
Abstract
Background:
An increase in the incidence of second primary cancers is the late effect of greatest concern that could occur in differentiated thyroid carcinoma (DTC) patients treated with radioactive iodine (RAI). The decision to treat a patient with RAI should therefore incorporate a careful risk–benefit analysis. The objective of this work was to adapt the risk-estimation models developed by the Biological Effects of Ionizing Radiation Committee to local epidemiological characteristics in order to assess the carcinogenesis risk from radiation in a population of Brazilian DTC patients treated with RAI. Absorbed radiation doses in critical organs were also estimated to determine whether they exceeded the thresholds for deterministic effects.
Methods:
A total of 416 DTC patients treated with RAI were retrospectively studied. Four organs were selected for absorbed dose estimation and subsequent calculation of carcinogenic risk: the kidney, stomach, salivary glands, and bone marrow. Absorbed doses were calculated by dose factors (absorbed dose per unit activity administered) previously established and based on standard human models. The lifetime attributable risk (LAR) of incidence of cancer as a function of age, sex, and organ-specific dose was estimated, relating it to the activity of RAI administered in the initial treatment.
Results:
The salivary glands received the greatest absorbed doses of radiation, followed by the stomach, kidney, and bone marrow. None of these, however, surpassed the threshold for deterministic effects for a single administration of RAI. Younger patients received the same level of absorbed dose in the critical organs as older patients did. The lifetime attributable risk for stomach cancer incidence was by far the highest, followed in descending order by salivary-gland cancer, leukemia, and kidney cancer.
Conclusion:
RAI in a single administration is safe in terms of deterministic effects because even high-administered activities do not result in absorbed doses that exceed the thresholds for significant tissue reactions. The Biological Effects of Ionizing Radiation Committee mathematical models are a practical method of quantifying the risks of a second primary cancer, demonstrating a marked decrease in risk for younger patients with the administration of lower RAI activities and suggesting that only the smallest activities necessary to promote an effective ablation should be administered in low-risk DTC patients.
Introduction
T
Differentiated thyroid carcinomas (DTCs) account for the vast majority of thyroid cancers (5), and maintain to a certain extent the most important features of normal thyroid follicular cells: the ability to accumulate iodine actively, produce thyroglobulin, and remain dependent on thyrotropin (TSH). Usually associated with a good prognosis, DTC treatment includes the surgical removal of the organ and, in most cases, subsequent administration of radioactive iodine (RAI) for ablation of thyroid remnants or treatment of residual or metastatic tumor.
The increased incidence of the disease has led to increasing use of RAI therapy for DTC treatment, even in cases of low-risk cancers in patients with a long life expectancy. This category of patients comprises the vast majority of new cases of thyroid cancer discovered each year (6), and in whom the use of RAI should be carefully weighed against the long-term risks of the treatment. An increase in the incidence of second primary cancers (SPC) would be the most important late effect that could occur in patients treated with RAI. The medical decision process for referral to treatment with RAI should therefore incorporate a careful analysis of the benefits and risks of this therapy, particularly in the case of younger patients with low risk of recurrence (7,8). For this purpose, it is necessary to provide physicians and patients with quantitative information on the risk of developing a SPC due to exposure to a given dose of radiation during treatment.
The purpose of this work was to evaluate the feasibility of adapting the risk-estimation models developed by the Biological Effects of Ionizing Radiation Committee (BEIR VII) (9) to national epidemiological characteristics, using them to quantify the risk of carcinogenesis by radiation in a population of DTC patients treated with RAI. The BEIR VII mathematical models were used to estimate the risk by age, sex, and level of administered radioisotope activity, generating information that allows a more individualized risk–benefit analysis to future patients. As part of this research, the absorbed doses of radiation in critical organs were also estimated in order to determine whether they exceeded the thresholds for deterministic effects.
Methodology
The medical data for 416 DTC patients treated with RAI in two public hospitals in the city of Rio de Janeiro (Hospital Universitário Clementino Fraga Filho and Instituto Estadual de Diabetes e Endocrinologia) between 1972 and 2015 were evaluated retrospectively. The study was approved by the ethics committees of both hospitals. Absorbed doses in four different critical organs were calculated using the dose factors of ICRP Publication 53 (10), and the risk of developing a SPC in these sites were estimated according to the mathematical models published by the BEIR VII Committee (9), relating absorbed doses and carcinogenic risk to population characteristics such as age and risk of DTC recurrence. The American Thyroid Association (ATA) 2009 risk stratification system (without the modifications proposed in the 2015 guidelines) was used to classify the patients according to the risk of recurrence (11,12).
