
Abstract
Background:
Programmed death-ligand 1 (PD-L1) expression has been reported in several malignancies, but the expression of PD-L1 in papillary thyroid cancer (PTC) has been characterized rarely. The aim of this study was to assess the significance of PD-L1 expression and its associations with clinicopathologic factors and disease outcome in PTC.
Methods:
Immunohistochemistry staining was conducted retrospectively to evaluate the expression of PD-L1 in a total of 260 PTC tumors and corresponding non-tumor tissues. The correlations between PD-L1 expressions with clinicopathologic features and recurrence-free survival (RFS) were analyzed.
Results:
PD-L1 expression was positive in 52.3% (136/260) of PTC tumor tissues, which was significantly higher than in corresponding non-tumor thyroid tissues. In clinicopathologic analyses, this positive staining of PD-L1 was positively linked to multifocality (p = 0.001) and extrathyroidal extension (p = 0.001). In multivariate Cox regression analysis, positive PD-L1 expression in tumor tissue was significantly associated with worse RFS (hazard ratio 2.825 [confidence interval 1.149–6.943], p = 0.024). In subgroup analyses based on clinicopathologic factors, positive PD-L1 staining of tumor tissue was associated with worse RFS in males (p = 0.001), older patients (≥45 years; p = 0.001), and patients with a primary tumor size >4 cm (p = 0.002), multifocal tumors (p = 0.031), extrathyroidal extension (p = 0.012), and lymph node metastasis (p = 0.004). In contrast, positive PD-L1 staining predicted worse RFS in the subgroup of patients without Hashimoto's thyroiditis (p = 0.001) and treated with total thyroidectomy (p = 0.019).
Conclusions:
PD-L1 is important in determining aggressiveness of PTC and could predict the prognosis of patients. Therefore, inhibition of PD-L1 is suggested as a potential strategy for the treatment of advanced PTC with high expression of PD-L1.
Introduction
T
A series of traditional factors have been identified to be associated with aggressive behaviors in previous studies, which are crucial in risk stratification and decision making for the management of TC (2,3). Recently, it has also been suggested that novel molecular-based classification could tackle this challenge effectively. For example, BRAFV600E and TERT promoter mutations could define PTC with worse clinical outcomes, so as to providing prognostic and therapeutic implications (4,5). Thus, the molecular characterization and identification of patients with PTC is thought to be a key aspect for future study.
One of the new promising molecular targets in different types of malignancies is programmed death-1 receptor (PD-1; CD279) and its ligand (PD-L1; B7-H1; CD274), which deliver inhibitory signals that regulate the balance between T-cell activation, tolerance, and immune-mediated tissue damage (6). PD-L1 is induced on epithelial cells and also expressed on various tumor cells. Its expression has been considered as an important process by which tumor cells suppress antitumor immunity in the tumor microenvironment (7,8). There have been several conflicting reports describing an association of PD-L1 expression with cancer prognosis (9 –11). In tumors, PD-L1 upregulation occurs either by constitutive oncogenic signaling via AKT or STAT3, a mechanism termed intrinsic immune resistance, or by IFN-gamma produced by activated T cell or NK cells (adaptive resistance). Thus, its overexpression is generally thought to be a risk factor for poor prognosis. However, the clinical significance of PD-L1 expression in disease-related recurrence in PTC has not been established. Therefore, the present study evaluated the prevalence and prognostic significance of PD-L1 expression in a collection of PTCs, testing the effectiveness of it as a novel prognostic molecular marker that has now started entering clinic for the management of cancer.
Materials and Methods
Patients selection and immunohistochemistry
Two hundred and sixty patients with PTC who underwent thyroidectomy between 2003 and 2012 at the Department of Head and Neck Surgery, Fudan University Shanghai Cancer Center (FUSCC) were identified eligible for the study. The patients included in the study met the following criteria: no previous thyroid surgery, the availability of an adequate medical history, and the histopathologic diagnosis of PTC. Patients with follicular thyroid cancer (FTC) and other histological types (anaplastic, medullary, lymphoma, sarcoma, metastatic carcinoma, and others) were systematically excluded. All tissues samples of the 260 eligible patients were provided by the Tissue Bank of FUSCC and used for tissue microarray construction. The corresponding non-tumor thyroid tissues were obtained at least 1 cm away from the tumor. All tissue samples were formalin-fixed and paraffin-embedded. All relevant histological slides were reexamined and reclassified according to current World Health Organization criteria by pathologists who had no knowledge of disease outcome. TNM staging was classified based on the criteria of the American Joint Committee on Cancer (AJCC, 7th edition) for differentiated thyroid cancer by pathologists who had no knowledge of the disease outcome (12). The study was approved by the Human Ethics Committee/Institutional Review Board of Fudan University Shanghai Cancer Center. Written informed consent was obtained from all 260 patients. Details of 260 primary surgery patients were obtained from the database of the Department of Medical Informatics.
