
Abstract
Background:
Hürthle cell carcinoma (HCC) is not typically iodine avid, raising questions regarding postoperative use of radioactive iodine (RAI). The aims of this study were to describe current practice patterns regarding the use of RAI for HCC and to assess its association with survival.
Methods:
The National Cancer Data Base 1998–2006 was queried for all patients with HCC who underwent total thyroidectomy. Inclusion was limited to T1 tumors with N1/M1 disease, and T2–4 tumors with any N/M disease. Patients were divided into two treatment groups based on receipt of RAI. Baseline patient characteristics were compared between the two groups. Survival was examined using Kaplan–Meier and Cox regression analyses.
Results:
A total of 1909 patients were included. Of these, 1162 (60.9%) received RAI, and 747 (39.1%) did not. Patients treated with RAI were younger (57 vs. 61 years for no RAI, p < 0.001), more often had private insurance (61.7% vs. 53.5% for no RAI, p < 0.003), and were more likely to be treated at an academic center (40.0% vs. 33.1% for no RAI, p < 0.001). Five- and 10-year survival rates were improved for patients who received RAI compared with those who did not (88.9 vs. 83.1% and 74.4 vs. 65.0%, respectively, p < 0.001). RAI administration was associated with a 30% reduction in mortality (hazard ratio = 0.703, p = 0.001).
Conclusion:
Present guidelines are inconsistent with regard to indications for using RAI for HCC. This could explain why nearly 40% of HCC patients did not receive RAI. RAI is associated with improved survival, suggesting that it should be advocated for HCC patients with tumors >2 cm and those with nodal and distant metastatic disease.
Introduction
H
National guidelines for the management of HCC are rooted in the treatment algorithms for follicular thyroid cancer, but these recommendations differ between the American Thyroid Association (ATA) and the National Comprehensive Cancer Network (NCCN) (3,5). Specifically, the recommended adjuvant role of radioactive iodine (RAI) for HCC is not standardized, likely as a result of the demonstrated decreased avidity that HCC generally has for iodine (6). The ATA recommends RAI postoperatively for HCCs following total thyroidectomy, although smaller tumors <1 cm and minimally invasive HCCs rarely require this intervention, as surgery may be sufficient (3). In contrast, the NCCN selectively recommends RAI for tumors >2 cm or in the presence of vascular invasion, extrathyroidal extension, lymph node metastases, or elevated postoperative unstimulated thyroglobulin (Tg) levels (5).
The aims of this study were to identify patterns of RAI use for HCC in a nationally representative sample, and to assess for any association between RAI utilization and overall survival among patients with HCC.
Methods
The National Cancer Data Base (NCDB) is a joint program of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. It is a nationwide, facility-based, comprehensive clinical surveillance data set that currently captures 70% of all newly diagnosed malignancies in the United States. It was established in 1989, and currently contains more than 29 million cancer cases from more than 1500 Commission on Cancer-accredited cancer programs from all 50 states, Puerto Rico, and the District of Columbia. More than 85% of all new thyroid cancer cases in the United States are captured in the database.
Data were coded according to the Commission on Cancer Registry Operations and Data Standards Manual, the American Joint Committee for Cancer (AJCC) Manual for Staging of Cancer, and the International Classification of Disease for Oncology (7). The NCDB stages subjects according to the AJCC. To reduce data errors and maintain the integrity of the database, all data were extracted from medical records by trained and certified tumor registrars. Data were validated both locally and at the NCDB level. Data were de-identified and submitted to the NCDB in compliance with the Health Insurance Portability and Accountability Act. The Institutional Review Board granted this study an exemption status.
Subjects
The NCDB was queried for all adult (age ≥18 years) patients with a diagnosis of HCC who underwent total thyroidectomy between 1998 and 2006. The International Classification of Disease for Oncology, Third Edition code 8290/3 was used to identify patients with HCC (8). NCDB procedure codes 40 and 50 were used to identify patients who underwent near-total or total thyroidectomy. Inclusion criteria were based on the TNM Classification of Malignant Tumors staging system; patients included in the data analysis had HCC tumors deemed to be T1 with N1 or M1 disease, and T2–4 tumors with any N or M disease (7). Patients were divided into two treatment groups based on whether they received RAI.