Internal dosimetry
Four organs, all considered critical organs for possible deterministic and stochastic effects of radiation, were selected for absorbed dose estimation and subsequent calculation of carcinogenic risk: the kidney, stomach, salivary glands, and bone marrow. Absorbed doses were calculated using the dose factors (absorbed dose per unit activity administered) tabulated in ICRP Publication 53 (10). These ICRP tables provide absorbed dose factors in mGy/MBq for different levels of RAI uptake by the thyroid tissue at 24 hours post administration of Na131I (0%, 5%, 15%, 25%, 35%, 45%, and 55%). For uptakes differing from these specific values, the absorbed dose-factor values were obtained by linear interpolation. However, absorbed dose factors for the salivary glands were not established by ICRP, so the present study used the dose factors derived by Jentzen et al. (13), which were obtained assuming a low or absent RAI uptake. Once the absorbed doses to critical organs were calculated, the study sought to verify if they exceeded the thresholds for the appearance of deterministic effects. The dose values considered as the threshold for emergence of tissue reaction to radiation were those provided in ICRP Publication 118, supplemented by data from Meredith et al. (14) and Keizer et al. (15). As the consideration of the relationship between risk and benefit of RAI therapy has special importance when discussing the initial treatment of patients with DTC (RAI therapy is less controversial in DTC recurrence), the administered Na131I activity for remnant ablation or adjuvant therapy after thyroidectomy was preferably used for absorbed dose and risk estimation (in 29 cases, the activity administered during recurrence treatment was used because there were no reliable information about the activity used in the first RAI therapy).
Risk models of the BEIR VII Committee report
The BEIR VII report presents risk models to estimate the risk of low-dose radiation carcinogenesis. The risk analysis takes into account sex, age at exposure, dose rate, and other factors, and is mainly based on data from studies of survivors of the atomic bombings of Japan. Studies using data from atomic-bomb survivors concluded that the risk of carcinogenesis is consistent with the dose–response derived at moderate to high doses, and the BEIR VII Committee, based on extrapolation of these data, decided to adopt the linear no-threshold model for radiation stochastic effects.
Two risk-calculation models are used in the BEIR VII report: the excess relative risk (ERR) and the excess absolute risk (EAR). The ERR is defined as the rate of disease in an exposed population divided by the rate of disease in an unexposed population minus 1.0, and the EAR is the rate of disease in an exposed population minus the rate of disease in an unexposed population. These allow the calculation of the risk of cancer induction in a given time after exposure, and its value depends on the sex and age of the individual at the time of exposure. The mathematical model used to estimate the ERR or EAR in solid tumors (other than breast cancer, non-melanoma, and thyroid cancer) is given by equation 1:
in which D is the equivalent dose (Sv); βs , y, and η are ERR- and EAR-specific parameters for various organs and for each sex, as provided in the BEIR VII report (9); e is the age at exposure (years); e* = (e – 30)/10 for e < 30 years and 0 for e ≥ 30 years; and a is the attained age.
The model for leukemia expresses the ERR and EAR as a linear-quadratic function of radiation equivalent dose. The estimated risk of leukemia described in the report is given by equation 2:
in which D is the equivalent dose (Sv), s is the sex, e is the age at exposure (years), t is the time elapsed since the exposure in years, and e* = (e – 30)/10 for e < 30 and 0 for e ≥ 30 years. βS , θ, γ, and φ are parameters given by the model and tabulated in the BEIR VII report (9).
The committee uses a measure named lifetime attributable risk (LAR) to translate the estimated risk of cancer to other populations. LAR can be succinctly defined as the additional cancer risk above and beyond baseline cancer risk, and it depends on the age of the individual at the time of exposure and incorporates a number of additional factors, such as the latency period between exposure and the possible occurrence of cancer, as well as the dose and dose rate effectiveness factor (DDREF). For an individual exposed to a dose D at an age e, the LAR is given by equation 3:
The summation in the above equation is performed in the range a = e + L and a = 100 years, where e is the age at exposure, L is a latency period (two years for leukemia and five years for solid tumors), and a is the attained age. S (a) is the probability of surviving to age a, and S (a)/S (e) is the probability of surviving to the attained age a conditional on the probability of surviving to exposed age e. The conditional probability S (a)/S (e) was derived from the life-span tables of the Brazilian Institute of Geography and Statistics (16).
