
Abstract
Introduction:
The presence of the Thr92Ala polymorphism of deiodinase-2 (D2) has been thought to have several effects. It may influence its enzymatic function, is associated with increased expression of genes involved in oxidative stress in brain tissue, and may predict favorable response to combination levothyroxine (LT4) plus triiodothyronine (T3) therapy. It was hypothesized that homozygous carriers of the D2-92Ala allele have different thyroid hormone parameters, and reduced health-related quality of life (HRQoL) and cognitive functioning.
Methods:
In 12,625 participants from the LifeLines cohort study with genome-wide genetic data available, the effects of the Thr92Ala polymorphism (rs225014) were evaluated in the general population and in 364 people treated with thyroid hormone replacement therapy, the latter mainly because of primary hypothyroidism. In addition to evaluating anthropometric data, medication use, and existence of metabolic syndrome, HRQoL was assessed with the RAND 36-Item Health Survey, and the Ruff Figural Fluency Test was used as a sensitive test for executive functioning. Data on thyrotropin, free thyroxine (fT4), and free T3 (fT3) levels were available in a subset of 4479 participants.
Results:
The mean age (±standard deviation) was 53 ± 12 years and the body mass index was 27.0 ± 4.5 kg/m2 in the LT4 users compared with 48 ± 11 years and 26.2 ± 4.1 kg/m2 in participants from the general population. The Ala/Ala genotype of the D2-Thr92Ala polymorphism was present in 11.3% of LT4 users and in 10.7% of the general population. In total, 3742/4479 subjects with thyroid hormone data available had normal TSH (0.4–4.0 mIU/L), and 88% of LT4 users were females. LT4 users had higher fT4, lower fT3, and a lower fT3/fT4 ratio, and female patients had lower scores on the HRQoL domains of physical functioning, vitality, mental health, social functioning, bodily pain, and general health compared with those not using LT4 (p < 0.005). Executive functioning scores, as part of cognitive functioning, were comparable between female LT4 users and the general population. In both groups, the D2-Thr92Ala polymorphism was not associated with differences in TSH, fT4, fT3, the fT3/fT4 ratio, presence of metabolic syndrome or other comorbidities, use of medication, HRQoL, and cognitive functioning.
Conclusion:
The Thr92Ala polymorphism of D2 was not associated with thyroid parameters, HRQoL, and cognitive functioning in the general population and in participants on thyroid hormone replacement therapy.
Introduction
P
In addition to health-related quality of life (HRQoL), impairments of thyroid function may interfere with cognitive functioning. Earlier studies have indicated that decreased thyroid function is especially associated with decreased information processing speed, poor learning, and reduced efficiency in executive functions (10). Whether these functions improve with thyroid hormone replacement therapy is still unclear (11).
The thyroid gland produces both T3 and T4. Only 20% of T3 is directly secreted from the thyroid gland, and 80% of T3 is formed by deiodination of T4 in extrathyroidal tissue. This reaction is catalyzed by two types of deiodinase enzymes: deiodinase-1 (D1) and deiodinase-2 (D2) (12). D1 is the predominant deiodinating enzyme in the liver and kidney, whereas D2 is predominant in the thyroid gland, brain, pituitary gland, skeletal muscle, heart, and skin. Deiodinase-3 (D3) is the main inactivating enzyme, which can inactivate both T4 (by conversion to reverse T3) and T3 (by conversion to T2) (13). Together, these three enzymes regulate the normal euthyroid state in the blood and tissues.
