different underlying mechanisms, the treatment of each type is different. Type 1 is treated with high doses of antithyroid drugs and, in some cases, with perchlorate, while in type 2, glucocorticoids are used (9). Thyroidectomy may be performed as a definitive treatment of II-Hyper (9).
Although not completely understood, II-Hypo may be caused by impaired autoregulation, as well as by complex effects of iodine on the exacerbation or deterioration of autoimmune thyroid disease (8,13 –15). Treatment of II-Hypo is the same as in other types of hypothyroidism, (i.e., supplementation with levothyroxine).
Data on the occurrence of thyroid disorders due to EII with respect to iodine supply are scarce. In general, in areas with deficient iodine supply, EII more frequently provokes hyperthyroidism and less frequently hypothyroidism compared with the areas with adequate iodine supply and vice versa (14,16). To support this claim, two similar studies were performed regarding the occurrence of II-Hyper and II-Hypo in patients treated with amiodarone. In the United States, which is an area with adequate iodine supply, II-Hypo occurred in 22–30% of patients taking amiodarone. In Italy, in an area with suboptimal iodine supply, II-Hypo only occurred in 5% of such patients. The Italian study reported that 9.6% of their amiodarone-treated patients suffered from II-Hyper in contrast with only 5.3% in the United States (14,17). To the best of the authors' knowledge, in the accessible literature, no data regarding the influence of a change in iodine supply on the occurrence and severity of thyroid disorders caused by EII are available.
Existing data regarding the incidence and treatment of EII-induced thyroid disorders with respect to iodine supply are scarce. Therefore, this study aimed to establish eventual changes in the incidence, severity, and treatment of these disorders before and after the increase in iodine supply.
Patients and Methods
Patients
This retrospective clinical study was performed at the Outpatient Thyroid Department of the University Medical Centre Ljubljana (UMCL). This department is a tertiary referral center, which has a stable catchment area of one million inhabitants for decades. Therefore, the incidence of various thyroid disorders can be estimated from the number of new cases in a year. Each patient is clinically examined by internal medicine specialists, who have extensive knowledge and experience in diagnosing and treating thyroid disorders. A detailed patient history, including information regarding EII, is obtained. At the first examination, thyroid ultrasound and measurements of thyrotropin (TSH) and both free thyroid hormones are regularly performed. In most cases, thyroglobulin (Tg) and thyroid peroxidase (TPO) antibodies are also measured. If applicable, thyroid scintigraphy with technetium-99m (Tc-99m) pertechnetate is performed.
Slovenia has been considered to be an area with adequate iodine supply since 1999. Therefore, the years 1998–1999 were selected as the period before and the years 2000–2009 as the period after the increase in iodine supply. Medical records were reviewed of 47,563 patients who visited the Outpatient Thyroid Department of UMCL between 1998 and 2009 for the first time. Only patients with II-Hyper or II-Hypo were included in the study. Furthermore, from the computer database, patients who visited the center for the first time before 1998 but who were diagnosed with II-Hyper or II-Hypo between 1998 and 2009 were also included. Patients who were exposed to EII but who did not develop a thyroid disorder were not included.
In addition to age, sex, type of thyroid disorder, and laboratory data, information about the source of EII was collected. In the case of amiodarone, the duration of treatment with amiodarone was established. In patients with II-Hyper, data about the type and the duration of the therapy with antithyroid drugs were also collected.
Laboratory tests
Data were collected on serum concentrations of TSH, free thyroxine (fT4), free triiodothyronine (fT3), as well as Tg and TPO antibodies. The fT4/fT3 ratio was calculated. TSH was measured in both periods using third-generation TSH assays. In 1998 and 1999, the VITROS® test (Amerlite) was used. Between 2000 and 2009, TSH was measured using the ADVIA Centaur System (Siemens Medical Solutions Diagnostics). In 1998 and 1999, the reference values for TSH were 0.465–4.680 mIU/L, and between 2000 and 2009, they were 0.35–5.5 mIU/L. In 1998 and 1999, fT4 and fT3 were measured using the VITROS test (Amerlite), and between 2000 and 2009 they were measured using the ADVIA Centaur System (Siemens Medical Solutions Diagnostics). In 1998 and 1999, reference values for fT4 and fT3 were 10.0–28.2 pmol/L and 4.26–8.10 pmol/L, respectively. Between 2000 and 2009, reference values for fT4 and fT3 were 11.5–22.7 pmol/L and 3.5–6.5 pmol/L, respectively. In 1998 and 1999, levels of Tg and TPO antibodies (anti-Tg, anti-TPO) were measured using the Sorin Biomedica test, and between 2000 and 2009 they were measured using the ADVIA Centaur System (Siemens Medical Solutions Diagnostics). In 1998 and 1999, the reference value for anti-Tg was <100 kIU/L, and between 2000 and 2009 it was <60 kIU/L. In 1998 and 1999, the reference value for anti-TPO was <15 kIU/L, and between 2000 and 2009 it was <60 kIU/L.