The term M(D,e,a) can be calculated using the ERR model or the EAR model. Using the ERR to estimate the risk of cancer incidence, M(D,e,a) is given by equation 4:
where λI c(a) is the cancer incidence rate dependent on age and sex. The baseline cancer incidence rates were obtained from the National Cancer Institute (17).
The term M(D,e,a) to estimate the incidence of cancer in the EAR model is given by equation 5:
The BEIR VII committee calculates the LAR values separately based on the EAR and ERR models described above, and then combines them using a weighted average, as shown in equation 6:
where the LAR is obtained by the weighted average of the LAR calculated with the ERR model (LARERR) and the LAR obtained with the EAR model (LAREAR), using a weight w, which varies according to the cancer site. For most types of cancer, the BEIR VII report recommends w = 0.7, showing a preference for ERR for the translation of the risk-prediction model. The initially obtained LAR was divided by a DDREF of 1.5, as recommended in the BEIR VII report.
LAR estimation has various sources of uncertainty and, according to the BEIR VII report, should be regarded as a range of possible values. The confidence intervals calculated in the report to express these uncertainties are partially subjective and quite large, dependent on researcher opinion in addition to direct numerical observation. As an example, the report gives an estimate of LAR for solid-cancer incidence in the female stomach as 43 cases [confidence interval (CI) 5–390] per 100,000 women of mixed age exposed to 0.1 Gy (9).
The ages used for calculating the LAR in women and men were chosen to be the average age of each of the four groups in which the population was divided to analyze the age range of absorbed doses (21, 35, 55, and 75 years, respectively). In addition to the average ages, the average absorbed dose in critical organs was calculated in each of these age groups for each sex, and these values were used to estimate the LAR.
Univariate statistical analysis for description and comparison among groups was performed using the chi-square test for categorical variables evaluation, Student's t-test for analysis of relationships between numeric variables, and one-way analysis of variance for comparing means of three or more groups. The level of statistical significance was set at p < 0.05. Statistical analyses were performed using the StatPlus Pro® v5.9 software (AnalystSoft, Inc.).
Results
The cohort totals 416 patients, and their characteristics are summarized in Table 1. The dose values obtained (absorbed dose average, standard deviation, and the minimum and maximum absorbed dose value found for each organ) are shown in Table 2, and the distribution of the absorbed dose values is displayed in Figure 1. The patient population studied was separated into four age groups to compare the administered Na131I activities and the absorbed doses in critical organs. The overall results, the results separated by age, and those separated by age and sex are shown in Tables 2 –4, respectively.
