
Abstract

Graves' disease (GD) is the most common cause of hyperthyroidism (1). There are three treatment modalities for GD: antithyroid drugs (ATD), radioactive iodine (RAI), and surgery. These options differ in their efficacy, safety, convenience, and cost (2). No treatment option is clearly superior to the others for everyone. Clinicians in Europe and Asia prefer to prescribe ATDs, while clinicians in the United States prefer RAI (3). The extent to which clinician preferences translate into practice is unknown.
We conducted a retrospective analysis of administrative claims data from Optum Labs Data Warehouse, which includes privately insured and Medicare Advantage enrollees throughout the United States, to characterize the treatment choice patterns for patients with GD. We included patients aged ≥18 years for whom surgery, RAI, or ATD was their first definitive treatment for GD between 2004 and 2013. We required patients to have a least one diagnosis code for GD in the 12 months preceding any of these treatments (International Classification of Diseases [ICD-9-CM] 242.00, 242.01). Patients with hyperthyroidism or with the diagnosis of thyroid cancer anytime in the year prior to their GD diagnosis were excluded. All individuals had continuous enrollment in their medical and pharmacy plans for at least 12 months prior to their treatment. To classify accurately patients who could have received ATD as pre-RAI or surgical therapy, patients receiving ≤60 days of ATD and switched to another therapy were analyzed as receiving the definitive therapy, not as receiving ATD. Patient baseline characteristics (i.e., age, sex, race/ethnicity) were noted. A multinomial logistic regression model was used to test the relation between these factors and treatment choice.
We identified 8217 patients, with a mean age of 47 ± 14.4 years, who were mostly white (62%) and female (79%). ATD was the most commonly used treatment in this cohort (58%; methimazole 87%, propylthiouracil 13%) followed by RAI (35%) and surgery (6%; see Fig. 1). Compared with patients who received RAI, ATD patients were more likely to be younger, to have fewer comorbidities, and to be pregnant; surgery patients were less likely to be male, Hispanic, to have greater comorbidity, and to receive care in the Northeast and South U.S. regions (Supplementary Table S1; Supplementary Data are available online at
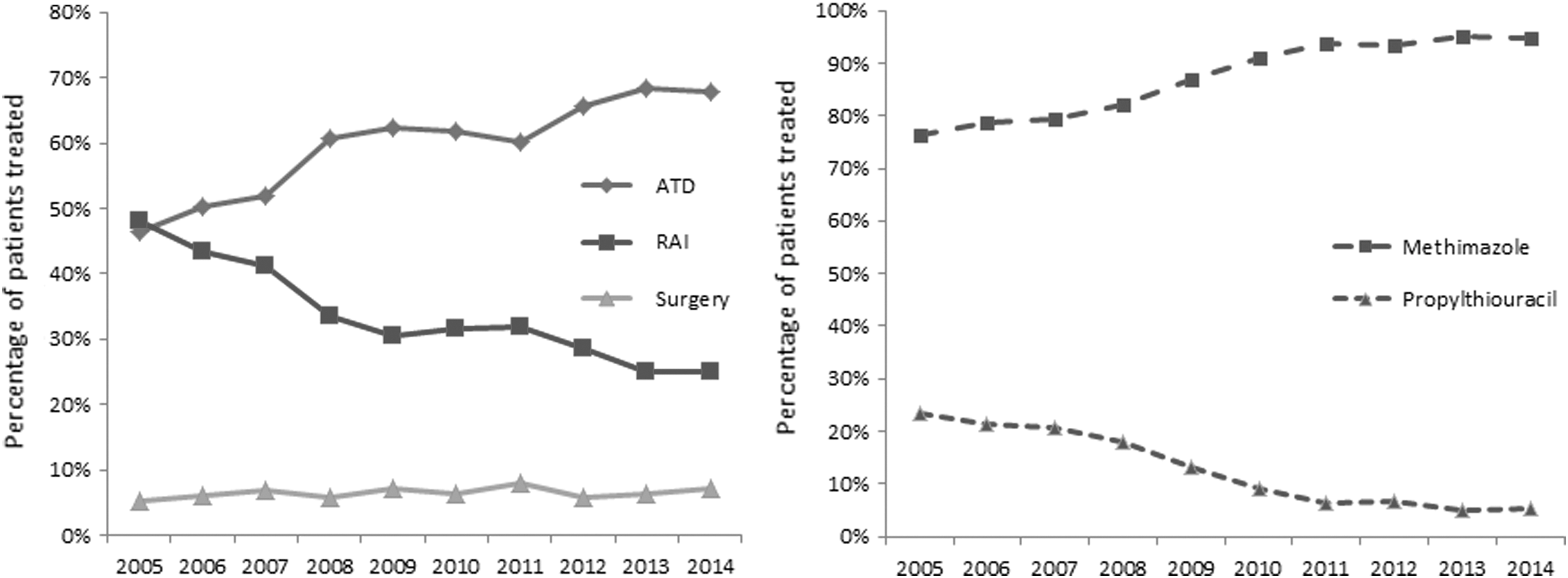
Left: Percentage of treatment choice by year. Right: Percentage of ATD treatment drug choice by year.
The most common treatment of GD in commercially insured patients in the United States today is ATD. An increase of ATD use started in 2005 at the expense of RAI use (Fig. 1). Preference to prescribe methimazole over propylthiouracil may reflect its ability to control thyrotoxicosis quickly and the recognition of propylthiouracil's adverse safety profile (4). While we identified several variables associated with treatment choice, other factors (e.g., smoking status, 24-hour RAI uptake results, goiter size, thyroid nodularity) were not assessed due to lack of clinical and laboratory detail in this administrative data set. These estimates differ from the results of clinician surveys of treatment preferences, hinting at the probably major role other factors, such as treatment availability, local expertise, and incentives, have in shaping the nature and frequency of post-treatment follow-up. To our knowledge, the role informed patient preferences play in treatment selection also remains unknown.
Footnotes
Acknowledgments
This study was funded by the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN.
Author Disclosure Statement
No competing financial interests exist.