Thyroid ultrasound
In each patient, thyroid ultrasound was performed using ALOKA machines with a 7.5 MHz transducer.
Thyroid scintigraphy
In most patients, thyroid scintigraphy was performed using a gamma camera equipped with a pinhole collimator (Siemens BASICAM) after intravenous administration of 100 MBq of Tc-99m pertechnetate.
Data on amiodarone
The National Institute of Public Health of the Republic of Slovenia provided the data regarding the number of prescribed boxes of amiodarone between 2002 and 2009. The number of prescribed boxes in 1998 and 1999 was accessible through previous unpublished data from the department. However, it was not possible to acquire data for the years 2000 and 2001.
Statistical methods
The Mann–Whitney U-test was used to compare measured values between the different groups. The data are presented as median values and range. Frequencies of different parameters were compared with the chi-square test. Spearman's test was used to establish possible correlations. Statistical analysis was performed with the Statistica software (StatSoft) program. p-Values <0.05 were considered to be statistically significant.
Results
Characteristics of patients
In the two-year period before the increase in iodine supply, 6745 patients were examined for the first time, while in the 10-year period after the increase in iodine supply, 40,818 patients were examined. Table 1 presents the number of all patients with EII-induced thyroid disorders and the number of patients with II-Hyper and II-Hypo in each year. Considering all patients examined for the first time, a significantly higher portion of patients with EII-induced thyroid disorders was found after the increase in iodine supply than before (1.93% and 1.47%, respectively; p = 0.011). Considering all patients with EII-induced thyroid disorders, the portion of patients with II-Hyper significantly decreased after the increase in iodine supply (94.94% and 80.03%, respectively; p < 0.001), while the portion of patients with II-Hypo significantly increased after the increase in iodine supply (5.1% and 19.97%, respectively; p < 0.001). As evident from Table 2, the age of the patients did not differ between the two observed periods (p = 0.862). A statistically significant shift in the ratio between the number of females and males in favor of males after the increase in iodine supply was identified (p = 0.038).
The percentage of patients with EII-induced thyroid disorders is also presented with respect to all patients examined for the first time, as well as the percentage of patients with II-Hyper and II-Hypo with respect to patients with EII-induced thyroid disorders.
EII, excessive iodine intake; TD, thyroid disorders; II-Hyper, iodine-induced hyperthyroidism; II-Hypo, iodine-induced hypothyroidism.
The number and percentage of female and male patients and the female/male ratio in the two periods are also presented.
p < 0.05 compared with the period 2000–2009.
Female/male ratio, ratio between the number of female and male patients.
The ratio between the number of patients with II-Hyper and II-Hypo was calculated in the two consecutive years for the period before and after the increase in iodine supply. In each two consecutive years in the period 2000–2009, this ratio was significantly lower than in the period 1998–1999 (Fig. 1). A significant decrease in the ratio occurred already in the first two years after the increase in iodine supply and later stabilized at the value of around 4:1.