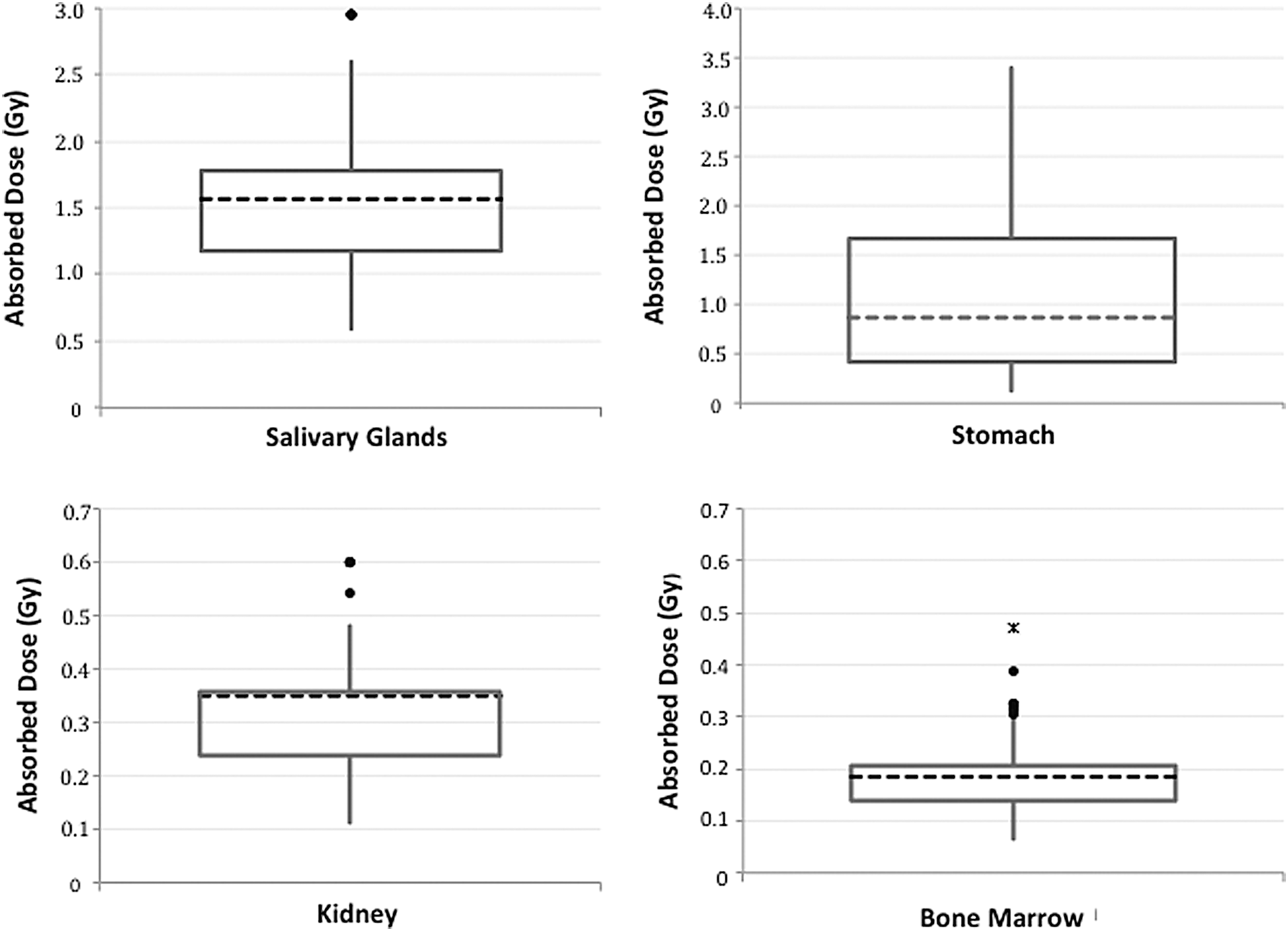
Box plot displaying the distribution of values of absorbed doses (Gy) in four critical organs in 416 differentiated thyroid carcinoma (DTC) patients treated with radioactive iodine (RAI). The dashed line is the median, the black dots are the outliers, and the small x is an extreme outlier.
Average RAI activity administred during the initial DTC treatment (includes 29 cases in which RAI was administered for recurrence therapy because there was no reliable records of the first RAI therapy).
Average cumulative RAI activity administered during the whole DTC treatment.
SD, standard deviation; RAI, radioactive iodine; ATA, American Thyroid Association; DTC, differentiated thyroid carcinoma.
LAR, lifetime attributable risk.
No difference was observed among age groups in relation to the average absorbed doses in the salivary glands (p = 0.83), stomach (p = 0.28), kidney (p = 0.71), and bone marrow (p = 0.76). Likewise, the average administered Na131I activities were similar in the four age groups (p = 0.82), as shown in Table 5.
Statistical analysis of the distribution of the ATA risk categories (low, intermediate, or high) among age groups shows that the two groups <45 years have a lower proportion of high-risk patients (p = 0.04). There was no difference in the distribution of other ATA risk categories (low or intermediate) and in the distribution of the 29 patients classified as “recurrence” (p = 0.17). Evaluation of the average absorbed doses considering only patients classified as low risk showed no statistical difference among different age groups in the salivary glands (p = 0.38), stomach (p = 0.41), kidney (p = 0.34), or bone marrow (p = 0.29). Finally, when separating the average absorbed doses in each age group by sex, there was no statistically significant difference over the age groups in women, with younger patients receiving similar doses to those of older patients (p = 0.28 for absorbed doses in the kidney, p = 0.17 for the stomach, p = 0.46 for the bone marrow, and p = 0.25 for the salivary glands). On the other hand, absorbed doses in men up to 25 years of age were higher than they were in other age groups, but this was statistically significant only in the salivary glands and bone marrow (p < 0.001 and p = 0.04, respectively; p = 0.25 and p = 0.07 for doses variation in the kidney and stomach, respectively). The male patients received in general higher absorbed doses in the kidney (p = 0.037), salivary glands (p = 0.014), and bone marrow (p = 0.049) than women did.
