
Abstract
Background:
Lymph node (LN) recurrence detected by ultrasound (US) is a very common problem after initial treatment for papillary thyroid carcinoma (PTC). Most patients with PTC have an excellent disease-specific survival even with LN recurrence. Recently, watchful waiting with serial cervical US evaluations would be considered a reasonable approach to management of LN recurrence in selected patients. On the other hand, some patients with LN recurrence have demonstrated clinically significant disease progression during follow-up. The objective of the present study was to document the changes of cervical LN metastases after initial treatment and identify useful information for deciding how best to manage individual patients with LN recurrence.
Methods:
This retrospective review identified 83 consecutive PTC patients with at least one LN on the postoperative US diagnosed with fine needle aspiration biopsy or the thyroglobulin titer in the wash-out of the needle. The change in LN size was determined using serial US studies over time.
Results:
The subjects were 15 men and 68 women, with a median age at initial surgery of 50.6 years (range, 18–80 years). The median LN size at the start of the observation period was 1.3 cm (range, 0.5–2.4 cm) in the largest diameter. After a median follow-up of 7.2 years, the median growth rate of the nodes showing structural progression was 1.4 mm per year (range, 0–12.0 mm/year). Seventeen of 83 patients (20.5%) demonstrated an increase in LN size of at least 3 mm, only 8.4% (7 of 83) had an increase of at least 5 mm, and 39.7% (33 of 83) resolved. Distant metastases were present in 11 of 83 patients. Ten-year and fifteen-year disease-specific survival rates after diagnosis of LN recurrence were 84.7% and 72.6%, respectively. Older age and recurrent LN growth of more than 3 mm/year were recognized as independent predictors for short survival on both univariate and multivariate analyses (p < 0.05).
Conclusions:
Most lymph node recurrences may remain stable for a long time and not be immediately life-threatening. However, recurrent LN growth of more than 3 mm per year could be related to mortality.
Introduction
M
Materials and Methods
After obtaining approval from our institutional review board, US reports for PTC patients who had at least one neck US study during their follow-up at Ito hospital between October 2003 and January 2014 were retrospectively reviewed. Of the reports initially reviewed, 189 patients with PTC after initial surgery had an abnormal LN identified on consecutive US studies. Suspicious malignant US features included marked hypoechogenicity, microlobulated, irregular margin, microcalcifications, and a taller than wide shape. Of these patients, 83 PTC patients with at least one cervical recurrent LN were diagnosed by postoperative US with fine needle aspiration biopsy or the thyroglobulin titer in the washout of the needle (FNAB-Tg) (6) and met the inclusion criteria. Reasons for exclusion included patients with LNs less than 5 mm in the minimum dimension who did not undergo fine needle aspiration biopsy. Patients with poorly differentiated histology, markedly PET-positive disease, and LNs more than 3 cm in size were not routinely offered the option of active surveillance. Patients who were followed for less than one year after diagnosis for recurrent LN metastasis, had distant metastasis at initial treatment, systemic therapy or previous external beam radiotherapy, or had insufficient data were excluded from this study.
All of these patients underwent thyroidectomy (total or limited thyroidectomy) and prophylactic central node dissection and/or lateral neck LN dissection at initial surgery. Patients were usually followed every 3–4 months during the first year and at 6- to 12-month intervals thereafter at the discretion of the attending physician based on the clinical course of the disease. After diagnosis of LN recurrence, patients were followed every 3–6 months to monitor them for size changes on US. US examinations were performed using high-resolution US machines equipped with a 7.5-, 8-, or 12-MHz linear probe (Aplio XG or MX or 400, Toshiba, Tokyo, Japan). For a patient having multiple LN metastases, the size of the larger tumor was used for this study. LN growth was defined as an increase of at least 3 mm per year in the largest dimension when compared with the size of the node at detection. A 3-mm increase was selected because this is the minimal size change that can be reproducibly determined by high-resolution US while minimizing operator-dependent differences in size assessment.