During recent years, it has been demonstrated that certain genetic polymorphisms of deiodinases may be associated with variation in thyroid hormone levels (14 –17). Even a modest variation in thyroid hormone levels can be associated with substantial phenotypic effects (18). The common single nucleotide polymorphism (SNP) rs225014 in the DIO2 gene results in a single amino acid substitution at position 92 (19), in which threonine (Thr) is replaced by alanine (Ala). The functional effect of this replacement has not yet been fully elucidated. Torlontano et al. (20) showed that athyreotic differentiated thyroid cancer patients who are homozygous carriers of the D2-92Ala allele needed higher doses of LT4 to achieve target TSH levels. Several other studies failed to detect an association between the polymorphism and thyroid function tests (14 –16,21,22), although recently it was suggested that the presence of this polymorphism could be associated with a higher than normal fT4/fT3 ratio (23). Panicker et al. (24) reported that patients with the Ala/Ala genotype of the D2-Thr92Ala polymorphism had a significantly lower psychological well-being and greater improvement of general health when treated with combined LT4/liothyronine therapy compared with LT4 alone. A recent study renewed interest in the genetic variation of D2, as it showed that homozygous carriers of the D2-92Ala allele exhibited increased expression of genes associated with oxidative stress and inflammation in brain tissue (25), and concluded that this could contribute to neurocognitive symptoms of affected carriers. Other studies have suggested an association between the D2-Thr92Ala polymorphism and insulin resistance, bipolar disorder, mental retardation, hypertension, and osteoarthritis (22).
It was hypothesized that homozygous carriers of the D2-92Ala allele can be recognized by having a low fT3/fT4 ratio, more frequently have high blood pressure and metabolic syndrome, experience lower HRQoL, and have impaired cognitive functioning in comparison with subjects who are heterozygous Thr/Ala or homozygous Thr/Thr carriers. This hypothesis was tested in healthy individuals from the general population and in patients using thyroid replacement therapy, who participated in a large population-based study.
Materials and Methods
Subjects
This cross-sectional study used data from subjects participating in the LifeLines cohort study. LifeLines is a multidisciplinary prospective population-based cohort study examining in a unique three-generation design the health and health-related behaviors of persons living in the north of Netherlands. It employs a broad range of investigative procedures in assessing the biomedical, sociodemographic, behavioral, physical, and psychological factors that contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics (26). The methodology has been described previously (27). All participants were between 18 and 90 years old at the time of enrollment. They provided written informed consent before participating in the study. The study protocol was approved by the medical ethical review committee of the University Medical Center Groningen.
The present study intended to include the 13,194 subjects in whom whole-genome SNP data were available. Subjects who were not of Western European descent and those who were current users of drugs known to influence thyroid hormone parameters such as liothyronine, lithium, amiodarone, methimazole, propylthiouracil, and corticosteroids were excluded. Participants with a CRP level >10 mg/L were also excluded because inflammation may disturb the activity of the deiodinase enzymes (28). Therefore, data for 12,625 participants could be analyzed, and of these, thyroid function parameters were available for 4479 participant. A total of 364 (3%) participants were using thyroid hormone replacement therapy with LT4. The majority of them used LT4 for primary hypothyroidism, and others after treatment for thyrotoxicosis or after thyroid surgery. The level of detail of the LifeLines data set does not allow further refinement of causes for LT4 use.
Clinical examination
Subjects completed a self-administered questionnaire on medical history, past and current diseases, use of medication, and health behavior at home. Medication was verified by a certified research assistant. Body weight was measured without shoes to the nearest 0.1 kg. Height and waist and hip circumference were measured to the nearest 0.5 cm. Waist circumference was measured in a standing position with a tape measure all around the body, at the level midway between the lower rib margin and the iliac crest. Body mass index (BMI) was calculated by dividing weight in kilograms by the squared height in meters (kg/m2). Systolic and diastolic blood pressure were measured every minute for a period of 10 minutes using a DINAMAP Monitor. The size of the cuff was chosen according to the arm circumference. The average of the last three measurements was reported for each of the blood pressure levels.
