
Abstract
Background:
Critical illness is hallmarked by low circulating thyroxine (T4) and triiodothyronine (T3) concentrations, in the presence of elevated reverse T3 (rT3) and low-normal thyrotropin (TSH), referred to as nonthyroidal illness (NTI). Thyroid hormone (TH) metabolism is substantially increased during NTI, in part explained by enhanced deiodinase 3 (D3) activity. T4- and T3-sulfate concentrations are elevated, due to suppressed D1 activity in the presence of unaltered sulfotransferase activity, and 3,3′-diiodothyronine (3,3′-T2) concentrations are normal. To elucidate further the driving forces behind increased TH metabolism during NTI, two other potential T4 metabolites—3,5-diiodothyronine (3,5-T2) and 3-iodothyronamine (3-T1AM)—were measured and related to their potential TH precursors.
Methods:
Morning blood samples were collected cross-sectionally from 83 critically ill patients on a University Hospital intensive care unit and from 38 demographically matched healthy volunteers. Serum TH and binding proteins were quantified with commercial assays, and 3,5-T2 and 3-T1AM with in-house developed immunoassays.
Results:
Critically ill patients revealed, besides the NTI, a median 44% lower serum 3-T1AM concentration (p < 0.0001) and a 30% higher serum 3,5-T2 concentration (p = 0.01) than healthy volunteers did. Non-survivors and patients diagnosed with sepsis upon admission to the intensive-care unit had significantly higher 3,5-T2 (p ≤ 0.01) but comparable 3-T1AM (p > 0.2) concentrations than other patients did. Multivariable linear regression analysis adjusted for potential precursors revealed that the reduced serum 3-T1AM was positively correlated with the low serum T3 (p < 0.001) but unrelated to serum T4 or rT3. The elevated 3,5-T2 concentration did not independently correlate with TH.
Conclusions:
Increased TH metabolism during NTI could not be explained by increased conversion to 3-T1AM, as circulating 3-T1AM was suppressed in proportion to the concomitantly low T3 concentrations. Increased conversion of T4 and/or T3 to 3,5-T2 could be possible, as serum 3,5-T2 concentrations were elevated. Whether 3-T1AM or 3,5-T2 plays a functional role during critical illness needs further investigation.
Introduction
C
Sulfation of T4 and T3 is one such alternative pathway. However, although elevated levels of T4-S and T3-S have previously been documented in critically ill patients, these were predominantly attributed to suppressed D1 enzyme activity (13,17,18). While activity of D1 is decreased, which exclusively and rapidly deiodinates iodothyronine sulfates, sulfotransferase enzyme activity and expression were not increased during critical illness (13,18).
Thyronamines are a relatively novel class of potential T4 metabolites of which 3-T1AM has been detected in vivo (19,20). High doses of 3-T1AM can evoke hypothermia and bradycardia (19,20). The biosynthesis pathways of 3-T1AM are not completely clarified, although in vitro thyronamines are isozyme-specific substrates for deiodinases and intestinal decarboxylation of TH by ornithine decarboxylase has been observed (21,22). Athyreotic patients on levothyroxine (LT4) replacement therapy also had higher serum 3-T1AM concentrations than individuals did with intact thyroid, indicating its extrathyroidal formation from supplemented LT4 (23). The TH metabolite 3,5-T2, which is theoretically formed through D1 deiodination of T3, has long been considered as a physiological inactive and minor metabolite of T4 and T3, but recent studies indicate that this metabolite might have a physiological impact on energy metabolism (24 –28).
To elucidate further the driving forces behind increased TH metabolism during the NTI of critical illness, this study investigated the impact of critical illness on these two potential T4 metabolites—3,5-T2 and 3-T1AM—and their association with potential precursor TH. In a cross-sectional observational study, morning blood samples were collected from 83 surgical intensive care unit (ICU) patients and 38 demographically matched healthy control individuals in order to quantify serum concentrations of total T4 (TT4), total T3 (TT3), rT3, and 3,5-T2 and 3-T1AM. Because free hormone levels could not be determined accurately, as patient samples were collected through heparinized arterial lines, thyroxine binding globulin (TBG) and Apolipoprotein B, the primary carrier of 3-T1AM in the circulation, were quantified (29,30).