Immunohistochemistry (IHC) staining was performed by using a highly sensitive streptavidin-biotin-peroxidase detection system with TC tissue microarrays and a rabbit monoclonal anti-PD-L1 (ab174838; working dilution 1:50) purchased from Abcam (Cambridge, MA) and a mouse monoclonal anti-PD-L1 (MABC290; working dilution 1:200) purchased from Millipore (Darmstadt, Germany). Immunolabeling was conducted using Dako EnVision + Rabbit Polymer (cat. no. K4003) from Dako (Carpinteria, CA). The slides were counterstained with hematoxylin and coverslipped.
IHC scoring
The IHC-stained tissue sections were scored separately by two pathologists blinded to the clinical parameters. In cases of disagreement, the result was reached by consensus. The staining intensity was scored as 0 (none), 1 (weak), 2 (medium), or 3 (strong). The extent of the staining was scored as (0, <5%; 1, 5–25%; 2, 26–50%; 3, 51–75%; and 4, >75%) according to the percentages of the positive staining areas in relation to the whole carcinoma area. Scores for staining intensity and percentage positivity of cells were then multiplied to generate the immunoreactivity score (IS) for each case. Tissues having a final staining score of <4, 4, 6, or ≥8 were considered to be negative (–), weak (+), medium (++), or strong (+++) staining, respectively (Fig. 1). Specimens with negative and weak staining were assigned to PD-L1-negative group, and those with medium and strong staining were assigned to PD-L1-positive group.
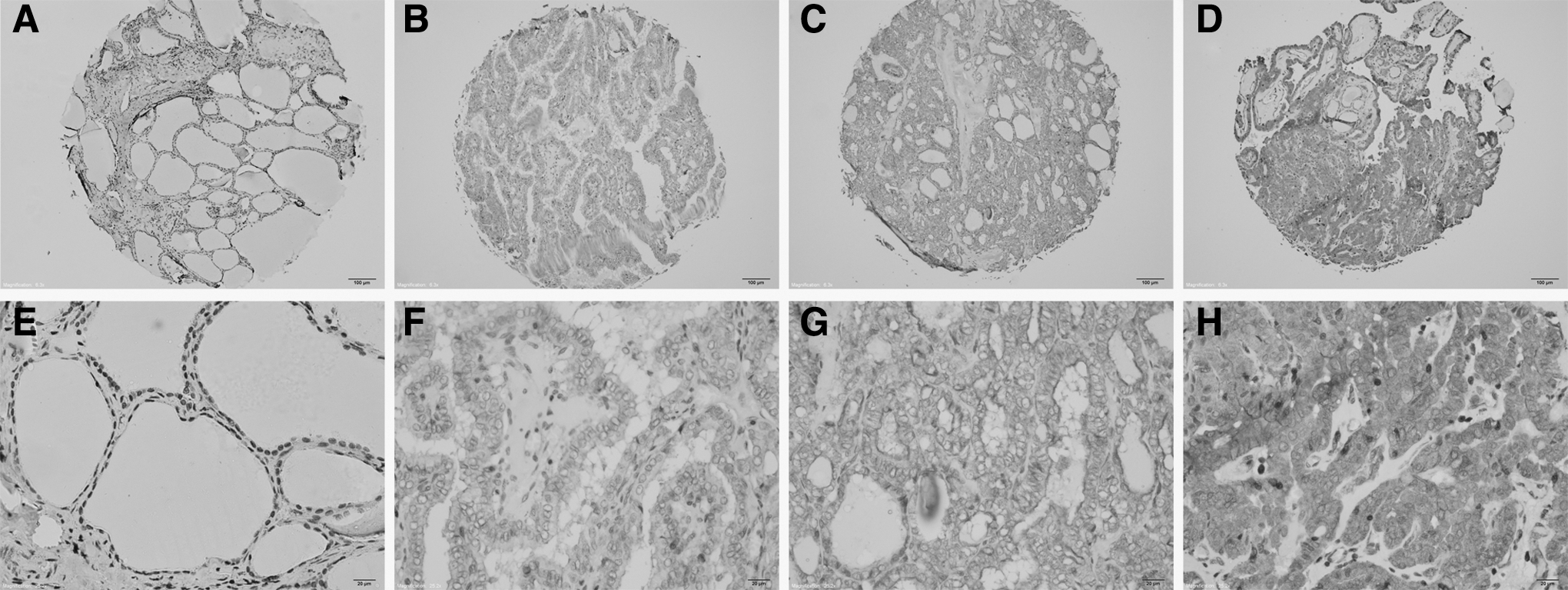
Expression of programmed death-ligand 1 (PD-L1) in papillary thyroid cancer tissues by immunohistochemistry (IHC). To analyze the correlation between the expression of PD-L1 and survival outcomes, negative and weak expression were grouped as PD-L1 negative, and medium and strong expression were grouped as PD-L1 positive. (
Initial treatment
Before surgery, each patient underwent an ultrasonography (US) examination. US-guided fine-needle aspiration was not performed routinely. Lobectomy plus ipsilateral central lymph node dissection (CLND) was typically performed as the initial surgical treatment for PTC patients with malignant lesions that were limited to a single lobe (13). When the patient was aged >45 years, the primary tumor was >1 cm, undetermined nodules were detected in the contralateral lobe by US, or regional metastases or multifocal tumors were present, total thyroidectomy (TT) was performed at the time of the initial operation. Undetermined nodules refer to contralateral thyroid nodules, which were suspicious only by imaging examinations but lacked cytological characterization preoperatively. When undetermined nodules were detected without other factors, a subtotal lobectomy of approximately one-fourth to two thirds of the contralateral lobe was performed to remove the suspicious lesions. Intraoperative