HRQoL
HRQoL was measured using the RAND 36-Item Health Survey (27). The RAND-36 includes exactly the same items as the 36-Item Short Form Health Survey v1.0. However, the scoring for the two domains of bodily pain and general health are slightly different. This generic questionnaire consists of 36 items in eight subscales: physical functioning (10 items), role limitations due to physical health problems (four items), bodily pain (two items), general health (five items), vitality (four items), social functioning (two items), role limitations due to emotional problems (three items), and general mental health (five items) (29). Scores on the eight domains are generated as described elsewhere (27,29,30). A higher score reflects a better health status and well-being. Since there is a difference in HRQoL scores between men and women, data were analyzed separately for each sex. As HRQoL scores are not normally distributed, for each domain a sex-specific cutoff point was used at the 75th percentile of the healthy non-obese general population, as described by Slagter et al. (30). Participants with a score lower than this cutoff were considered to have an abnormally low score for this specific domain.
Cognitive functioning
Executive functioning, as part of cognitive functioning, was assessed in LifeLines with the Ruff Figural Fluency Test (RFFT) (31). Participants received five sheets of paper with 35 squares with five-dot patterns (Supplementary Fig. S1; Supplementary Data are available online at
Genomics
The genotype data for the Thr92Ala (rs225014) SNP were derived from genome-wide genotyping performed with the Illumina HumanCytoSNP12 v2 beadchip assay (Illumina, Inc., San Diego, CA) as described previously (32). Frequency of the allele distribution of the D2-Thr92Ala polymorphism (common D2-Thr92 or T-allele, minor D2-Ala92 or C-allele) was calculated with PLINK (33).
Biochemical measurements
Blood samples were collected in the morning after an overnight fast, directly into tubes containing heparin, and centrifuged. Measurements were performed in the clinical chemistry laboratory of the University Medical Center Groningen. Serum levels of total and high-density lipoprotein cholesterol were measured using an enzymatic colorimetric method, triglycerides using a colorimetric UV method, and low-density lipoprotein cholesterol using an enzymatic method, all on a Roche Modular P chemistry analyzer (Roche, Basel, Switzerland). HbA1c was measured using a turbidimetric inhibition immunoassay on a Cobas Integra 800 CTS analyzer (Roche Diagnostics Nederland BV, Almere, Netherlands). Fasting blood glucose was measured using a hexokinase method, and hs-CRP was analyzed using nephelometry (BN II system; Siemens, Marburg, Germany). Results of the thyroid hormone status were available in a subset of 4479 participants. TSH, fT4, and fT3 were assayed by electrochemiluminescent immunoassay on the Roche Modular E170 Analyzer using kits provided by the manufacturer (Roche, Basel, Switzerland) (27). Normal values are 11–20 pmol/L for fT4 and 4.4–6.7 pmol/L for fT3. The general Dutch population is iodine sufficient. Tests to measure antithyroid peroxidase antibody levels were not performed.
Data description and statistical analysis
The number of different medications used by a participant was considered as a proxy for multi-morbidity (34). The presence of the metabolic syndrome was calculated according to the revised criteria of the National Cholesterol Education Program's Adult Treatment Panel III (NCEP ATP III) (35).
The initial analyses showed that there were differences in sex distribution, age, and BMI between participants using LT4 and the general population, and 88% of the LT4 users were female. This would have influenced the interpretation of the thyroid hormone parameters, as well as the scores of HRQoL and executive functioning. Therefore, the data were reevaluated in the female participants only after matching the LT4 users 1:5 with control participants for age and BMI. Matching was adequate, with mean age being 52.7 ± 11.4 versus 52.1 ± 11.1 years, and BMI 27.0 ± 4.6 versus 26.9 ± 4.4 kg/m2 in LT4 users versus the matched control group, respectively.
SNPs were coded by genotype as 0, 1, and 2, with individuals homozygous for the non-risk allele as the reference group. To examine the main effect of the D2-Thr92Ala SNP, the three genotypes (Thr/Thr, Thr/Ala, and Ala/Ala) were considered separately under the additive model.
All analyses were conducted using IBM SPSS Statistics for Windows v22 (IBM, Armonk, NY). Data are presented as mean ± standard deviation (SD), or median and interquartile range when not normally distributed. Means were compared between groups with analysis of variance. When variables were not normally distributed, medians were compared with the nonparametric Kruskal–Wallis test. The chi-square test was used to analyze categorical variables. To adjust for multiple comparisons, a p-value of <0.01 was considered statistically significant.
