
Abstract

T
It is within the context of this changing landscape that the authors of this commentary participated in the Endocrine Pathology Society's conference to re-evaluate encapsulated non-invasive follicular variant papillary thyroid carcinoma in Boston, Massachusetts, in March 2015. These tumors represent the subset of follicular variant PTC (FVPTC) that are encapsulated or clearly demarcated without evidence of capsular or vascular invasion. Through a number of pre-meeting conference calls and then a two-day long in-person meeting, these tumors were reconsidered by a panel of internationally recognized expert pathologists and clinicians, including endocrinologists, a surgeon, patient representatives, and an expert in the field of the psychiatric burden of cancer. The conclusion of this group was to rename these tumors as NIFTP—non-invasive follicular thyroid neoplasm with papillary-like nuclear features (8). So, why the name change?
FVPTC is a common diagnosis that has risen in incidence by fourfold in the last three decades, currently comprising >20% of all thyroid cancers in Europe and North America (9,10). FVPTC is subdivided into two subtypes: infiltrative (non-encapsulated) and encapsulated. The latter may present with no invasion or show focal invasion of the tumor capsule or blood vessels while still preserving overall tumor encapsulation. Several key retrospective studies have demonstrated that the non-invasive encapsulated form of FVPTC is a highly indolent tumor demonstrating a risk of overall recurrence (local, regional, and distant) of <1% in >300 published cases with extended follow-up, despite the fact that for the majority, treatment consisted of lobectomy only without RAI ablation (11 –17). The work leading up to this conference demonstrated in a new carefully annotated group of >200 additional cases collected from several countries around the world that (i) stringent criteria could successfully be applied allowing a reproducible histologic diagnosis of NIFTP (Fig. 1), and (ii) despite prevalent management with lobectomy without RAI, no evidence of recurrence at any site or disease-related death occurred in patients followed for 10–26 years. Genetic analysis of these lesions also demonstrated that NIFTP is predominantly driven by RAS mutation typically associated with histologically follicular-patterned lesions with different stages of invasiveness, as opposed to BRAF and RET rearrangements, which have been associated with classical PTC. This suggests that NIFTP is an early non-invasive precursor of invasive encapsulated FVPTC (Fig. 1).
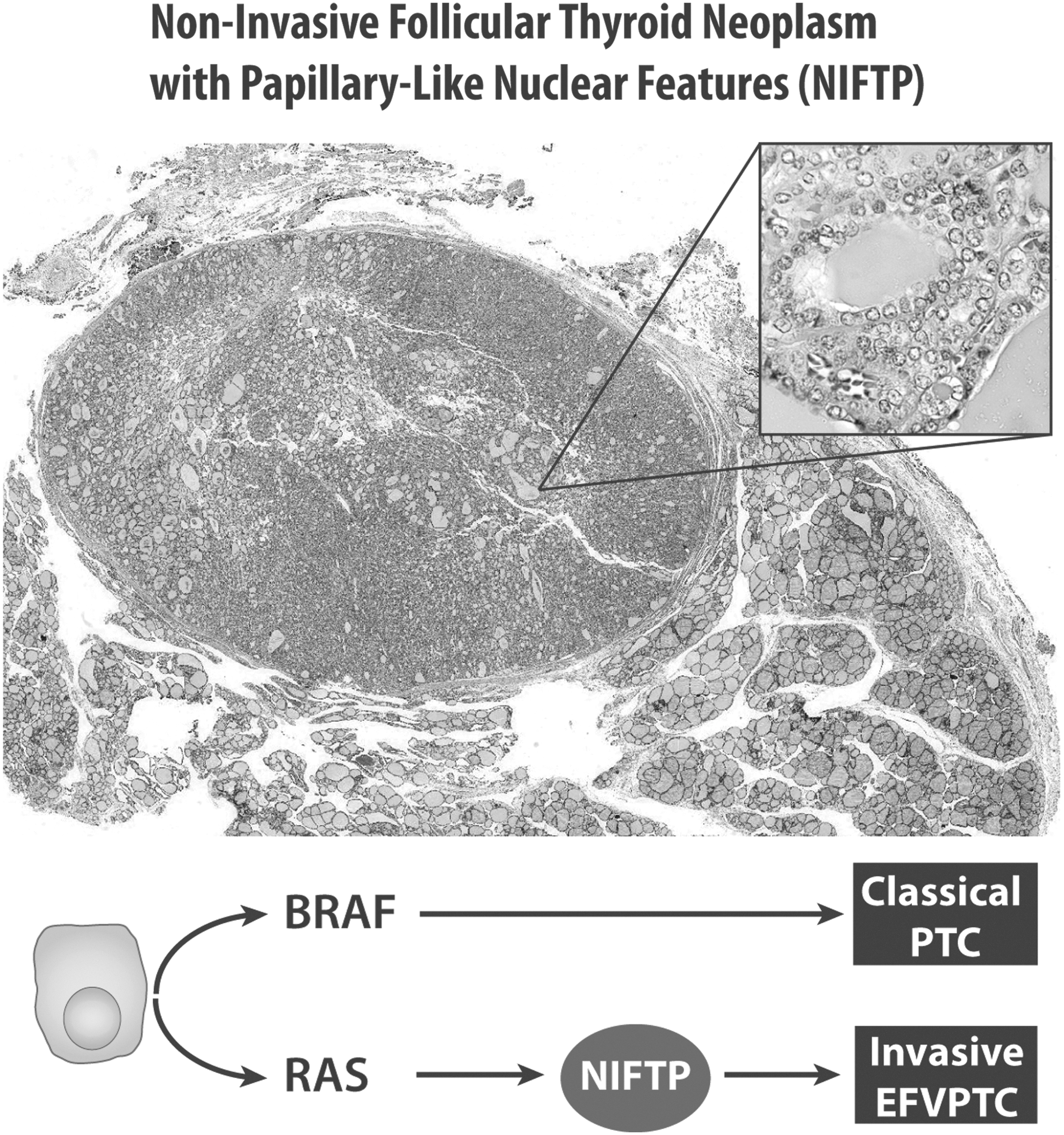
Non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is characterized by (i) encapsulation or clear demarcation of the tumor from adjacent thyroid tissue with no invasion, (ii) follicular growth pattern, and (iii) at least moderately expressed nuclear features of papillary carcinoma. NIFTP is driven by RAS and RAS-like mutations, and represents a pre-invasive stage of invasive encapsulated follicular variant of papillary thyroid cancer.