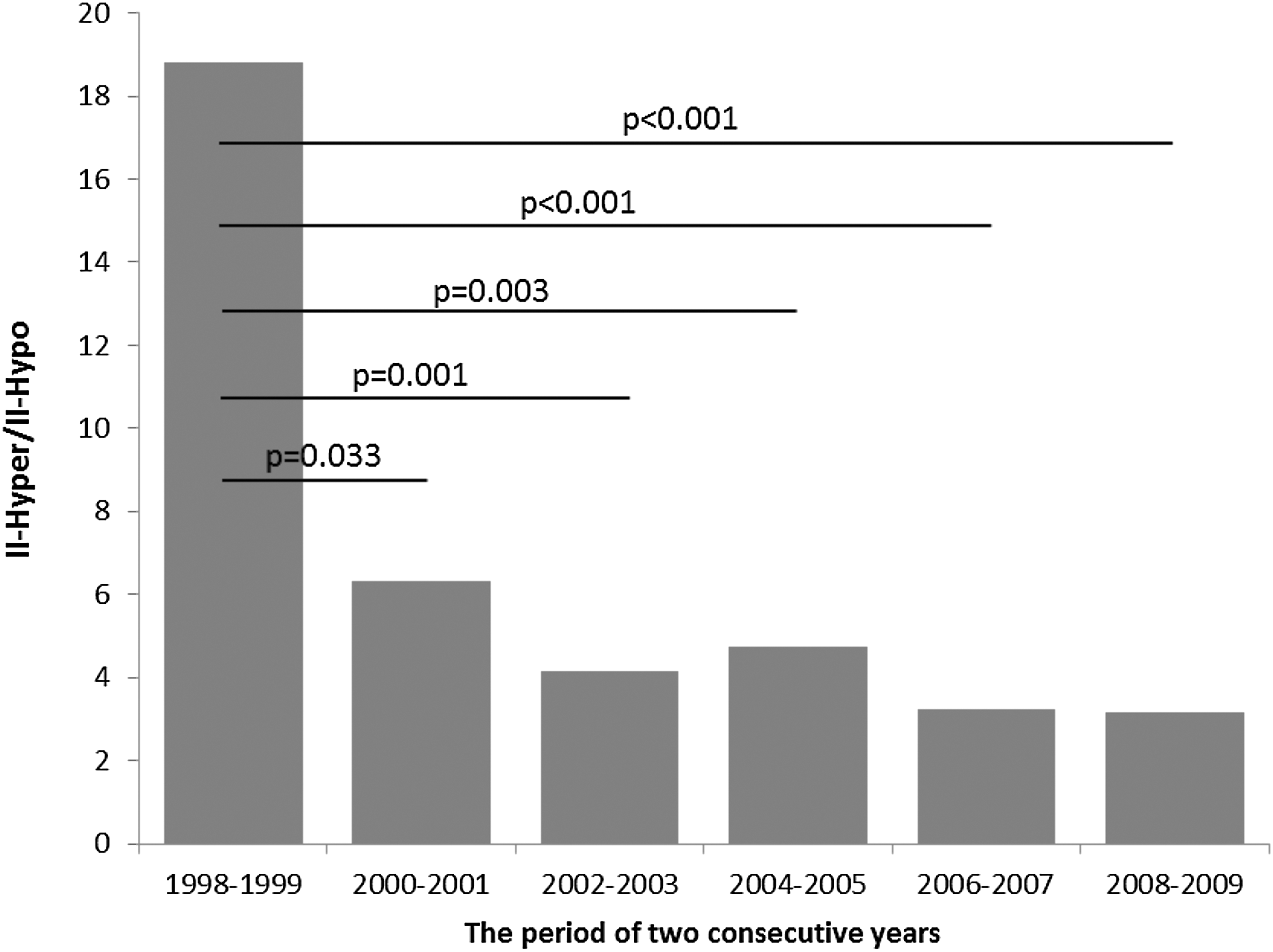
The ratio between the number of patients with iodine-induced hyperthyroidism and iodine-induced hypothyroidism preceding and following the increase in salt iodization. II-Hyper/II-Hypo, the ratio between the number of patients with iodine-induced hyperthyroidism and iodine-induced hypothyroidism. p-Values in the figure were obtained with the chi-square test. The period 1998–1999 was compared with the two consecutive years after the increase in iodine supply.
Clinical and laboratory findings in patients with II-Hyper
As evident from Table 3, the duration of treatment with amiodarone did not differ significantly between the two observed periods (p = 0.191). Although decreased, the concentration of TSH was significantly higher after the increase in iodine supply than before it (p = 0.002). The concentrations of fT4 and fT3 were significantly lower (p = 0.008 and p < 0.001, respectively), and the fT4/fT3 ratio was significantly higher (p < 0.001) after the increase in iodine supply than before it. After the increase in iodine supply, significantly higher values of anti-Tg and anti-TPO antibodies were identified (p < 0.001 and p < 0.001, respectively). Considering the concentration of free thyroid hormones, the patients with II-Hyper were classified into four groups. The first group consisted of patients with increased fT4 and fT3 level (overt hyperthyroidism). In the second and third groups, patients had increased levels of either fT4 or fT3. In the fourth group, the concentrations of fT4 and fT3 were normal (subclinical hyperthyroidism). As shown in Figure 2, after the increase in iodine supply, significantly fewer patients had overt hyperthyroidism and significantly more patients had subclinical hyperthyroidism (p = 0.007 and p = 0.015, respectively). Furthermore, after the increase in iodine supply, significantly fewer patients only had increased concentrations of fT3, and significantly more patients only had increased concentrations of fT4 (p < 0.001 and p = 0.011, respectively).