Demographic variables, including patient age at diagnosis, sex, race/ethnicity, annual income, insurance status, type of insurance, year of diagnosis, distance traveled to the treating institution, and comorbidity were extracted from the database. Patient co-morbidities were represented by the modified Charlson/Deyo scoring system (9). Annual income levels were assigned by the NCDB by linking a patient's zip code to the 2000 U.S. Census data. Clinical and pathologic variables of interest included tumor size, postoperative surgical margin status, lymph node involvement, and cancer stage according to the AJCC. Facility characteristics included treatment facility type and treatment facility volume. Facilities were characterized as academic, community, or comprehensive. High-volume treatment facility status was considered to be >10 cases per facility during the time period, as this represented at least one case of HCC per year and the 90th percentile per facility.
Analysis
Baseline characteristics were reported using frequencies and proportions for categorical variables. Data were compared utilizing the chi-square test, Student's t-test, and the log-rank test. Overall survival was defined from the time of diagnosis to the time of death or last follow-up, whichever came first. Survival time was censored for patients alive at the end of the study period. Patients with zero months of follow-up were excluded. Estimates and confidence intervals (CIs) of overall survival proportions were computed using the Kaplan–Meier method, and survival distributions were compared across groups using the log-rank test.
A multivariable Cox proportional hazards model was used to examine the adjusted association of receipt of RAI and survival. The model adjusted for the effects of patient demographics, tumor factors, and facility characteristics, including age, sex, tumor size, surgical margin status, lymph node status, facility type, and surgical volume of the institution.
All analyses were conducted using SPSS (version 22, Armonk, NY: IBM Corp) statistical software. Two-sided statistical tests were specified in all analyses, and p-values of <0.05 were considered statistically significant.
Results