frozen section (FS) histology assisted surgeons in determining the extent of the surgical procedures. When malignant lesions were identified in both lobes of the thyroid by FS after a subtotal lobectomy, a completion thyroidectomy (CT) was performed (13). Modified lateral lymph node dissection, including levels II–V, was performed in cases with pathologically proven lymph node metastasis (LNM) or suspicious lymph nodes observed intraoperatively or on preoperative imaging.
Suppressive treatment with thyroid hormone was initiated after surgery to decrease serum thyrotropin (TSH) to subnormal levels without clinical thyrotoxicosis. Because its use is strictly controlled in China, radioactive iodine (RAI) therapy was not routinely prescribed for PTC patients after surgery unless patients had distant metastases (13).
Clinicopathologic variables assessed
Clinicopathologic variables, such as sex, age at diagnosis, maximal tumor size, multifocal lesions (defined as two or more cancer sites within the thyroid; multifocal lesions could be either unilateral or bilateral (14)), extrathyroidal extension (ETE), coexistent Hashimoto's thyroiditis (HT), central lymph node metastasis (CLNM), and lateral lymph node metastasis (LLNM), were collected for analysis. According to the current staging system, the age of 45 years was used as the cutoff point to divide all patients into younger patients (age <45 years) and older patients (age >45 years), and the cutoff points of 2 and 4 cm were used to stratify subgroups (15). The prognosis of cancer was analyzed as a binary variable to indicate whether any local recurrence or distant metastasis had occurred. The tumor characteristics were assessed by the final pathologic findings.
Follow-up
All patients received TSH-suppressive hormonal therapy following surgery. RAI therapy was limited to patients who had distant metastasis because of its strictly controlled use in China. All 260 patients gave their consent to participate in the follow-up analysis and are the subjects of this study. The follow-up period for each patient was defined as the length of time from the initial therapy until the last known contact either as documented by medical record review or by telephone calls. Recurrence was defined as the appearance of disease, with new biopsy-proven/secondary surgery–confirmed local disease or distant disease revealed by US and/or imaging scans, in any patient who had been free of disease (no palpable disease and negative RAI scan). It was classified as “local” if the contralateral lobe or cervical lymph nodes were involved and as “distant” if the disease was located in other sites, including the lung, bone, brain, or other sites. Local/distant recurrence-free survival (RFS) was defined as the time between the date of initial surgery and the first event of recurrence or death.