Statistical analysis was performed using a statistical software program (JMP12.0; SAS Institute, Inc., Cary, NC). Fisher's exact analysis was used for univariate analysis. Disease-specific survival (DSS) was evaluated using the Kaplan-Meier method, and survival time was measured from the date of LN recurrence to the date of last follow-up. Univariate analysis for DSS was conducted by the Kaplan-Meier method for the variables of sex, age at initial diagnosis, and age at LN metastasis. Differences between groups were analyzed for significance by the log-rank test. For multivariate analysis, multivariate logistic analysis was performed. Hazard ratios for each category were calculated, and a p-value smaller than 0.05 was considered significant.
Results
The subjects were 15 men and 68 women, with a median age at initial surgery of 50.6 years (range, 18–80 years). Median duration between initial surgery and diagnosis of LN recurrence was 3.7 years (range, 1–16 years). Table 1 presents the clinicopathologic features of the 83 patients with LN metastasis on routine follow-up neck US after initial surgery. Initial therapy included total thyroidectomy in 48.2% of patients and central neck dissection in 100% of the patients. Ten patients (12.0%) had massive extrathyroid extension. The number of LNs removed ranged from 0 to 28, with a median of 5 LNs resected per patient. A histological diagnosis of classical papillary thyroid carcinoma was made at the primary operation in all cases.
CND, central neck dissection; ND, neck dissection; UICC, Union for International Cancer Control.
The median LN size in the largest diameter at the start of the observation period was 1.3 cm (range, 0.5–2.4 cm). Follow-up for LN recurrence ranged from 16 to 98 months (median follow-up period, 86 months). The median rate of LN growth showing structural progression was 1.4 mm/year (range, 0–12.0 mm/year). Seventeen of 83 patients (20.5%) demonstrated an increase in LN size of at least 3 mm per year, while only 8.4% (7 of 83) had an increase of at least 5 mm per year. Distant metastases were present in 11 of 83 patients after initial treatment (13.2%). The distant metastatic sites were lung (n = 9), bone (n = 2), brain (n = 1), and skin (n = 1). For treatment of distant metastases, 10 patients received ablation and/or therapeutic doses of radioiodine ranging from 1.9 to 33.3 GBq. Postoperative thyrotropin suppression therapy was performed selectively in 44 patients with distant metastases, extrathyroidal massive invasion, or a second recurrence.
Thirty-three patients (39.7%) underwent surgical treatment for various reasons after a median follow-up of 2.8 years (range 2–6.9 years). The leading reason for surgery was LN enlargement (17 patients). The median LN size in the largest diameter at the operation for LN recurrence was 2.2 cm (range, 1.5–3.2 cm). Eight of the 17 patients also showed new LN metastases. Nine patients underwent surgery because multiple new LNs suspicious for malignancy appeared during follow-up, though the LN enlargement was less than 3 mm per year. Seven patients underwent surgery after observation at their choice, even though LN metastasis was stable. Six patients who had a second recurrence after reoperation underwent a third operation, three of whom underwent a fourth operation for a third recurrence. Twenty-one LN metastases were in a previously formally dissected compartment, and the others were in an area that was not formally dissected. They had no fatal complications after reoperation. After the second surgery, all cases were pathologically confirmed as metastatic classical PTC. LN metastasis of one patient who had a third recurrence was diagnosed as poorly differentiated carcinoma.
The relationships between LN growth and various clinicopathological features were investigated (Table 2). Patients with LN growth of at least 3 mm per year were more likely to have older age and larger LN size at study entry. Based on p-values on multivariate logistic analysis, no factor, such as advanced age, distant metastasis, tumor size larger than 4 cm, and the number of LN metastases at initial surgery, was related to LN growth (Table 3).
Reference values: TSH, 0.2–4.5 mIU/L.
LN, lymph node; TSH, thyrotropin.
CI, confidence interval.