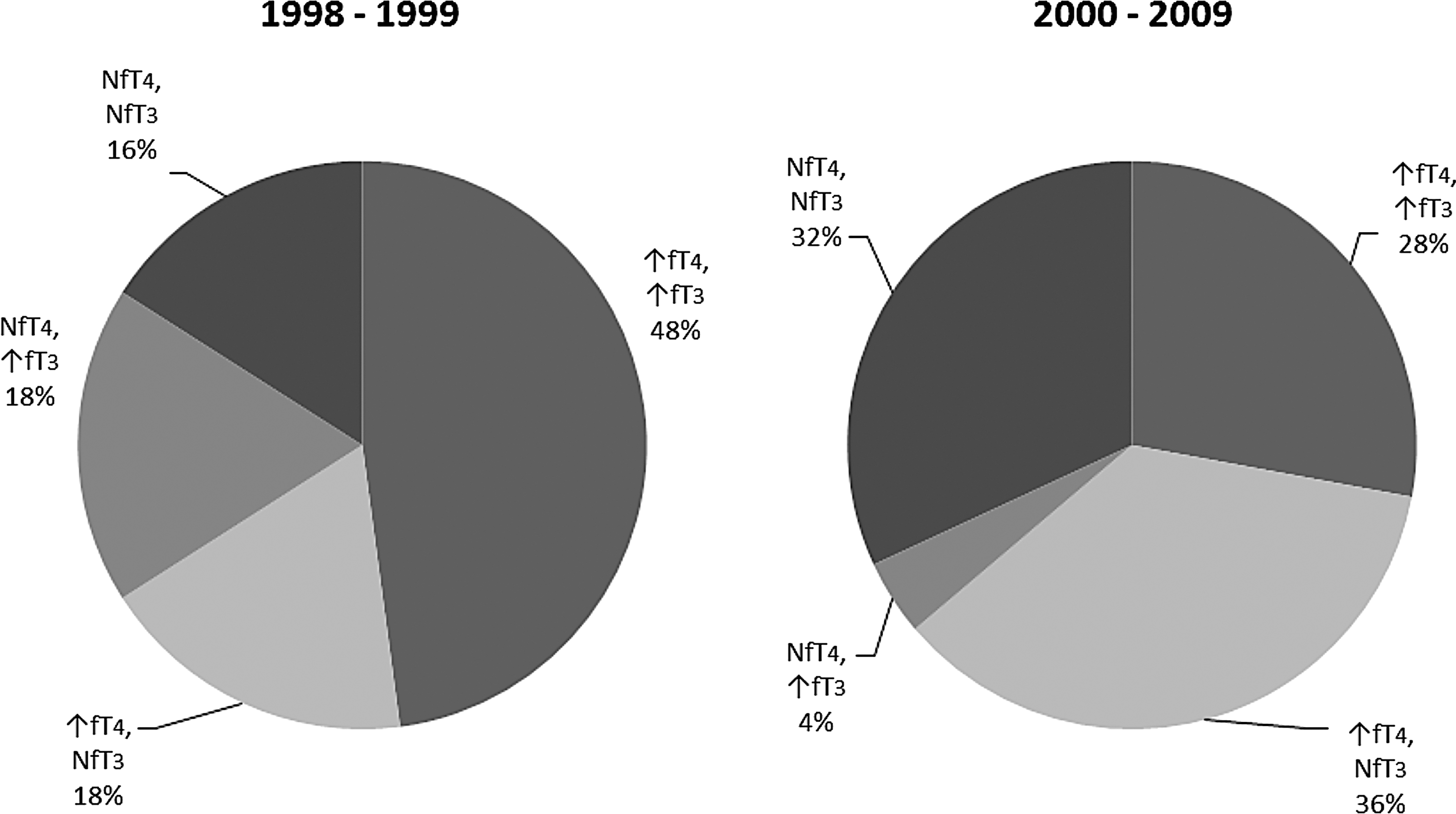
The pattern of distribution of free thyroid hormone concentration in patients with II-Hyper in the periods 1998–1999 and 2000–2009. II-Hyper, iodine-induced hyperthyroidism; ↑, increased concentration; N, normal concentration; fT4, free thyroxine; fT3, free triiodothyronine.
Data are presented as median (minimum–maximum value).
p < 0.05 compared with the period 2000–2009.
p < 0.001 compared with the period 2000–2009.
min, minimum; max, maximum; TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; anti-Tg, thyroglobulin antibodies; anti-TPO, thyroid peroxidase antibodies.