Results
Relevant baseline characteristics are shown in Table 1 for participants using LT4 and those from the general population. LT4 users more often were women, and they were older than participants from the general population. Both groups had similar TSH levels. There were, however, significant differences of fT3 and fT4 between those with and without LT4 therapy. fT3 was lower and fT4 was higher in the individuals using LT4. Patients treated with LT4 reported significantly more comorbidities such as atherosclerosis, gallstones, Parkinson's disease, anemia, osteoporosis, and depression compared with the general population. Also, the LT4 group used a higher number of other medications (median 1.9 vs. 1.1 other drugs). In particular, lipid-lowering medication was used more often (Table 1).
Data are given as mean ± SD, or median (IQR) when not normally distributed.
Available in 4336 participants from the general population, and 143 LT4 users.
LT4, levothyroxine; M, males; F, females; BMI, body mass index; TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; BP, blood pressure; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation; IQR, interquartile range.
The Ala/Ala genotype of the D2-Thr92Ala polymorphism was present in 11.3% of the LT4 users and 10.7% in the general population, whereas the Thr/Thr genotype frequency was 44.8% and 44.2%, respectively. Only 52% of LT4 users had a TSH level within the normal range (0.4–4.0 mIU/L), while 17% had a TSH level <0.4 mIU/L, and 31% had a TSH level >4.0 mIU/L. In the general population, 88% had normal TSH values. There were no significant associations between the number of D2-Ala92 alleles and the TSH classes in the LT4 users (data not shown) as well as in the general population (Supplementary Table S1).
Table 2 depicts the characteristics and thyroid hormone parameters between the different genotype groups of the D2-Thr92Ala SNP for the total study population of 12,625 participants. No statistically significant differences were observed in these parameters. Also, lipid levels and percentage of participants fulfilling the criteria for the metabolic syndrome were not different in individuals carrying the Ala/Ala genotype compared to the other two genotype groups, and neither was the percentage of participants using blood pressure or cholesterol-lowering drugs. Thyroid hormone parameters were also similar when these parameters were evaluated in the different genotype groups separately for female LT4 users and their matched control group (Table 3). A lower fT3/fT4 ratio in the Ala/Ala carriers was not observed in participants from the general population, LT4 users, or matched non-LT4 users.
Data are given as mean ± SD, median (IQR) when not normally distributed, or percentage.
Available for 4336 participants from the general population, and 143 LT4 users.
Available in 628 participants.
Available in 131 participants.
Data are given as mean ± SD, or median (IQR).
HRQoL and cognitive functioning
As the number of males using LT4 was limited (43/364), their HRQoL was not evaluated in comparison to males from the general population, and only data from the female population are reported. Compared with matched controls, a significantly larger proportion of female LT4 users had a score lower than the cutoff value, indicating a poor score, in six of the eight subscales (i.e., physical functioning, vitality, mental health, social functioning, bodily pain, and general health; Table 4). There was no difference in cognitive functioning between females using LT4 and the matched control group in both the creation of unique designs (p = 0.420), their z-scores (p = 0.949), and perseverative errors (p = 0.701; Table 5).
Data are given as percentage for the different HR-QoL domains, and as mean ± SD and median (IQR) for RFFT scores. For each HR-QoL domain a sex-specific cutoff point at the 75th percentile of the healthy non-obese general population was used, as described by Slagter et al. (30).
HR-QoL, health-related quality of life; RFFT, Ruff Figural Fluency Test; NS, not significant.
Data are given as mean ± SD, or median (IQR).
An association could not be demonstrated between the number of Ala alleles and HRQoL in the general population (Fig. 1), in LT4 users, and in their matched controls (Supplementary Table S2). Also, an association was not observed between the number of the D2-Ala92 alleles and cognitive functioning (unique patterns of z-score) in the LT4 users (p = 0.912), the matched control group (p = 0.083), and the general population (p = 0.372; Table 5).