Statistical analysis
The results are expressed as the mean ± standard deviation. Statistical analysis was performed using Student's t-test, chi-square test, or Mann–Whitney test as appropriate. Patients who were alive and who did not relapse were censored at the date of their last follow-up visit. Survival rates were estimated using the Kaplan–Meier method (16). The hazard ratio (HR) and the confidence interval (CI) for relationships between each variable and recurrence were calculated using a binary Cox regression model (17). A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics for Windows v13.0 (SPSS, Inc., Chicago, IL).
Results
Characteristics of patients
In age of the 260 PTC patients enrolled in the present study age ranged from 14 to 80 years (M = 46.6 ± 12.3). As initial surgical treatment for primary tumor, TT was performed in 57 (21.9%) while CLND was typically performed for each PTC patient. RAI therapy was applied only in patients with local or distant recurrence after TT in 25 (9.6%) patients. According to the final pathology, 140 (53.8%) patients had LNM involving only the central compartment (N1a), and 86 (33.1%) had involvement of both the central and lateral compartments (N1b). Skip metastases, which indicate LLNM without CLNM (18), were found in three (1.5%) patients. There were no patients with a history of head and neck radiation before surgery, and no patient had distant metastasis at diagnosis. The characteristics of these patients are listed in Table 1.
Data are presented as n (%).
PD-L1, programmed death-ligand 1.
Correlation between PD-L1 expression in cancer tissues and clinicopathologic features
The protein levels of PD-L1 expression in samples were analyzed by IHC staining. PD-L1 expression was positive in 136/260 (52.3%) papillary cancer samples and negative in the remaining 124 (47.7%) samples. Among them, 122 (46.9%) samples were ++, and 14 (5.4%) were +++. The corresponding non-tumor thyroid tissues were also stained. The PD-L1 expression in tumor and non-tumor tissues is summarized in Table 1. Non-tumor tissues were scored as – in 164 (63.1%) cases and + in 96 (36.9%) cases. Overall, the expression levels of PD-L1 were significantly lower in non-tumor tissues compared with corresponding thyroid tumor tissues (p = 0.001). All IHC samples were stained and evaluated with two different antibodies, and the results were similar, as shown in Supplementary Figures S1 and S2 (Supplementary Data are available online at
Correlation between PD-L1 expression in cancer tissues and patient survival
The mean follow-up duration was 121 months (range 13–161 months). During this time, only one (0.5%) patient died from a cancer specific cause. Neck recurrences occurred in 29 (12.3%) patients, and distant recurrences occurred in three (1.5%) patients. The Kaplan–Meier method and log-rank test were adopted to analyze time-dependent influences of clinicopathologic variables and PD-L1 expression (Fig. 2A and B) in tumor tissues on recurrences. The results show that primary tumor size >4 cm (HR = 6.604 [CI 2.826–15.435], p = 0.001), multifocality (HR = 3.098 [CI 1.484–6.468], p = 0.003), ETE (HR = 3.155 [CI 1.559–6.383], p = 0.001), CLNM (HR = 2.203 [CI 1.985–4.925], p = 0.050), LLNM (HR = 1.880 [CI 1.130–3.804], p = 0.049), and PD-L1-positive staining (HR = 3.306 [CI 1.424–7.673], p = 0.005) were independent predictors for recurrence, while other variables such as sex, age, and HT were not significantly associated with recurrence (Table 2).