For PTC patients with LN recurrence, 10-year and 15-year disease-specific survival (DSS) rates after initial surgery were 96.1% and 90.1% respectively (Fig. 1A), while 10-year and 15-year DSS rates after diagnosis of LN recurrence were 84.7% and 72.6% (Fig. 2A) respectively. Advanced age showed a significant direct correlation with DSS after initial treatment (Fig. 1B), but primary tumor size at initial surgery did not (Fig. 1C). Recurrent LN growth of more than 3 mm per year showed a significant direct correlation with DSS after LN recurrence, while larger LN size (more than 1.5 cm) at the start of the observation period showed no correlation with DSS after LN recurrence (Fig. 2B, C). Table 4 shows the results of multivariate logistic analysis for factors predicting a poor survival rate. Older age and the speed of recurrent LN growth (more than 3 mm/year) were related to short survival.
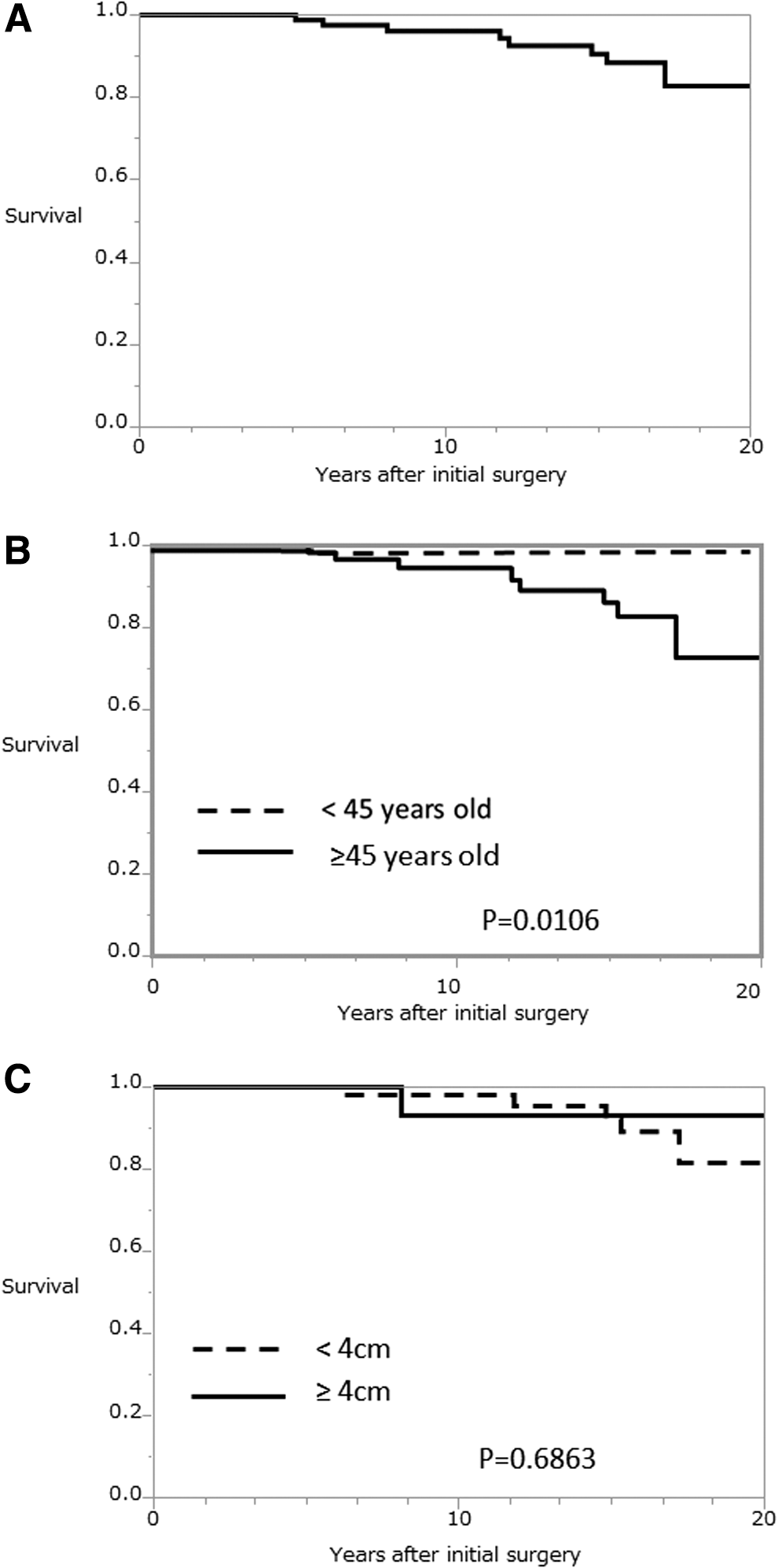
Disease-specific survival (DSS) curve after initial treatment of 83 papillary thyroid carcinoma patients with lymph node recurrence (