Estimated carcinogenic risk induced by RAI therapy
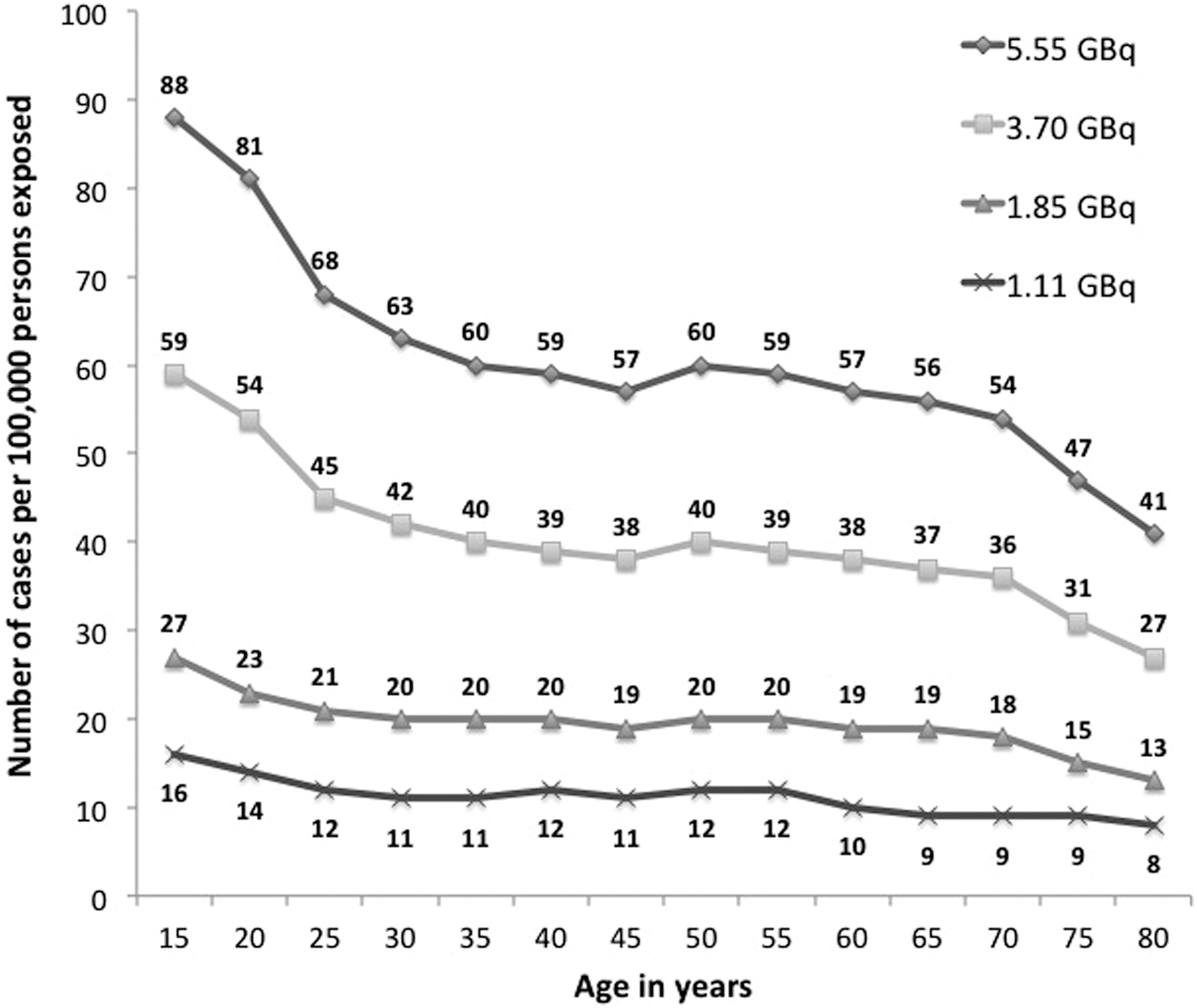
The LAR values for different types of cancer in women are shown in Figure 2, and the LAR values in men are shown in Figure 3. To quantify the effect of reducing RAI-administered activities to DTC patients on the carcinogenic risk, the LAR of incidence of stomach cancer and leukemia in women for various exposure ages to four different activities Na131I were calculated (Figs. 4 and 5). The LAR was calculated only for women because they represent the vast majority of patients with DTC, not only in the cohort of this study but also in the global population affected by DTC (18).