Treatment characteristics of patients with II-Hyper
The duration of treatment with antithyroid drugs was significantly shorter after the increase in iodine supply than before it (3.2 ± 2.5 and 8.1 ± 7.8 months, respectively; p = 0.001). Similarly, the duration of treatment with perchlorate was significantly shorter after the increase in iodine supply than before it (3.2 ± 2.6 and 6.0 ± 3.9 months, respectively; p = 0.002). Additionally, a significant negative correlation between the duration of treatment with antithyroid drugs and the level of anti-Tg after the increase in iodine supply was found (R = −0.151; p = 0.029).
Clinical and laboratory findings in patients with II-Hypo
As evident from Table 4, the duration of treatment with amiodarone in patients with II-Hypo did not differ between the two observed periods (p = 0.717). The concentrations of TSH and fT4 also did not differ significantly (p = 0.756 and p = 0.101, respectively). After the increase in iodine supply, the concentration of fT3 was significantly lower (p = 0.024), the fT4/fT3 ratio significantly higher (p = 0.007), and the concentrations of anti-Tg and anti-TPO significantly higher (p = 0.017 and p = 0.007, respectively) compared with the period before the increase in iodine supply.
The data are presented as median (minimum–maximum value).
p < 0.05 compared with the period 2000–2009.
p < 0.001 compared with the period 2000–2009.
Source of EII
As presented in Figure 3, the source of EII did not differ between the two periods for amiodarone, ICCM, iodine-containing vitamins, or unknown sources of EII (p = 0.468, p = 0.355, p = 0.262, and p = 0.260, respectively).
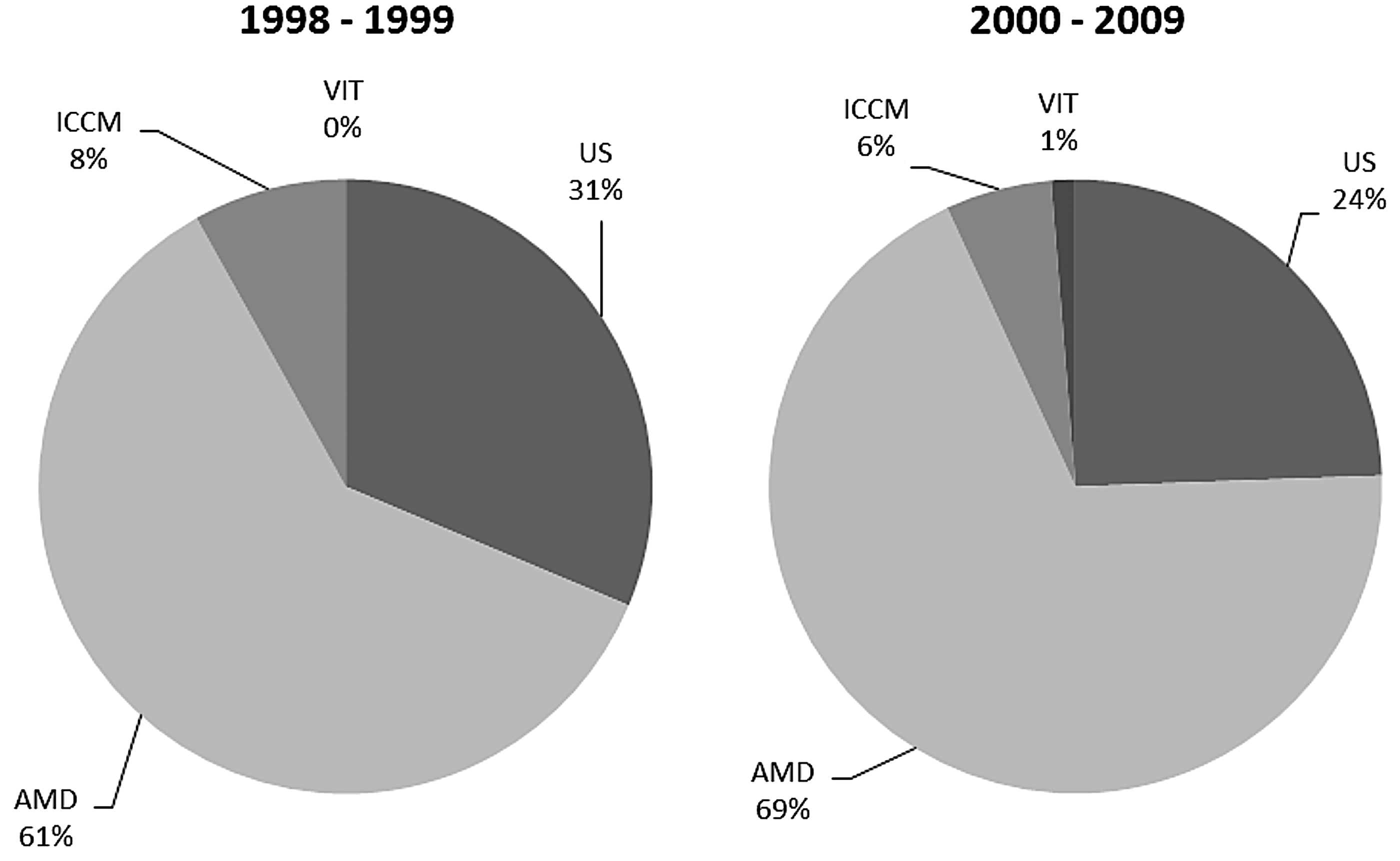
Distribution of patients based on the source of EII in the periods 1998–1999 and 2000–2009. EII, excessive iodine intake; ICCM, iodine-containing contrast medium; VIT, iodine-containing vitamin supplements; AMD, amiodarone; US, unknown source.