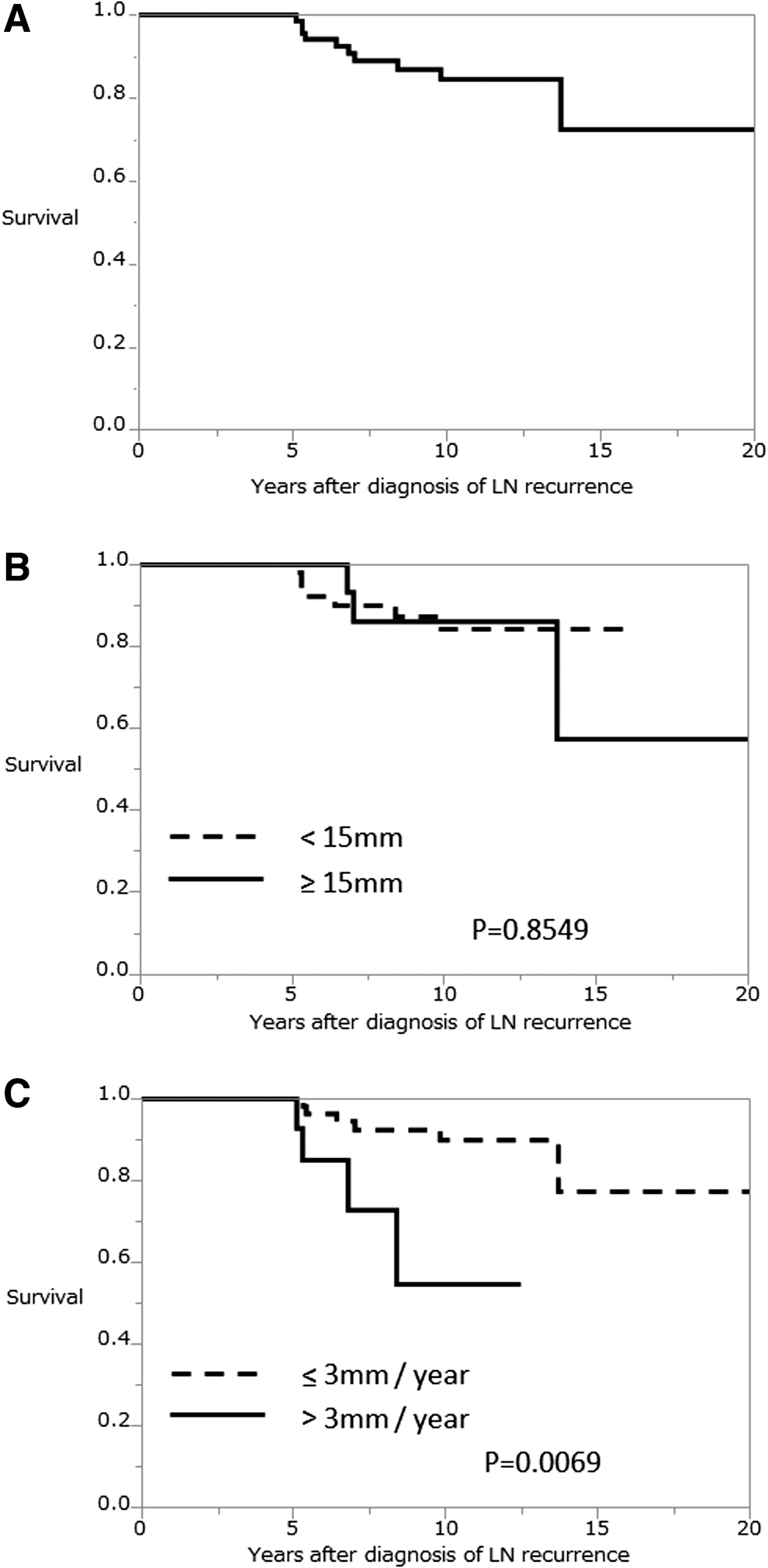
DSS curve after diagnosis lymph node recurrence (
Discussion
There are two types of prognostic factors for PTC, static and dynamic. The following static prognostic factors have been conventionally accepted: age, tumor size, extrathyroidal massive extension, LN metastasis, and distant metastasis based on pre-, intra-, and postoperative findings (7,8,9). These factors are useful for deciding therapeutic strategies for PTC patients, including the extent of surgery and radioactive iodine ablation. In contrast, the dynamic prognostic factors are based on changes in US, CT scans, physical examination, and the serum thyroglobulin values and/or thyroglobulin antibodies in patients who have undergone a total thyroidectomy (10). It is very important to evaluate whether and how recurrent lesions progress in real time. We suggest that the change in recurrent LN size by serial cervical US evaluations could be another useful dynamic prognostic factor for survival.