A total of 1909 patients underwent total thyroidectomy for HCC >2 cm and T1 tumors with N1 or M1 disease between 1998 and 2006. In all, 1162 (60.9%) patients received RAI, and 747 (39.1%) did not (Table 1). On univariate analysis, patients treated with RAI were younger (M age = 57 years vs. 61 years for no RAI, p < 0.001), more often had private insurance (61.7% vs. 53.5% for no RAI, p < 0.003), and were more likely to be treated at an academic center (40.0% vs. 33.1% for no RAI, p < 0.001). RAI utilization for HCC varied significantly across tumor stages (patients with Stage I disease were more likely to receive RAI than other patients were), but it did not differ significantly based on such pathologic features as tumor size, margin status, or lymph node involvement (Table 2).
NCDB, National Cancer Data Base; RAI, radioactive iodine.
HCC, Hürthle cell carcinoma; LN, lymph node; NOS, not otherwise specified; T, tumor; M, metastasis.
Five- and 10-year overall survival rates were improved for patients who received RAI versus those who did not receive RAI (88.9 vs. 83.1% and 74.4 vs. 65.0%, respectively, p < 0.001; Fig. 1). There was no difference in unadjusted overall survival in patients <45 years who were treated with RAI compared to those who did not receive RAI. However, there were only 13 deaths in this cohort of patients. On multivariate analysis, there was no difference in RAI utilization between high- and low-thyroidectomy volume facilities (hazard ratio [HR] = 0.817, p = 0.227), or between community and academic facilities (HR = 1.11, p = 0.577; Fig. 2). RAI administration was independently associated with a 30% reduction in mortality (HR = 0.703, p = 0.001).
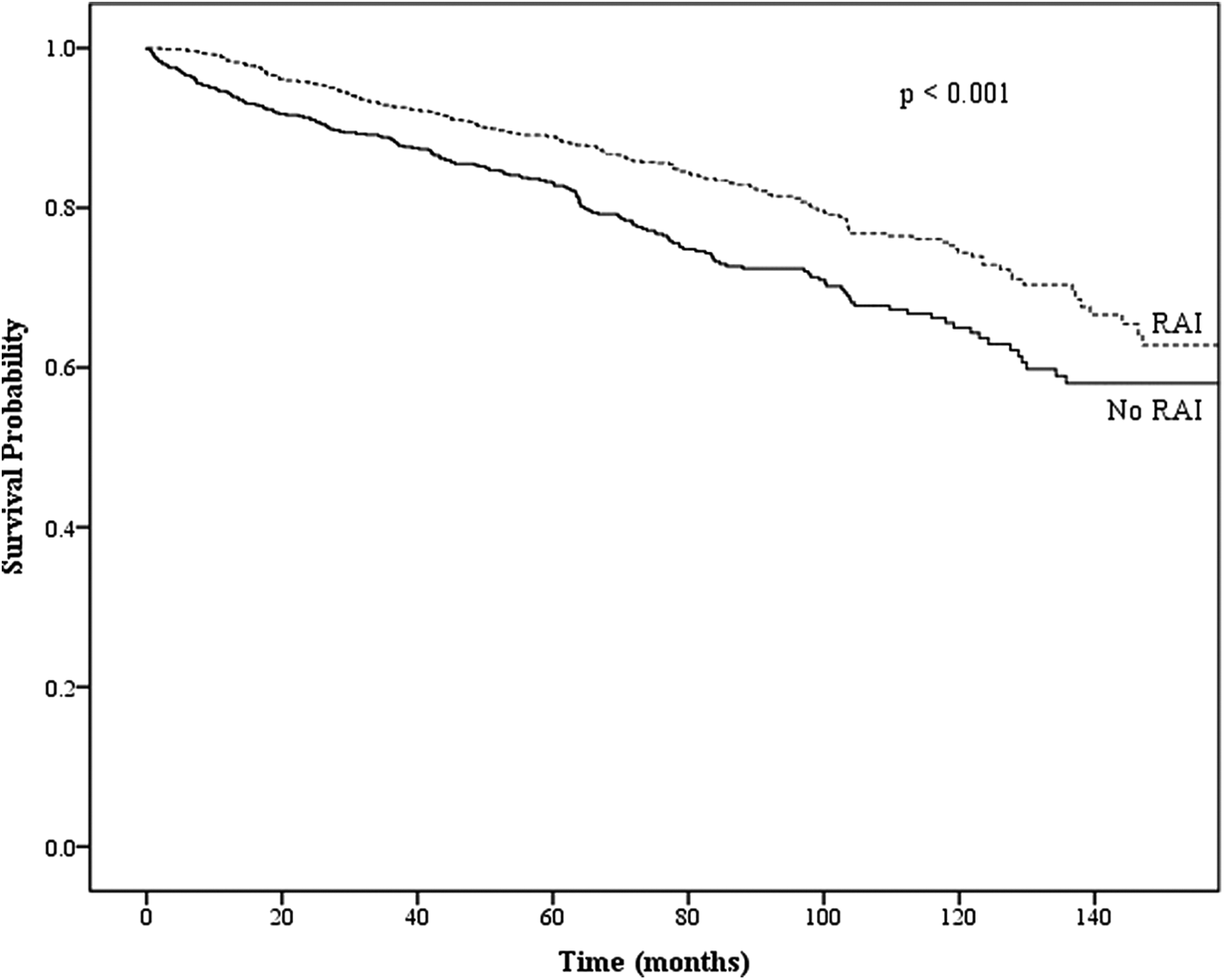
Overall survival according to radioactive iodine use in patients with Hürthle cell carcinoma in the National Cancer Data Base, 1998–2006.
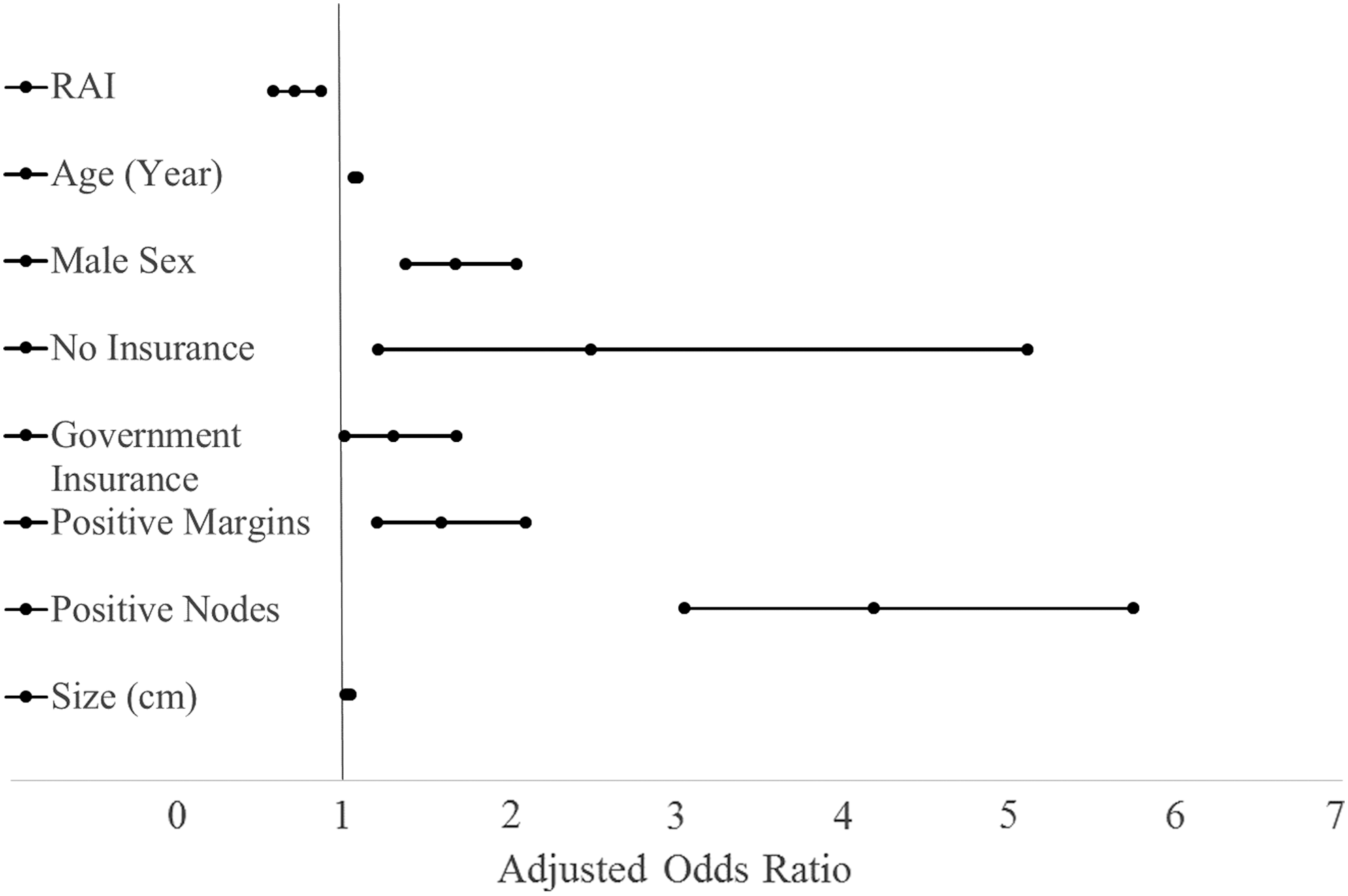
Factors independently associated with overall survival for patients with Hürthle cell carcinoma in the National Cancer Data Base, 1998–2006.