Material and Methods
Patients
On five consecutive collection days (with five days between each collection), morning blood samples were taken from all patients who were admitted to the surgical ICU and for whom informed consent was given by the patient or the next of kin. Those patients who were still in the ICU on more than one collection day were only included once in the study. Undiluted blood samples were collected at 6:00am via an arterial catheter in place for clinical purposes. After sampling and centrifugation, serum was kept frozen at −80°C until batched analysis. As healthy references, morning blood samples were collected by venipuncture from 38 overnight-fasted healthy volunteers with demographics that were comparable to the patient population (Table 1). The study protocol and consent forms were approved by the Institutional Ethical Review Board (approval number ML2112 and ML4190).
Complicated surgery indicates patients suffering from complications after abdominal or pelvic surgery, pulmonary or esophageal surgery, or vascular surgery. The Acute Physiology and Chronic Health Evaluation II (APACHE II) score reflects severity of illness, with higher values indicating more severe illness, and can range from 0 to 71 (43).
ICU, intensive care unit; SE, standard error; BMI, body mass index; IQR, interquartile range.
Quantification of circulating hormones, metabolites, and binding proteins
The serum concentrations of the metabolites 3-T1AM (23) and 3,5-T2 (28,31) were quantified with in-house developed monoclonal-antibody based chemiluminescence immunoassays, partly adapted from previously described. For the 3-T1-AM assay, plates were now coated with 3-T1AM-labeled bovine serum albumin (BSA; 50 μg in 0.1 mL per well; overnight at 4°C), instead of coating with a polyclonal rabbit anti-mouse IgG (H&L) as capture antibody, to minimize cross-reactivities between antibodies. The same previously used (23) monoclonal antibody (mAb) for 3-T1AM was now biotinylated (10 ng in 0.05 mL per well). Incubation time (1.5 h at 750 rpm) and serum volume (25 μL per determination) remained unchanged. The detection system consisted of streptavidin-labeled Europium, binding to the biotin label and producing a stable fluorescence signal for quantification. The modified 3-T1AM assay is now characterized by a limit of detection <1 nM (0.93 nM). The 3-T1AM values were calculated from a log-transformed standard calibrator curve (0.5–50 nM, R
2 = 0.99) in artificial serum matrix composed of 7% BSA (w/v) in 10 mM phosphate-buffered salt solution, pH 7.2, containing 0.02% Tween 20 (Supplementary Fig. S1; Supplementary Data are available online at
Statistical analysis
Parametrical Student's t-tests and non-parametrical Mann–Whitney U-tests were used to analyze differences between control subjects and ICU patients, as appropriate for normally and non-normally distributed data, respectively. Non-normally distributed data were analyzed with parametric tests if after log- or (double) square root-transformation, this resulted in a near-normal distribution. With univariable and multivariable linear regression analyses, the presence of an independent association between serum 3-T1AM, 3,5-T2, and their respective potential precursors was assessed. The presence of multicollinearity among the regressor variables of the multivariable regression analyses was excluded using the tolerance, variance inflation factor, condition indices, and variance proportions (33). All statistical analyses were performed with JMP12 for Windows (SAS Institute, Inc., Cary, NC). Statistical significance was set at a two-tailed p-value of ≤0.05.
Results
Circulating thyroid hormones, metabolites, and binding proteins
Healthy control subjects and ICU patients had comparable demographic characteristics (Table 1). Samples were collected from a diverse group of surgical ICU patients after a variable time spent in the ICU (Table 1). All ICU patients demonstrated serum TT3 concentrations below that of the healthy controls (Fig. 1C). The mean serum TT4 concentration was also lower in the ICU patients in the presence of low mean serum TSH (Fig. 1A and B). In contrast, the mean rT3 serum concentration was significantly higher in ICU patients compared with healthy controls (Fig. 1D).