The new designation NIFTP acknowledges the very low malignant potential of these tumors by intentionally removing the word “cancer” from the designation. In our experience, the word “cancer” significantly impacts the way a disease is viewed and treated by clinicians, patients, and their families. The word “cancer” has strong association with “something evil or malignant that spreads destructively” as well as “death” (18,19). Use of this highly charged word too easily forces the clinician's hand, who engages all available treatment options aimed at the cancer's eradication for clinical, interpersonal, and medicolegal reasons (7,18). Such renaming is consistent with recent recommendations from a number of authors following a National Cancer Institute conference convened to address questions regarding cancer over-diagnosis (7). That publication advocated the need for nomenclature that better reflects the fact that “cancer” is actually a heterogeneous mix of diseases that range from inexorably fatal to indolent tumors and precursor lesions that have low and sometimes no true malignant potential. The term NIFTP recognizes that the continued use of “cancer” at best misrepresents the biological behavior of this tumor, and at worst will drive continued over-treatment, which exposes patients to unnecessary risks. It is estimated that >45,000 patients worldwide per year would benefit from a more rational and streamlined risk-appropriate NIFTP care while accruing significant morbidity reduction as well as cost and psychological benefits (8). NIFTP will be included in the upcoming 4th edition of World Health Organization (WHO) Classification of Tumors of Endocrine Organs.
We believe that the terminology change to NIFTP will also result in substantial cost savings. Significant cost reductions could be obtained by the avoidance of completion thyroidectomy and avoidance of RAI treatment, both of which are also associated with small though real risks of complications such as recurrent laryngeal nerve injury, superior laryngeal nerve injury, hypoparathyroidism, and secondary malignancies (20,21). Significant cost savings would also be realized by de-escalation of long-term surveillance with reduced office visits, as well as unnecessary ancillary radiographic and biochemical testing.
We are committed to our patients, and we believe that the language we use to describe this disease is important to both patients and physicians. NIFTP is a discrete and now well-studied histologic entity; extensive follow-up data justify omitting the highly charged word “cancer” and adoption of the new term NIFTP. This is not simply an exercise in academic etymology. We believe this change will have important clinical impact and better characterize a tumor that has very low malignant potential, and encourage a more restrained risk-adapted management. Through the consequent reduction in over-treatment and iatrogenic complications, and by lessening the emotional burden that we sometimes unintentionally inflict upon our patients, we will all be empowered to follow what is perhaps the most important dictum that guides us all—primum non nocere.
Societal Endorsements
The significant clinical implications of the NIFTP designation although just recently articulated have been widely understood in multiple surgical and endocrine organizations here and abroad. This has resulted in numerous societal endorsements that include the American Academy of Otolaryngology Head and Neck Surgery, American Head and Neck Society, the Endocrine Society, British Association of Endocrine and Thyroid Surgeons, Japanese Thyroid Association, International Neural Monitoring Study Group, World Congress on Thyroid Cancer, Latin American Thyroid Association, Brazilian Society of Head and Neck Surgery, and Brazilian Society of Endocrinology and Metabolism, underscoring the widespread medical endocrine and surgical appreciation of this lesion's clinical indolence and the important implications this name change conveys.