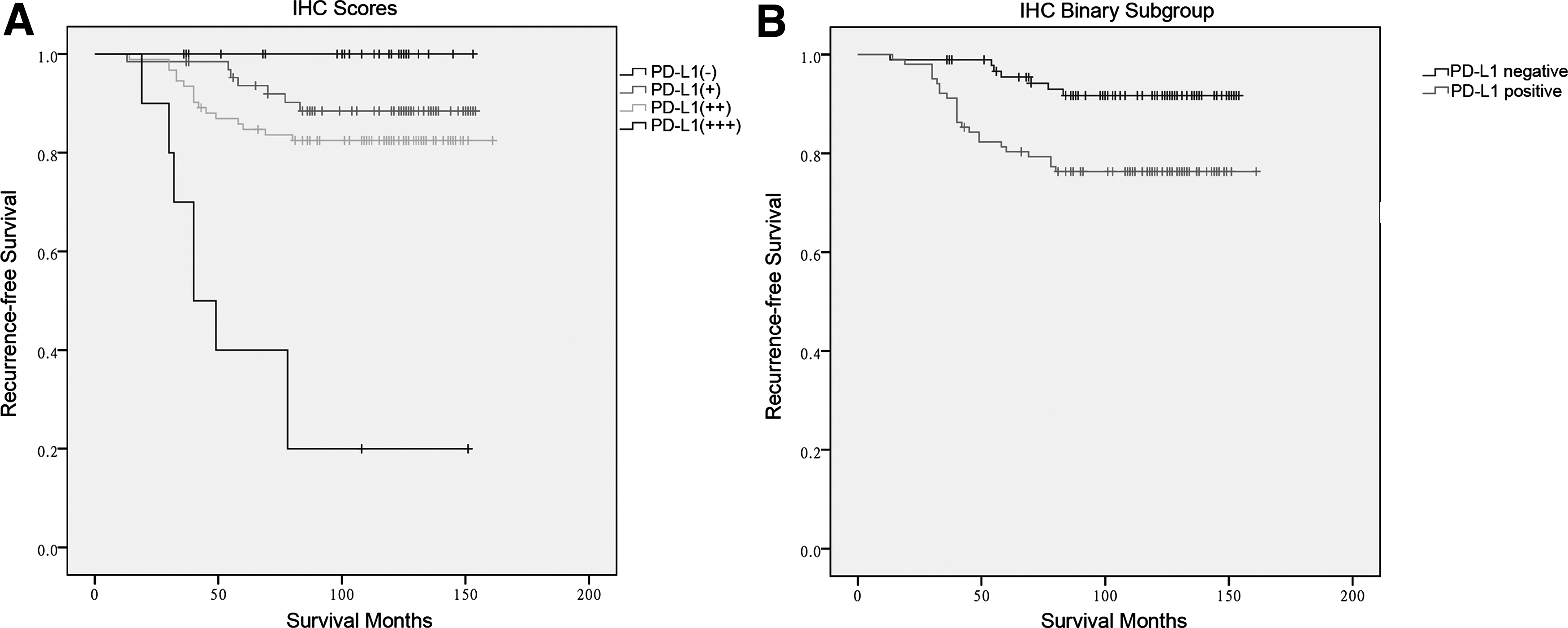
Kaplan–Meier survival curves according to the expression of PD-L1 in papillary thyroid cancer tissues by IHC. (
HR, hazard ratio; CI, confidence interval.
To determine how strongly PD-L1 expression in cancer tissues is associated with recurrence relative to other known predictors of recurrence in PTC, multivariate Cox regression analysis was performed. Instead of limiting the multivariate analysis to the significant terms from the univariate analysis, all variables were included because these factors have been previously demonstrated to be important in predicting disease recurrence in adult PTC patients. The results are presented in Table 2. The risk of recurrence increased significantly with higher PD-L1 expression (HR = 2.825 [CI 1.149–6.943], p = 0.024). In addition, primary tumor size >4 cm (HR = 4.933 [CI 1.784–13.638], p = 0.002) was another independent predictor of recurrence in multivariate analysis after adjusting to other factors.
Impact of PD-L1 expression in cancer tissues on survival in subgroups
The traditional adverse clinicopathologic features and risk factors identified from the Cox proportional hazards regression models were all reported to be associated with poor prognosis in previous studies in PTC patients. Further subgroup analyses were conducted for the effects of PD-L1 expression in tumor tissues on survival in patients stratified by clinicopathologic variables assessed in this study (Figures 3 and 4). Using the Kaplan–Meier method and log-rank test, it was found that PD-L1 positive staining was associated with worse RFS than negative staining was in males (p = 0.001), older patients (≥45 years, p = 0.001), and subgroups of patients with a primary tumor size >4 cm (p = 0.002), multifocal tumors (p = 0.031), ETE (p = 0.012), and LNM (p = 0.004). In contrast, PD-L1-positive staining predicted worse RFS than negative staining did in the subgroup of patients without HT (p = 0.001) compared with the ones with HT (p = 0.196). Furthermore, in the patients with TT as the initial treatment for primary tumor (referring to the indications mentioned above), PD-L1-positive staining was also associated with worse RFS (p = 0.019), but the association was not significant in the patients treated with lobectomy or lobectomy and partial contralateral lobectomy (p = 0.127).