Comparison of serum thyroid hormone (TH) concentrations for healthy control subjects and intensive care unit (ICU) patients. The panels represent serum thyrotropin (TSH;
The serum concentrations of the metabolite 3-T1AM were significantly lower in ICU patients than they were in healthy control subjects (Fig. 2A). In contrast, the serum concentrations of 3,5-T2 were significantly higher in ICU patients than they were in healthy controls (Fig. 2B). Furthermore, patients who eventually did not survive their ICU stay displayed higher serum 3,5-T2 concentrations than ICU survivors did (Fig. 2D), whereas surviving and non-surviving ICU patients had comparable 3-T1AM concentrations (Fig. 2C). Furthermore, patients diagnosed with sepsis upon admission had higher serum 3,5-T2 (p = 0.006) than patients who did not have a sepsis diagnosis on admission, but comparable serum 3-T1AM concentrations (p = 0.6).
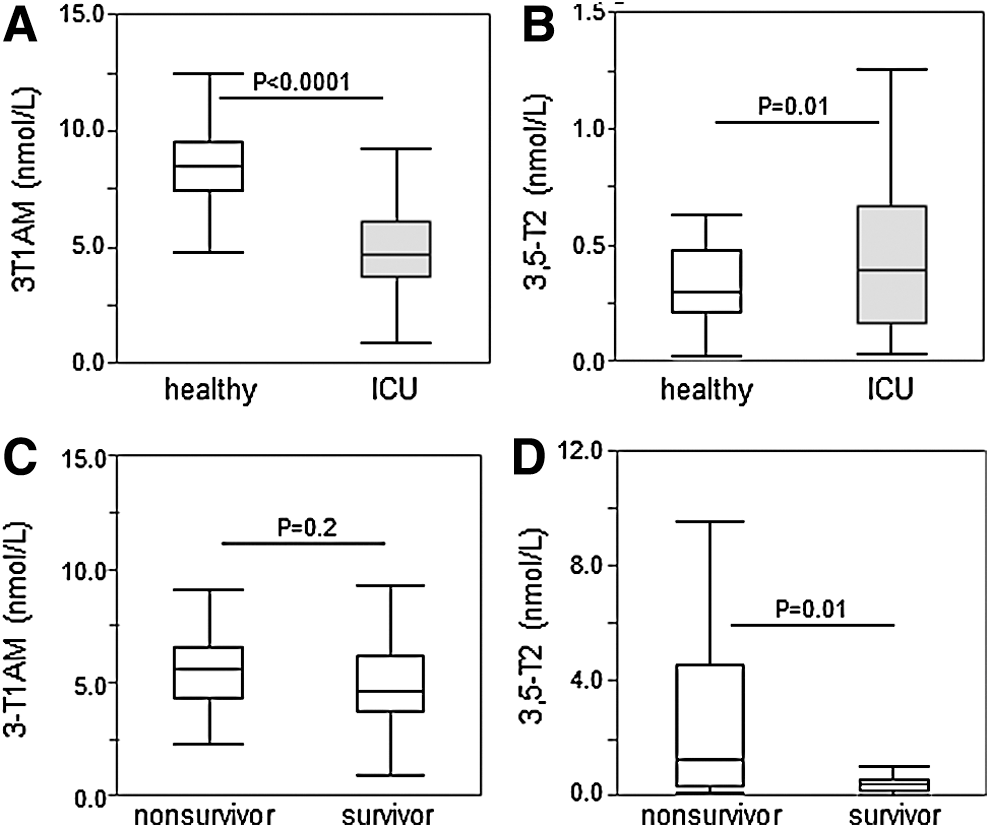
Comparison of serum 3-T1AM and 3,5-T2 in healthy control subjects and ICU patients. The upper panels represent serum 3-T1AM (
The serum TBG concentration was significantly lower in ICU patients than it was in healthy controls (Fig. 3A). Because serum 3-T1AM predominantly resides in ApoB100 containing low-density lipoproteins (29), the serum ApoB concentration was also quantified, which was comparable in healthy control subjects and ICU patients (Fig. 3B).