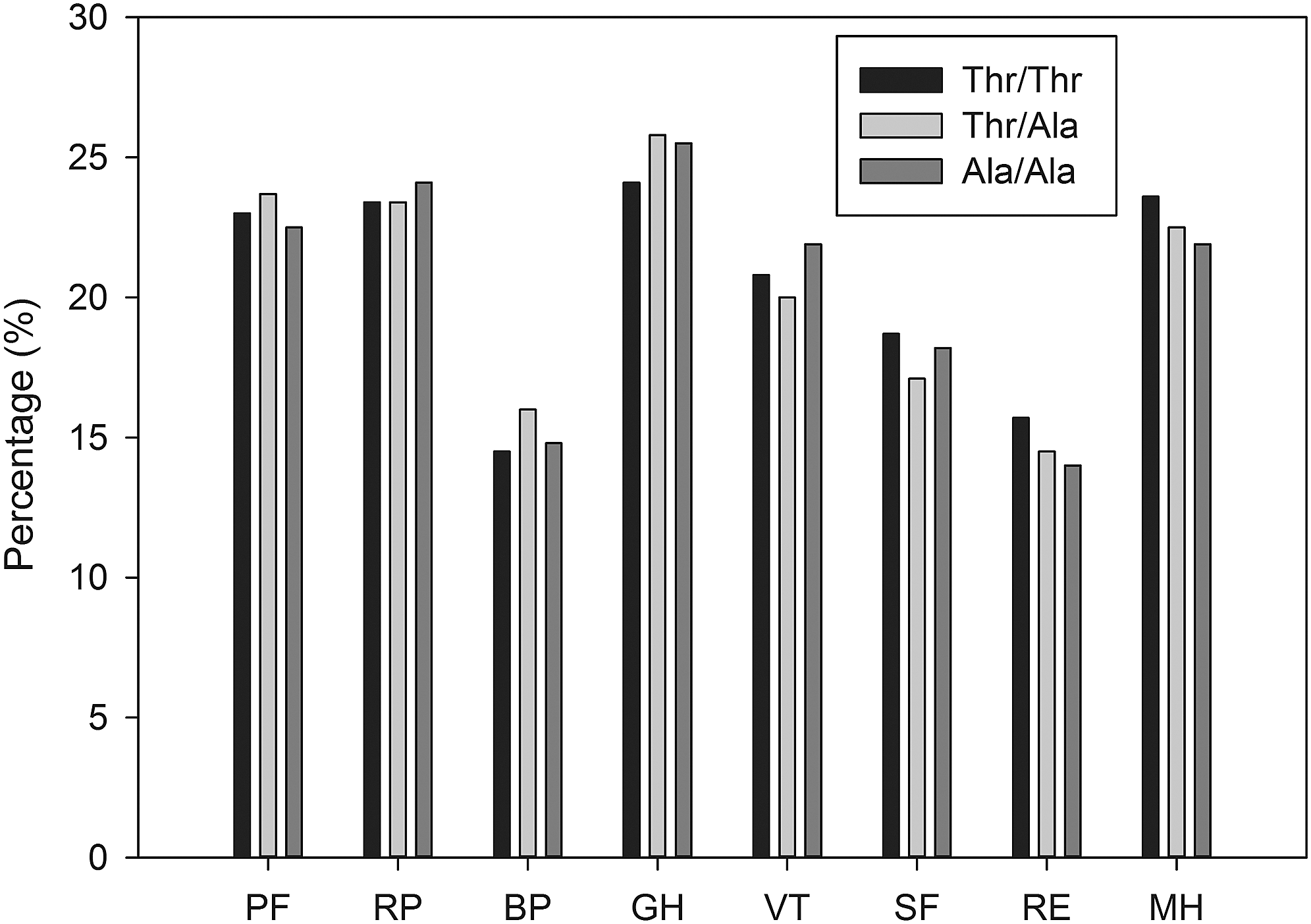
Percentages of female participants in the general population with a poor health-related quality of life domain score, according to Thr or Ala carriership. The corresponding cutoff value derived from the scores in the normal weight population for the individual domains (25th percentile): PF, physical functioning (85.0); RP, role limitations due to physical health problems (100.0); BP, bodily pain (67.4); GH, general health (65.0); VT, vitality (55.0); SF, social functioning (75.0); RE, role limitations due to emotional problems (100.0); MH, mental health (72.0). There are no statistically significant differences between Thr/Thr, Thr/Ala, and Ala/Ala.