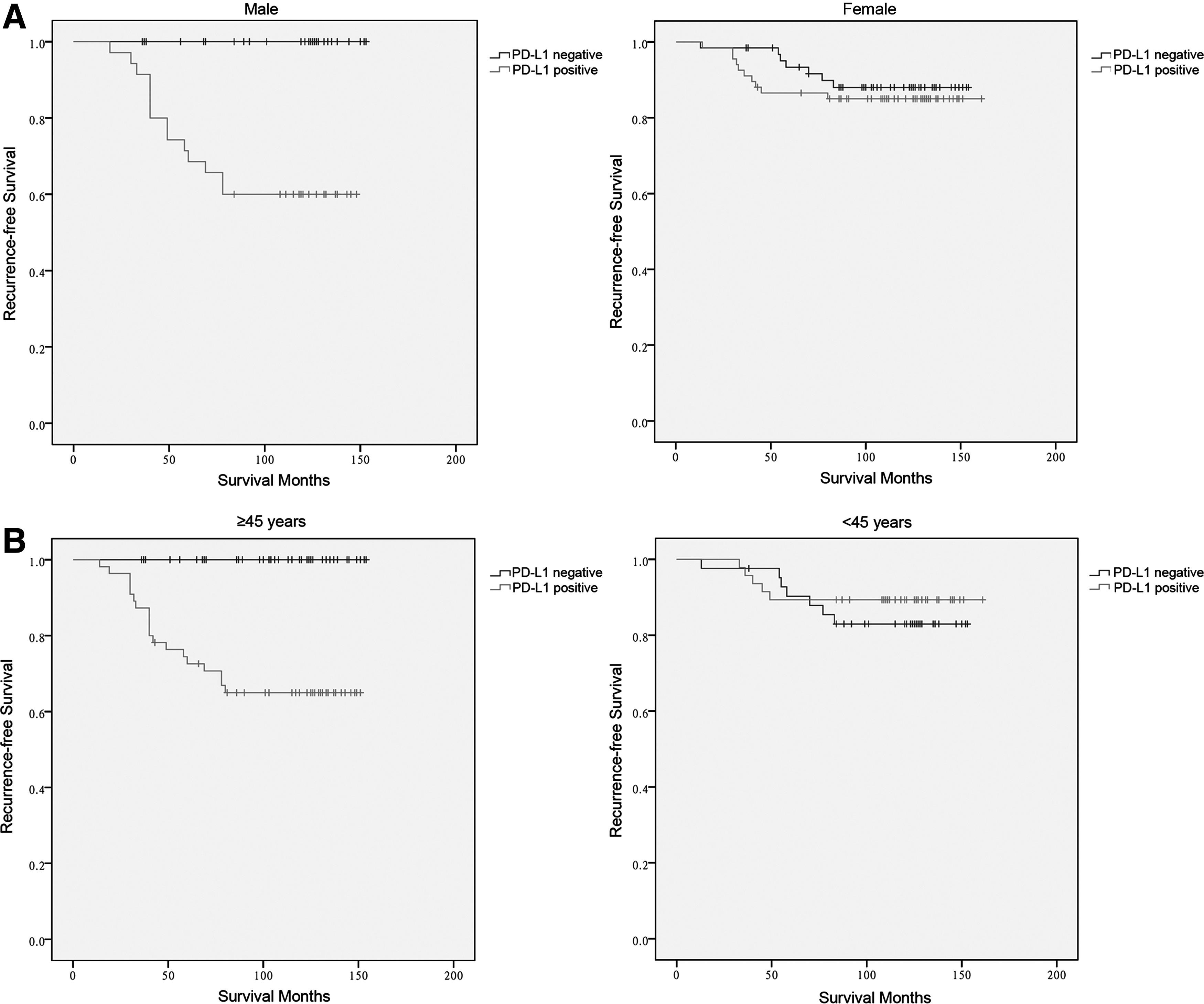
Kaplan–Meier survival curves according to the expression of PD-L1 in papillary thyroid cancer tissues by IHC. (
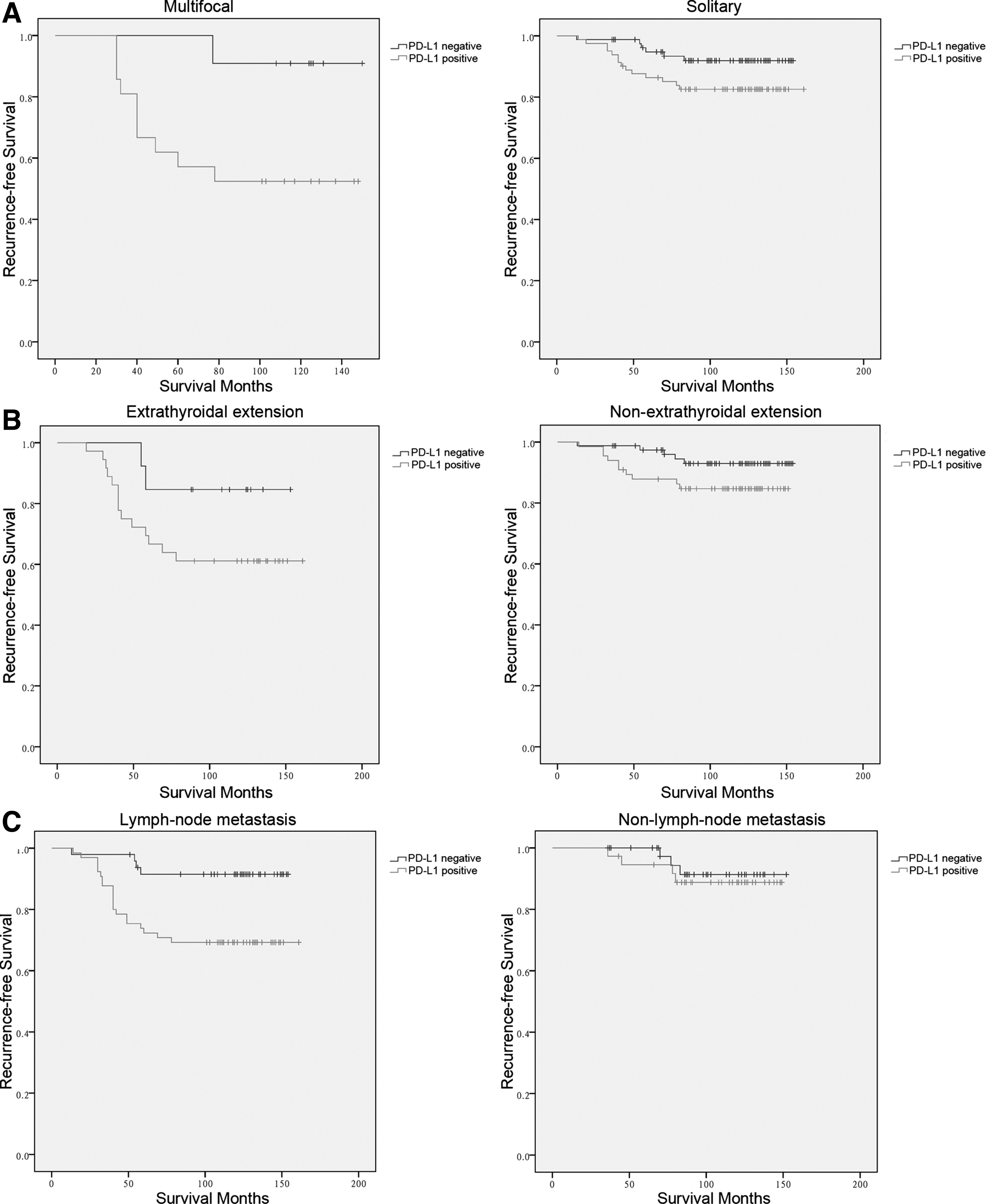
Kaplan–Meier survival curves according to the expression of PD-L1 in papillary thyroid cancer tissues by IHC. (
Discussion
The present study demonstrates the prognostic value of PD-L1 expression on RFS in patients with PTC. Consistent with the findings in a recently published study by Chowdhury et al. (19), this study found a negative influence of PD-L1 expression in PTC cells on recurrence and independently confirms that PD-L1 overexpression is a negative prognostic marker for PTC. The effect of PD-L1-positive staining in tumor tissues on recurrence remains significant even after multivariable adjusting for the clinicopathologic risk factors. Compared with negative samples, the PTC-related RFS for patients with positive PD-L1 expression in tumor tissue was also significantly lower in the following subgroups: male sex, older age, larger tumor size (>4 cm), multifocal tumors, ETE (p = 0.012), and LNM. This demonstrates an incremental adverse effect of the positive expression of PD-L1.