In a subset analysis of patients analyzed based on a tumor size of 2–4 cm and >4 cm, patients with tumors that were 2–4 cm who received RAI were younger (M age = 54 vs. 59 years, p < 0.001) and more often had private insurance (65.8% vs. 54.3% for no RAI, p = 0.001) or underwent treatment at an academic medical center (37.5% vs. 31.1% for no RAI, p = 0.003). Patients with tumors 2–4 cm who received RAI more often had positive surgical margins (5.6% vs. 3.2% for no RAI, p = 0.031) and positive lymph node involvement (12.7% vs. 11.1% for no RAI, p = 0.035). In this subgroup, 5- and 10-year overall survival rates were improved for patients who received RAI compared with those who did not receive RAI (97.8 vs. 87.8% and 94.1 vs. 71.9%, respectively, p < 0.001).
Patients with tumors >4 cm who received RAI were younger (M age = 60 vs. 64 years, p = 0.006) and were more likely to be treated at an academic center (43.3% vs. 35.4% for no RAI, p = 0.008). On univariate analysis, RAI utilization for HCC tumors >4 cm did not differ significantly according to pathologic features such as tumor size or stage, margin status, or lymph node involvement. In this subgroup, 5- and 10-year overall survival rates also were improved for patients who received RAI compared with those who did not receive RAI (82.3 vs. 77.6% and 62.3 vs. 56.9%, respectively, p < 0.001).
Discussion
Recommendations regarding the use of adjunctive therapy with RAI for HCC differ across ATA and NCCN guidelines. This may account for the nearly 40% of HCC patients in this study who did not receive RAI. Although the utility of RAI has been debated, an association has been shown here between RAI use and improved survival, suggesting that its use should be advocated for in HCC patients with tumors >2 cm and those with nodal and/or distant metastatic disease.
The ATA recommends RAI postoperatively for HCC tumors >1 cm following total thyroidectomy (3), and the NCCN selectively recommends RAI for tumors >2 cm or in the presence of vascular invasion, extrathyroidal extension, lymph node metastases, or elevated postoperative unstimulated Tg levels (5). Although RAI therapy has been shown to be beneficial in the treatment of papillary and follicular thyroid carcinoma, its utility in HCC has been challenged because RAI does not accumulate as well in HCC (10). The relative rarity of HCC and its exclusion from most large trials evaluating the efficacy of RAI for well-differentiated thyroid cancer have limited studies to mostly small, retrospective, single institutional series evaluating RAI uptake for patients with metastatic HCC.