Discussion
In this large cross-sectional study, participants using LT4 had a lower fT3 and a higher fT4, while their TSH was comparable to the general population. Also, female LT4 users had lower HRQoL in six of the eight domains of the RAND-36 questionnaire (physical functioning, vitality, mental health, social functioning, bodily pain, and general health), but a difference in cognitive functioning was not observed. In contrast to the hypothesis, the D2-Thr92Ala polymorphism was not associated with any of the thyroid parameters, percentage of participants with the metabolic syndrome, percentage of participants using blood pressure or cholesterol-lowering drugs, HRQoL, and cognitive functioning either in the general population or subjects on thyroid hormone replacement therapy or in matched controls.
Renewed interest in the effects of polymorphisms of deiodinases came after the elegant recent study by McAninch et al., who showed that the D2-Ala92 polymorphism was associated with increased expression of genes associated with oxidative stress and inflammation in brain tissue (36). These are relevant findings for the clinician, considering that 10–12% of patients treated for primary hypothyroidism experience complaints such as fatigue, lack of energy, reduced exercise capacity, and disturbances in concentration and mental functioning, despite optimal thyroid hormone replacement therapy. It has been suggested that some of these patients can be identified by a lower fT3/fT4 ratio (23), and may favorably respond to combination therapy of LT4 and liothyronine (24). Thus, it may be warranted to identify those patients in clinical care, preferentially based on simple parameters such as thyroid hormone measurements, who may show the best response to this treatment. In this study, there was no association between the plasma level of fT4, fT3, and the fT3/fT4 ratio and the number of D2-Ala92 alleles. There are two studies that indirectly showed that the T4 to T3 conversion could be diminished in subjects carrying the D2-Thr92Ala polymorphism. Butler et al. showed that the Thr92Ala polymorphism is associated with a delayed T3 secretion in response to TRH stimulation (37). Torlantano et al. showed that thyroidectomized patients carrying the Thr92Ala polymorphism needed higher doses of LT4 to achieve target TSH levels (20). Other studies failed to confirm these findings (38,39).
The current study evaluated HRQoL with the RAND-36 questionnaire, a generic questionnaire on well-being, of which physical functioning, vitality, and general health are prominent domains. The RAND-36 instrument proved able to discriminate differences in HRQol, as it was found that more LT4 users reported impaired HRQoL compared with the matched euthyroid participants. Women using LT4 experienced a significant reduction in HRQoL in several RAND-36 domains. However, no differences in any of the RAND-36 domain scores were observed between the Thr/Thr and the Ala/Ala carriers in all three groups evaluated (the general population, the LT4 users, and their matched controls), which confirms an earlier report by Appelhof et al. (40). It has been known from several studies that comorbidities may strongly influence HRQoL. In the present population, participants treated with LT4 used more other medications (median 1.9 vs. 1.1) than those not using LT4. The number of medications used is considered as a proxy for the presence of other comorbid disorders (34). In particular, lipid-lowering drugs were more often used by LT4 users. Also, more LT4 users reported complaints related to gallbladder disease, anemia, atherosclerosis, and depression.