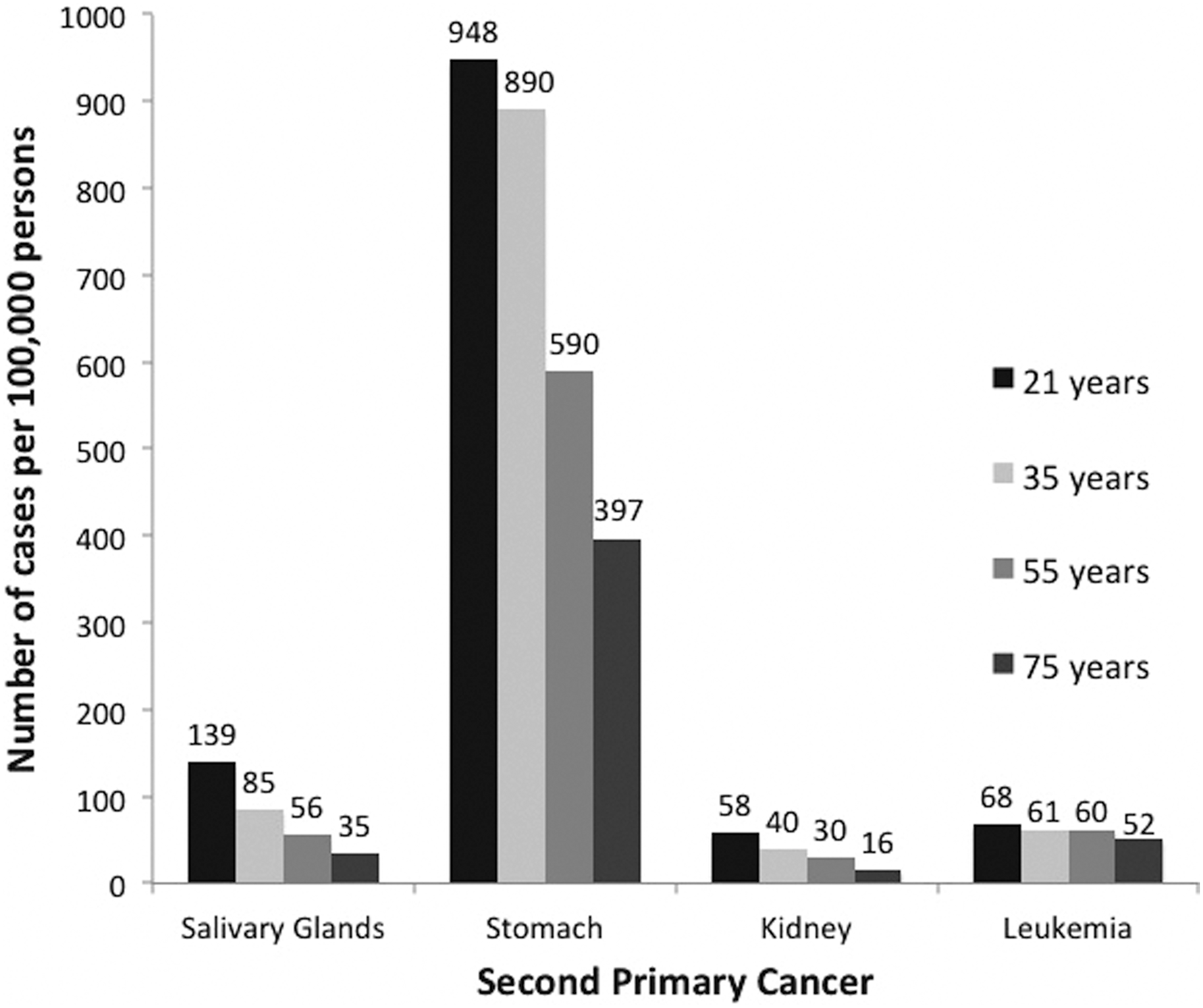
Lifetime attributable risk (LAR) of cancer incidence for four different ages of exposition in women with DTC treated with RAI. The chosen ages are averages of the four age groups into which the patients were divided.