The detection of small LN metastases after initial treatment for PTC is the most common problem (1,4,11). US is not using ionizing radiation, has no known side effects, and is widely available. The earlier detection of LN recurrence is due to the increased use of office-based US. LN recurrence is easily diagnosed by US-guided fine-needle aspiration biopsy and the thyroglobulin titer in the washout of the needle (FNAB-Tg) (6). The first suspicious recurrent LN following measurement of the change of the size by US can be accepted as the most reasonable criterion for deciding on the need for further examination. If the size of the LN is increasing more than 3 mm per year, a fine needle aspiration biopsy and surgical intervention would be considered. In the present study, cases of suspicious LN recurrence by US underwent fine needle aspiration when the size of the LN in the largest diameter was more than 10 mm and the growth speed of LN size was greater than 3 mm per year.
Intervention for recurrent metastatic LNs should be discussed in detail with each patient. The clinicians must determine the appropriate therapeutic approach, which may include surgical resection in experienced hands, observation with or without thyrotropin suppressive therapy with thyroid hormone, radioactive iodine therapy, external beam radiation therapy, and/or tyrosine kinase inhibitors (TKIs). Theoretically, there may be benefit derived from removing these LNs to prevent de novo distant metastases as well, although this has not been proven. We have to understand the risks and benefits of each therapy, including observation, depending on the recurrence site and patient-related factors. The National Comprehensive Cancer Network panel agrees that surgery is the preferred therapy for locoregional recurrent disease. Patients with a recurrent metastatic LN with evidence of invasion or concern for likely invasion into major anatomic structures (internal jugular vein, carotid artery, esophagus, recurrent laryngeal nerve) would undergo surgical removal. However, surgery itself can sometimes decrease a patient's quality of life because of iatrogenic uni- or bilateral vocal cord paralysis. It should also be made clear that surgical removal of metastatic cervical LNs has been reported to have no impact on overall survival (12 –14). Other therapies such as external beam radiation therapy and/or TKIs decrease morbidity rather than completely cure patients, but they may be associated with side effects. The National Comprehensive Cancer Network guidelines suggest that external radiation therapy improves outcomes for unresectable, locoregional disease inadequately responsive to radioiodine. TKI initiation should be considered when no other approaches can control progressive or symptomatic disease (15,16). The therapy should be continued for as long as net benefit exceeds net harm. TKIs also have a high probability of side effects; they can worsen quality of life by cutaneous alterations, aerodigestive fistulas, and carotid rupture, among others. The risk versus benefit of starting a TKI should therefore be carefully weighed.
Conclusion
Most LN recurrences remain stable for a long time, and patients with papillary thyroid carcinoma have an excellent disease-specific survival even with LN recurrence. However, recurrent LN growth of more than 3 mm per year could be related to mortality. The velocity of LN metastasis growth after thyroidectomy for papillary thyroid carcinoma is very helpful for deciding how best to manage individual patients with LN recurrence.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest in relation to this manuscript.