In previous studies, it was reported that the positive rates of the expression for PD-L1 in human tumor tissues ranged from 25.0% to 85.0% by IHC (20 –25). In this translational study, a higher PD-L1 expression was observed in PTC tumor tissues compared with non-tumor tissues, which is consistent with previous studies (26,27). Second, a incidence of 52.0% of cytoplasmic staining was detected in addition to the membranous PD-L1 expression (++/+++) in follicular tumor cells (28). Although the positive rates in various studies are partially influenced by different scoring systems and differences in the antibodies for PD-L1 detection, the present findings are generally in line with previous studies, as well as the experimental models for a series of malignant tumors, suggesting a prominent involvement of the PD-L1 axis in creating an immunosuppressive microenvironment in PTC. On the other hand, the high prevalence of PD-L1 expression also provides a strong rationale for clinical trials investigating immune checkpoint inhibitors and the response to treatment in advanced or refractory PTC.
As known, PD-L1 constitutes an important element of the immune response. However, its prognostic value is still not defined. In the present study, it was hypothesized that PD-L1 could classify patients into different risk groups because of the correlation between PD-L1 expression and some of the prognostic factors. Indeed, PD-L1 was independently correlated with multifocality and ETE of tumor, which were considered as traditional risk factors for prognosis in previous studies (29,30). Relevant in the tumor microenvironment, PD-L1 expressed on the surface of follicular-derived papillary cancer cells attracts PD-1 expressing immune-inhibitory tumor-infiltrating lymphocytes in the PD-1 pathway within the thyroid gland, thereby inducing a intratumoral immune reaction, which is thought to have a favorable influence on tumor development (31). However, the complex interaction of immune effector T cells such as CD4+ T cells, CD8+ T cells, and Treg cells within the tumor microenvironment very distinctly impacts the biological features. Thus, this immune reaction network between lymphocytes and clinicopathologic features needs to be further characterized in future studies.
Interestingly, it was found that the negative impact of PD-L1 was weakened in the HT group in subgroup analysis. Chronic lymphocytic thyroiditis, such as coexistent HT, is characterized by infiltration of the thyroid gland by inflammatory cells producing chemokines, cytokines, and growth factors, thereby creating a functional network between thyroid epithelial cells and inflammatory cells (32). This suggests that autoimmune activity against the gland may also exert a protective effect on the recurrence in PTC, even if PD-L1 is expressed in tumor tissues. However, the favorable clinical outcome with coexistent HT was not significant in the studied PTC patients, which may be explained by the low incidence of coexistent HT (20.9%) compared with other studies (33 –35).
TT is the most commonly performed operation in previous studies, and those who favor TT believe that PTC is often multifocal and that the recurrence of locoregional disease would occur less frequently with more extensive surgery (36 –38). However, this study found that the TT group did not have a lower incidence of recurrence in patients with more advanced tumor stage in multivariate analysis. The higher rate of PD-L1 expression in patients with TT, compared with patients without TT (66.7% vs. 48.1%), may explain why extended surgery did not improve the prognosis of PTC patients. In order to control locoregional disease better in patients who underwent TT, RAI therapy may be particularly indicated in patients who have a high expression of PD-L1 in tumor tissues.
The present analysis, though comprehensive and performed at a single center that is highly specialized in the diagnosis and treatment for TC, has limitations. Both the retrospective nature of the analysis and the limited comprehensive endocrine evaluations in many patients represent challenges in accurately analyzing the correlations between PD-L1 expression and patient outcomes. Second, the sample size of the study is small.
Considering the association of PD-L1 expression and poor pathologic features and clinical outcomes, PD-L1 expression emerges as a potential prognostic biomarker in PTC. The high expression of PD-L1 defines it as a viable therapeutic target to optimize clinical outcomes in patients with advanced PTC. Whether the high expression of PD-L1 in PTC is likely to respond to anti-PD-L1 therapies should be investigated in further studies.
Footnotes
Acknowledgments
We would like to acknowledge our collaborators Dr. Wan-run Lin, Dr. Lei Dong, and Dr. Yue Zhang from the Department of Pathology at the Fudan University Shanghai Cancer Center for the immunohistochemistry scoring. We would like to acknowledge Prof. Meng-hong Sun and Prof. Xiao-qiu Li from the Tissue Bank at the Fudan University Shanghai Cancer Center for help with obtaining PTC tissues. We would like to acknowledge Dr. Fei Liang and Prof. Ji Zhu for administration support and for excellent technical assistance.
This work was supported by funds from the National Natural Science Foundation of China (No. 81572622 and No. 81272934 to QHJ) and Shanghai Municipal Health Bureau Project (No. 20134406).
Author Disclosure Statement
The authors have declared that no competing interests exist.