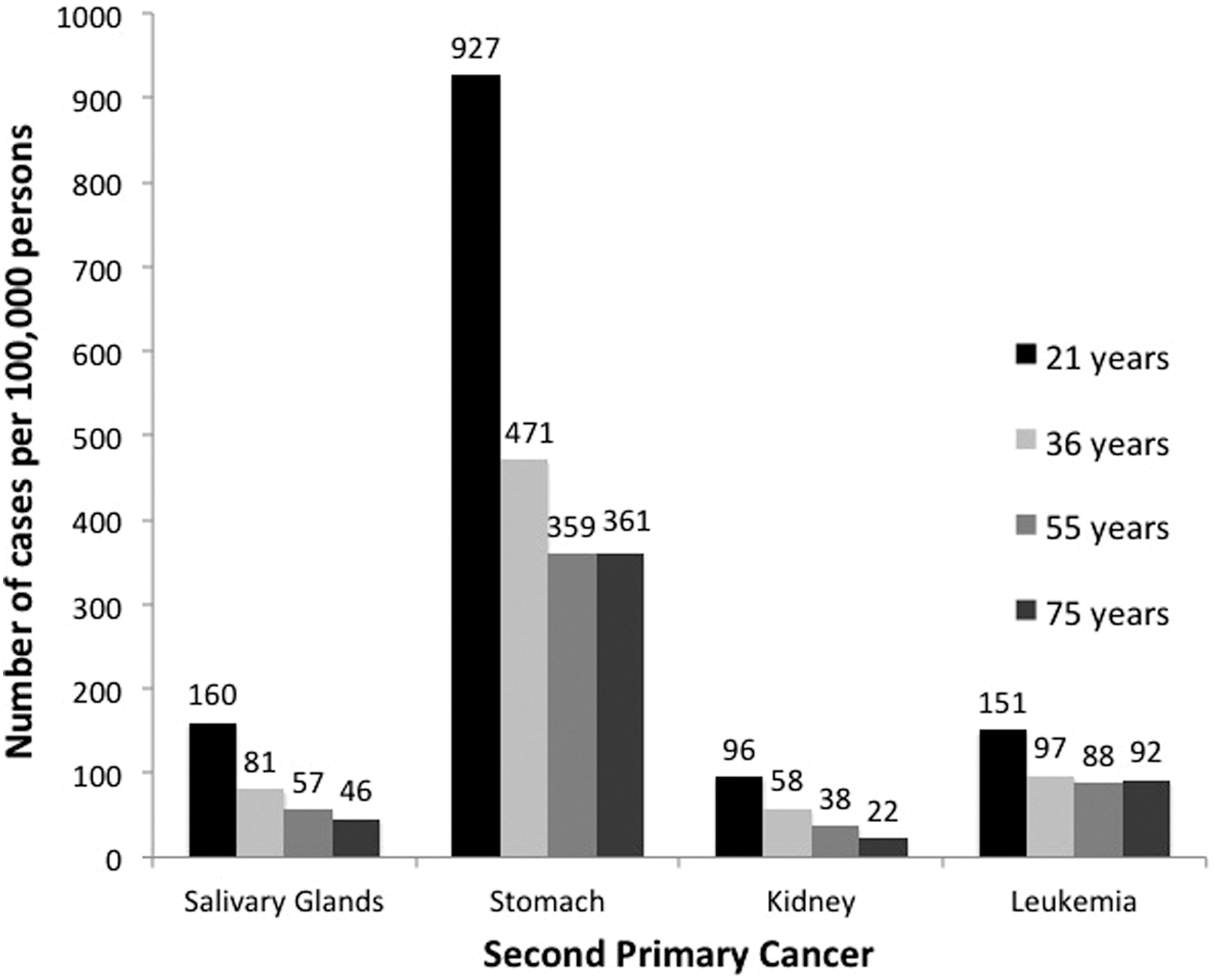
LAR of cancer incidence for four different ages of exposition in men with DTC treated with RAI. The chosen ages are averages of the four age groups into which the patients were divided.