In addition to the more traditional HRQoL assessment, it was possible to assess potential differences in concentration and mental functioning in the present population with the RFFT. This test measures the ability to draw as many unique designs as possible within a set time period, and is a sensitive cognitive test for changes in nonverbal fluency in young as well as old persons (31,41 –43). The test provides insight in many different cognitive abilities that range from initiation and planning to divergent reasoning and mental flexibility. These characteristics and the limited time that is allowed to administer the test make the RFFT a useful outcome measure for cognitive functioning and early cognitive decline (42,43). No differences were observed in RFFT scores between participants who used LT4 and those who did not. This is in accordance with the study by Samuels et al., in which executive functioning was assessed with the Letter Cancellation Test, Train Making Test, and the Iowa Gambling Test (44). Another study by Samuels et al. did show a significantly lower cognitive functioning and HRQoL in patients treated with LT4 compared to healthy controls, which it was suggested was related to suboptimal treatment (45).
The findings by McAninch et al. (36) suggest that the D2-Thr92Ala polymorphism could be a risk factor for neurodegenerative diseases and neuropsychological impairment. In the current study, carriers of the two D2-Ala92 alleles did not show a worse score compared to the other two groups. To the authors' knowledge, no other studies have been performed that investigated the association between the D2-Thr92Ala polymorphism and executive functioning. Replication of the present findings in other cohorts and perhaps with other techniques assessing cognitive functioning may be warranted. The single amino acid substitution of Thr for Ala lies within the 18 amino acid loop that controls susceptibility to T4-induced ubiquination of D2 (46). This mutated enzyme is ectopically located in the Golgi apparatus and has a longer half-life. Also the Golgi apparatus has a different structure. The cellular abnormalities result in alterations at the transcriptional level and are independent of D2-mediated T3 production. These transcriptional changes are associated with mitochondrial dysfunction, inflammation, apoptosis, changes in DNA repair, and growth factor signaling (36). This may explain why it has been suggested that the D2-Thr92Ala polymorphism may result in such diverse phenotypic outcomes, such as insulin resistance, bipolar disorder, mental retardation, hypertension, and osteoarthritis (22). However, the current study did not find any association between the D2-Ala92 polymorphism and metabolic syndrome or hypertension, or their treatment.
There are some strengths and limitations to this study. More than 12,600 individuals from the general population were evaluated, which is one of the largest cohorts to date of people in whom both information on the D2-Thr92Ala polymorphism, thyroid hormone parameters, and HRQoL was available. A limitation of this study is that the analyses were mainly limited to female users of LT4, as <12% of subjects using thyroid replacement therapy were male. Considering the 3% prevalence of primary hypothyroidism in the general population, only a small number of LT4 users could be included in this cross-sectional study. Nevertheless, this study was specifically chosen to be performed in the general population, as evaluating LT4 users treated in other settings, for instance an endocrinology outpatient clinic, may overestimate the prevalence of residual complaints and reduced HRQoL. Typically, patients with more severe complaints are more likely to be referred to an endocrinologist.
In conclusion, this study demonstrates that women using thyroid hormone replacement therapy experience a lower HRQoL in six domains of the RAND-36 questionnaire (physical functioning, vitality, mental health, social functioning, bodily pain, and general health) compared with matched participants from the general population. The Thr92Ala polymorphism of D2 was not associated with thyroid parameters, elevated blood pressure, metabolic syndrome, HRQoL, or executive functioning in the general population and in subjects using thyroid replacement therapy.
Footnotes
Acknowledgments
The authors wish to acknowledge all participants of the LifeLines cohort study and everybody involved in the set-up and implementation of the study.
LifeLines has been funded by a number of public sources, notably the Dutch Government, The Netherlands Organization of Scientific Research NOW (grant 175.010.2007.006), the Northern Netherlands Collaboration of Provinces (SNN), the European fund for regional development, Dutch Ministry of Economic Affairs, Pieken in de Delta, Provinces of Groningen and Drenthe, the Target project, BBMRI-NL, the University of Groningen, and the University Medical Center Groningen, Netherlands. This work was supported by the National Consortium for Healthy Ageing, and funds from the European Union's Seventh Framework program (FP7/2007-2013) through the BioSHaRE-EU (Biobank Standardisation and Harmonisation for Research Excellence in the European Union) project, grant agreement 261433. LifeLines (BRIF4568) is engaged in a Bioresource research impact factor (BRIF) policy pilot study, details of which can be found at
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.