Amiodarone as a source of EII
Between 1998 and 1999, significantly fewer boxes of amiodarone were prescribed yearly than between 2002 and 2009 (19,560 ± 1191 and 30,522 ± 1215, respectively; p = 0.044). The ratio was calculated between the number of amiodarone-exposed patients, which was obtained from patient history data, and the number of prescribed boxes of amiodarone in order to get the standardized value for each year (Fig. 4). When comparing the period 1998–1999 with 2002–2004, a significant increase was found in the standardized number of all patients on amiodarone, and a significant increase was found in the standardized number of patients with II-Hypo (p = 0.034 and p = 0.001, respectively). However, the standardized number of patients with II-Hyper did not change significantly (p = 0.507). When comparing the period 1998–1999 with 2005–2009, a significant increase was found in the standardized number of patients with II-Hypo (p < 0.001). However, the number of all patients and the standardized number of patients with II-Hyper did not change significantly (p = 0.268 and p = 0.304, respectively). When comparing the period 2002–2004 with 2005–2009, a significant decrease was found in the standardized number of patients with II-Hyper (p = 0.019). However, the number of all patients and the standardized number of patients with II-Hypo did not change significantly (p = 0.099 and p = 0.566, respectively). Additionally, a significantly positive correlation between the year of the occurrence of EII-induced thyroid disease and the duration of treatment with amiodarone was found (R = 0.132, p = 0.048).
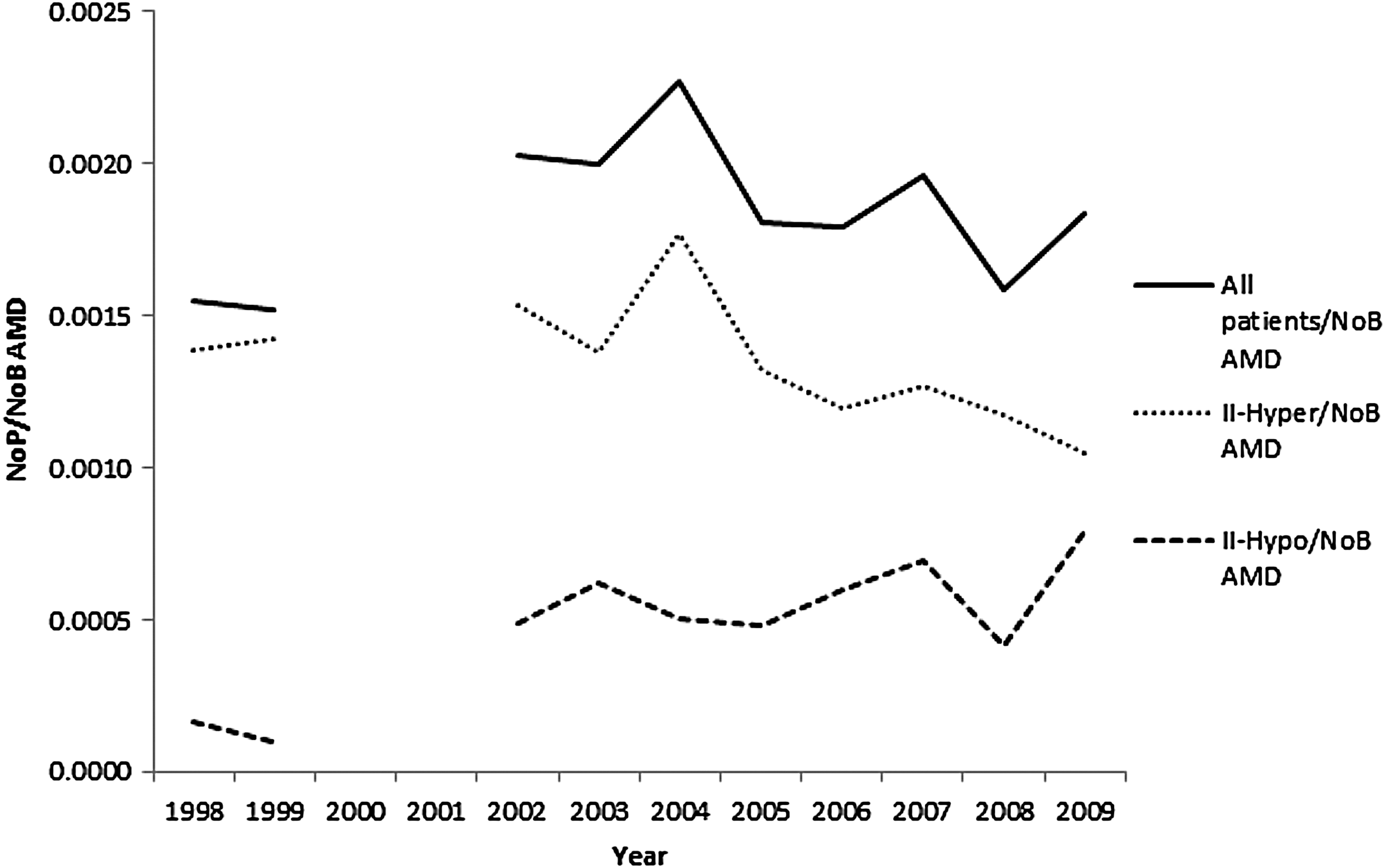
Ratio between the number of all patients who were using amiodarone and number of prescribed boxes of amiodarone; number of patients with II-Hyper who were using amiodarone and number of prescribed boxes of amiodarone; and number of patients with II-Hypo who were using amiodarone and number of prescribed boxes of amiodarone for each year. NoP, number of patients; NoB AMD, number of prescribed boxes of amiodarone; All patients, all patients with amiodarone-induced thyroid disorders; II-Hyper, number of patients with iodine-induced hyperthyroidism due to amiodarone; II-Hypo, number of patients with iodine-induced hypothyroidism due to amiodarone.
Discussion