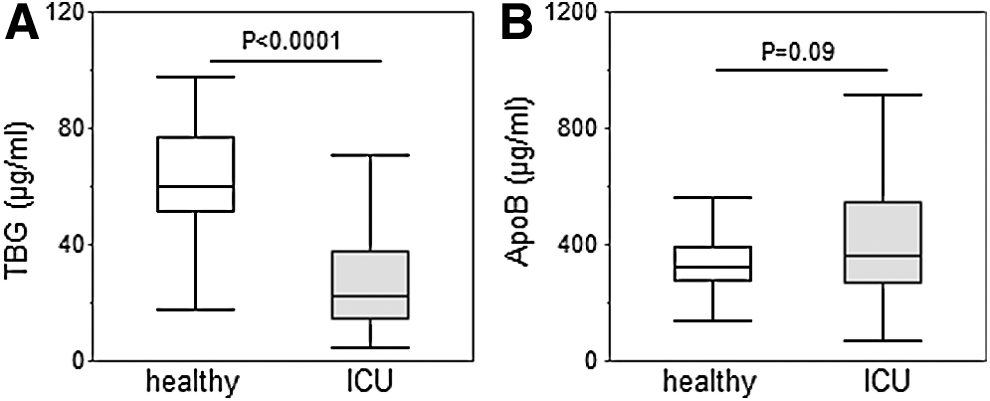
TH binding proteins. The panels represent serum thyroxine binding globulin (TBG;
Univariable and multivariable regression analysis
To assess the relationship between the two novel metabolites and potential TH precursors, first univariable regression analyses were performed. In univariable analysis, 3-T1AM was significantly positively correlated with T4 and T3, and negatively with rT3 and 3,5-T2 (Table 2). In univariable analysis, the metabolite 3,5-T2 was negatively, albeit weakly, correlated with its putative precursors T4 and T3 (Table 3). Because the concentrations of these hormones are related to each other, a multivariable regression analysis was also performed, adjusting for the studied potential precursor hormones. This analysis indicated that only total T3 was independently and positively correlated with 3-T1AM (for each nmol/L increase of TT3, 3-T1AM had an estimated increase of 2.22 nmol/L, p 0.001; Table 2). The weak association between T3 or T4 and 3,5-T2 was no longer present in the multivariable regression analysis, adjusted for all studied precursor TH (Table 3).
TH, thyroid hormone; CI, confidence interval; TT4, total thyroxine; TT3, total triiodothyronine; rT3, reverse T3.
Discussion
This cross-sectional observational study demonstrates that critically ill patients with NTI have a median 44% lower serum 3-T1AM concentration, in proportion to the concomitantly low T3 concentrations, and a median 30% higher serum 3,5-T2 concentration than matched healthy control subjects have. Enhanced TH metabolism during NTI could thus not be explained by an increased conversion to 3-T1AM. Increased deiodination of T4 and/or T3 to 3,5-T2 could contribute to the high TH turnover during NTI of critical illness.
It was hypothesized that during critical illness, T4 is not only metabolized to rT3, but also that other metabolites might be increased during critical illness (13,16). This hypothesis was based on previous findings in critically ill patients and animals, where T4 substitution could not normalize T4 or T3, and this without a concomitant change in T3, rT3, or 3,3′-T2 (10 –13). Two potential metabolites with physiological activities—3,5-T2 and 3-T1AM—were therefore investigated.
A median 30% increased 3,5-T2 concentration was observed in critically ill patients, particularly in patients with an unfavorable outcome. Also in cardiac surgery patients, patients with sepsis, liver cirrhosis, and brain tumors with NTI, 3,5-T2 concentrations have been reported to be elevated (31,34). Thus, during critical illness, part of T4 and T3 might indeed be metabolized to 3,5-T2. In theory, D1 could catalyze the conversion from T4 to T3 to 3,5-T2. However, regression analysis indicated only a weak univariable association between both T3 and T4 and 3,5-T2. Furthermore, hepatic D1 activity is reduced in critically ill patients (7). However, clear evidence on which deiodinases are involved in the formation and further metabolism of 3,5-T2 is currently lacking. It is possible that D2, which was previously reported to be upregulated in the muscle of prolonged critically ill patients, might also be involved (35). In addition to an increased conversion of T3 and/or T4 to 3,5-T2, a decrease in 3,5-T2 metabolism or a decreased tissue uptake might also (partly) explain the increase in circulating 3,5-T2. Which pathways, compartments, or organs might be involved in the generation and metabolism of 3,5-T2 and whether 3,5-T2 plays a functional role during critical illness is beyond the scope of this observational study, but needs further investigation.