Reports of RAI uptake in metastatic HCC have ranged substantially across multiple studies. In a study by Kushchayeva et al. of 33 patients with HCC, 11 patients developed recurrence and underwent a RAI scan (10). Only 1/11 (9%) patients had appreciable uptake at the site of metastases. In another study by Besic et al. including 48 patients with HCC, eight patients were diagnosed with metastases at initial presentation, and eight patients developed recurrent distant metastases (6). RAI uptake was identified in 11/16 (69%) patients, who were subsequently treated. The authors suggested that the high rate of RAI uptake seen in their study may be due to more frequent (87.5%) adjuvant iodine remnant ablation after thyroidectomy compared with historical studies; the iodine may be preferentially taken up by the thyroid remnant rather than residual disease.
The impact of RAI on survival for HCC has been evaluated by few studies. In a study by Lopez-Penabad et al., 72% of the 89 patients with HCC received adjuvant RAI (11). Of the 37 patients with known metastases at the time of initial RAI scan, 14 (38%) patients showed uptake. RAI treatment had no observed effect on overall mortality in this small study. On subgroup analysis, however, they reported a significant improvement in overall survival for HCC patients who received RAI for adjuvant ablation compared with those who either did not receive RAI treatment or received treatment in the presence of residual disease. Another SEER-based study by Goffredo et al. including 3311 patients with HCC demonstrated improved disease-specific survival in univariate analysis of their HCC cohort. However, this was not shown on multivariate analysis, likely a result of the findings being underpowered (4).
To the authors' knowledge, this is the first study to demonstrate a survival advantage in patients with HCC who received RAI. Both 5- and 10-year overall survival rates were significantly improved for patients with T1 and N1 or M1 disease, or T2–4 disease, who received RAI. Given the rarity of HCC and the small cohort sizes of previous studies, it is possible that this association could only be demonstrated in this adequately powered patient cohort.
Significant variation was found in patterns of RAI utilization for HCC, including treatment that was not aligned with professional society and cooperative group guidelines for HCC. Patients were more likely to receive RAI therapy if they were younger, had private insurance, and/or were treated at an academic institution. Subgroup analysis did not account for observed variation based on differences in tumor size, lymph node, or surgical margin status.
According to the ATA and NCCN guidelines, RAI therapy was indicated for all the patients included in this study, based on the inclusion criteria. It is therefore surprising that only 61% of patients received RAI treatment. This low rate of adherence to guidelines is similar to that reported by Famakinwa et al., who examined practice patterns among 52,964 patients with differentiated thyroid carcinoma using the Surveillance, Epidemiology, and End Results (SEER) data set. Of 491 patients with HCC included in the study, only 51% deemed to be eligible for RAI remnant ablation received treatment (12). In another SEER population-level analysis of 3311 HCC patients, Goffredo et al. evaluated disease-specific survival and benchmarked practice patterns with ATA guidelines. They found that only 54.1% of patients underwent RAI therapy in accordance with the guidelines (4). Their multivariate analysis demonstrated one notable factor independently associated with HCC management that was not adherent with guidelines was patient age >65 years. The present data from the NCDB reinforces the fact that RAI administration for HCC is often not in accordance with recommendations from national practice guidelines, and is adequately powered to show a significantly positive association with RAI and patient survival.
The current study has several limitations, including those inherent to using a large administrative database. The NCDB has been well validated with minimal coding errors overall (13). Both disease recurrence and disease-specific survival are not captured as outcomes in this database and therefore are absent from the analysis. To use criteria from both the ATA and NCCN guidelines, an overlap in extent of surgery and tumor characteristics was necessary; this resulted in the inclusion criteria of tumor size cutoff of 2 cm and T1 lesions with nodal or metastatic disease. To capture the effect of RAI on HCC best, the study was limited to those patients who had total thyroidectomy (14). Despite these limitations, this study is strengthened by its large sample size.
In conclusion, treatment recommendations differ between guidelines issued by the ATA and NCCN regarding RAI therapy for HCC. This could account in part for the observed variation in practice patterns and under-utilization of RAI that was observed in this nationally representative sample. RAI therapy for HCC tumors >2 cm and those with nodal and distant metastatic disease is associated with improved survival. Given the relative rarity of HCC, multi-institutional trials should be pursued, along with standardization and reinforcement of published management guidelines. Since specific patient and provider characteristics were associated with the observed variation in practice, attention also should be focused on eliminating potential barriers in access to care among elderly patients, patients without private insurance, and those who do not receive care at academic institutions.
Footnotes
Acknowledgments
The data used in the study were derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigators.
A portion of these data were presented at the 36th Annual Meeting of the American Association of Endocrine Surgeons, May 17–19, 2015, Nashville, TN.
Author Disclosure Statement
The authors have no financial disclosures.