This retrospective study for the first time evaluates the characteristics of EII-induced thyroid disorders before and after the increase in mandatory iodization of kitchen salt in an area that progressed from mild iodine deficiency to iodine sufficiency. After the increase in iodine supply, the incidence of II-Hypo increased, the incidence of II-Hyper decreased, II-Hyper became less severe, and the duration of treatment with antithyroid drugs and perchlorate was shorter than before. Moreover, the longer the patients had an adequate iodine supply, the longer they could take amiodarone before EII-induced thyroid disorders occurred.
In both observed periods, the ratio between females and males was in favor of females, which was unexpected, since males typically have EII-induced thyroid disorders 1.5 times more frequently than females (9). The decrease in this ratio after the increase in iodine supply can most likely be attributed to the more frequent prescription of amiodarone, especially to men (18,19).
A decrease in the incidence of II-Hyper was found after the increase in iodine supply. To the authors' knowledge, there are no similar studies comparing this incidence within the same population, but it is known that in areas with adequate iodine supply, the incidence of hyperthyroidism is lower than in areas with suboptimal iodine supply (17). In Denmark, the prevalence of low TSH was higher in moderate than in mild iodine deficiency (20). After the introduction of a mandatory iodization program, the prevalence of mild hyperthyroidism decreased (21). After the increase in iodine supply, in Austria, Germany, Switzerland, and Slovenia, a decrease in the incidence of thyroid autonomy was observed (22 –25). Underlying thyroid autonomy is a risk factor for II-Hyper (11,12). Most likely, in spite of the significant increase in the number of prescribed boxes of amiodarone leading to a higher incidence of II-Hyper, a simultaneous significant decrease in the incidence of thyroid autonomy resulted in a overall lower incidence of II-Hyper.
The shorter duration of treatment with antithyroid drugs and perchlorate in patients with II-Hyper after the increase in iodine supply can be attributed to the less severe II-Hyper. In the literature, no data about the severity and duration of treatment of II-Hyper with respect to iodine supply are available.