In contrast with 3,5-T2, a median 40% lower serum 3-T1AM concentration was observed in critically ill patients compared with healthy controls. It thus seems unlikely that an increased decarboxylation of T4 or T3 plays a role in the development of NTI or in the elevated TH turnover. The concentration of 3-T1AM independently correlated with serum T3 only, which suggests that its decreased concentration is likely due to a decreased availability of T3 as precursor. A univariable correlation between 3T1-AM and T3 was also observed in a mixed population of patients suffering from cardiac or thyroid disease (36), whereas no correlation to T3 was observed in two smaller observational studies in cardiac surgery patients with NTI (31) or patients on T4 substitution (23). Decreased conversion of 3,5-T2 to 3-T1AM might theoretically also have played a role, suggested by the (univariable) negative correlation of both metabolites. Indeed, in vitro conversion from 3,5-T2 to 3-T1AM has been demonstrated before (22). However, 3-T1AM is also a substrate for D3, and could thus have been further deiodinated (21). Furthermore, although the biosynthesis pathways of 3-T1AM are not completely clear, intestinal decarboxylation by ornithine decarboxylase and deiodination has been observed (22), and intestinal activity of ornithine decarboxylase is increased in septic animals (37). Thus, a tissue specific increase in 3-T1AM, not reflected in the circulating levels, cannot be excluded. Alternatively, oxidative deamination of 3-T1AM might be an alternative pathway involved in bringing about low T3 and low 3-T1AM, which warrants further investigation (38). Furthermore, conjugation of 3-T1AM to sulfates has been reported in vitro (39). Whether altered enterohepatic recycling of TH in critical illness contributes to these inverse changes in 3,5-T2 and 3-T1AM serum concentrations remains to be clarified.
The largest part of circulating T4 and T3 is bound to carrier proteins, of which TBG is the dominant binding protein (40). The observed decreased serum TBG concentration, but also decreased serum albumin, commonly found in critically ill patients, might have increased the amount of circulating free 3,5-T2, but its binding to serum TH distributor proteins is not well characterized. Different from circulating T3 and T4, 3-T1AM resides predominantly in the ApoB100 containing low-density lipoprotein fraction, which also can affect its intracellular uptake (29). As the serum ApoB concentration in patients was comparable to that of healthy controls, an effect on 3-T1AM bioavailability during critical illness or decreased (free) serum concentrations are less likely. Because 3-T1AM is largely bound to the carrier protein ApoB100 (29), it is speculated that this might also have played a role in the much lower 3-T1AM concentrations found with mass spectrometry (36) compared with the values quantified with the immunoassay in the sera of healthy controls. For the LC-MS/MS analysis, serum samples were deproteinized and lipid depleted, which might have removed the largest part of bound 3-T1AM from the sample (36). This would suggest that the LC-MS/MS method would represent the “free/non-bound 3-T1AM fraction,” whereas the immunoassay might have detected the (nearly) total 3-T1AM fraction in human serum. Of course, the ratio and concentration of the reported TH metabolites in serum might not adequately reflect steady-state concentrations in the tissues. Indeed, 3-T1AM appears to accumulate in peripheral tissues such as the liver, heart, kidney, and muscle at much higher levels than in circulation, but also 3,5-T2 has been reported to accumulate in mouse liver after exogenous administration (41,42).
In conclusion, critically ill patients not only suffer from low T4 and T3, but 3-T1AM is also decreased. On the contrary, in addition to the increased conversion of T4 to rT3, enhanced metabolism to 3,5-T2 might also play a role in the development of NTI. Whether 3-T1AM or 3,5-T2 plays a functional role during critical illness or contributes to its manifestation needs further investigation.
Footnotes
Acknowledgments
We thank the volunteers, the patients, and their family members for participating in this study. G.V.d.B., via the University of Leuven (KU Leuven), receives long-term structural research support from the Methusalem Program funded by the Flemish Government (METH/08/07 and METH/14/06) and holds a European Research Council Advanced Grant AdvG-2012-321670 from the Ideas Program of the European Union seventh framework program. J.K. and I.L. are supported by research grants from the Priority Programme 1629 ThyroidTransAct (KO 922/16-2 and 922/17-1/2) funded by the Deutsche Forschungsgemeinschaft DFG and grants from the Charité-Universitätsmedizin Berlin.
Author Disclosure Statement
The authors have declared that no conflict of interest exists.