A significant increase in the incidence of II-Hypo, as well as in the level of anti-Tg and anti-TPO after the increase in iodine supply, was an expected result. In an area with suboptimal iodine supply (Italy) and in an area with adequate iodine supply (the United States), 5% and 22%, respectively, of patients treated with amiodarone developed II-Hypo (14,17). Hypothyroidism is most frequently caused by Hashimoto's thyroiditis (HT), which is diagnosed by increased levels of anti-Tg and/or anti-TPO antibodies. In long-standing iodine sufficiency, female sex, onset of puberty, and maternal autoimmunity were associated with thyroid antibody positivity in children (26). The reported prevalence of thyroid antibodies in areas with suboptimal iodine supply was around 13%, in adequate iodine supply around 18%, and in areas with excessive iodine supply around 25% (27 –29). In mild iodine deficiency, the increase in iodine supply increased the frequency of anti-Tg and/or anti-TPO antibodies up to four times (30). Also, in Slovenia, the incidence of HT increased after the increase in iodine supply (3), which, in the authors' opinion, significantly contributed to the increase in the incidence of II-Hypo. The data in the literature show that 20% of patients with HT develop hypothyroidism after the daily intake of 250 μg of iodine (31). Patients with HT have a mild defect in the organification of iodine. The excess of iodine intensifies this defect and leads to hypothyroidism (32).
The ratio between the number of II-Hyper and II-Hypo patients was higher in the period before the increase in iodine supply (18.8:1) than it was in the first two years after the increase (4:1), and it later continued to decrease. These results are in accordance with previous findings of a decreased incidence of thyroid autonomy and increased incidence of HT (3,25).
After achieving adequate iodine supply, patients with II-Hyper were less severely hyperthyroid. The higher fT4/fT3 ratio in these patients was predominantly explained by the lower fT3 concentration. The weakness of this part of the study is that different laboratory tests were used for the determination of TSH, fT4, and fT3 in both periods. Therefore, the absolute values of thyroid hormones in these periods cannot be reliably compared. For this reason, the fT4/fT3 ratio was calculated, which is only affected by the synthesis of thyroid hormones and the conversion of fT4 into fT3 by 5′ deiodinases (33). Studies in rats show that the thyroid gland compensates for suboptimal iodine intake by releasing more T3 than T4 because of higher expression of intrathyroidal deiodinases (34). Nonetheless, under conditions of adequate iodine supply, the situation is reversed (34). Therefore, it is presumed that after the increase in iodine supply, less fT3 is released from the thyroid, which is also supported by the results. Since in hyperthyroidism the thyroid gland is a major source of T3 (33), less severe II-Hyper after the increase in iodine supply most likely contributed to a higher fT4/fT3 ratio. In peripheral tissues, however, the activity of deiodinase type I (D1) and type II (D2) prevails in hyperthyroidism and hypothyroidism, respectively, while in euthyroid state, D2 is a major source of T3 (33). Most likely, less severe II-Hyper after the increase in iodine supply was associated with less active D1 and with a lower synthesis of fT3. Amiodarone decreases the activity of 5′ deiodinases (35), which also could have contributed to a higher fT4/fT3 ratio. Less severe II-Hyper is an expected result of this study if we consider underlying thyroid autonomy as the main cause of type 1 II-Hyper (11,12,25).
As expected, amiodarone was the most frequent source of EII. After the increase in iodine supply, the standardized number of patients with II-Hypo who were using amiodarone most likely increased because of the increased incidence of HT. A significantly lower standardized number of patients with II-Hyper in the period 2005–2009 than in 2002–2004 might be related to a decreased incidence of thyroid autonomy.
An additional aspect of a beneficial effect of adequate iodine supply on EII-induced thyroid disorders represents the finding that the longer the patients lived in the area with adequate iodine supply, the longer they could use amiodarone before an EII-induced thyroid disorder developed. Therefore, the thyroid-related side effects of amiodarone decrease as a function of the time spent in an environment of adequate iodine supply, which is a new finding. This study is in line with the recent publication by Völzke et al. (36), which emphasized the importance of monitoring outcome in already established iodination programs.
Conclusion
After achieving an adequate iodine supply by increasing mandatory iodization of kitchen salt, a lower incidence of II-Hyper can be attributed to a lower incidence of thyroid autonomy. The observed increase in the incidence of II-Hypo could be related to a higher incidence of HT. Other beneficial clinical consequences are less severe II-Hyper and a shorter duration of treatment of II-Hyper, as well as longer thyroid disease-free period in patients taking amiodarone.
Footnotes
Acknowledgments
The abstract was presented at the Annual Meeting of the European Association of Nuclear Medicine in Gothenburg, Sweden, in 2014 and at the Annual Meeting of the European Thyroid Association in Santiago de Compostela, Spain, in 2014.
Author Disclosure Statement
No competing financial interests exist.