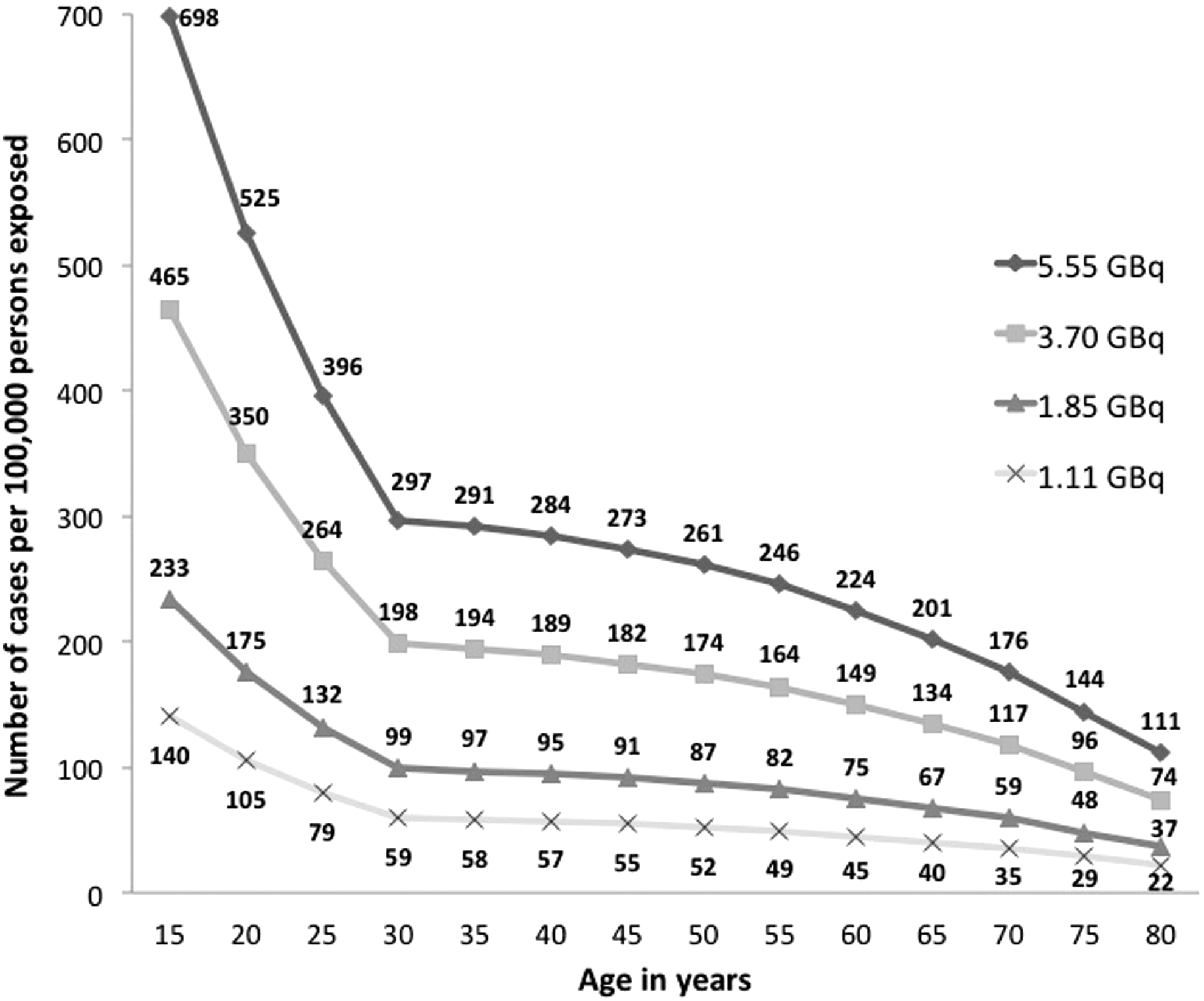
Variation in LAR of incidence of stomach cancer in women, according to age at exposure and administered RAI activity.
Variation in LAR of incidence of leukemia in women, according to age at exposure and administered RAI activity.
Discussion
The biological effects of radiation are traditionally classified into deterministic effects (also called tissue reactions) and stochastic effects (19). Deterministic effects have a threshold for the appearance of damage (derived from cell death), whose severity is directly related to the radiation dose received. Stochastic effects are derived from cellular DNA damage, and in humans are represented basically by the risk of carcinogenesis or, in the case of cancer patients treated with radiation, the risk of appearance of a SPC. The main international organizations of radiation protection consider that there is no threshold for the appearance of stochastic effects, and that the probability of cancer induction varies directly with the radiation dose (9,19,20). The theoretical probabilities of the occurrence of the two types of biological effects of radiation were evaluated in this study.
Tissue reaction or deterministic effect
The absorbed dose in the critical organs studied (the salivary glands, stomach, kidney, and bone marrow) were found to be well below the respective thresholds for severe deterministic effects according to the values established mainly in ICRP Publication 118 (19). The average dose in the salivary glands (1.57 Gy, the highest among the critical organs in this study) exceeded the threshold of 1 Gy established in the empirical study by Jentzen et al. (21) for the transitory deterministic effect of dysfunction in the parotid glands (30% reduction in salivary secretion). However, the same study established a threshold of 3 Gy for submandibular gland dysfunction, and no patient had an absorbed dose in the salivary glands above this value. The absorbed doses in the salivary glands were even further below the 25 Gy threshold for tissue necrosis of the parotid established by ICRP (the highest dose in the salivary glands was 2.96 Gy). In this study, the highest absorbed dose in the stomach was 3.40 Gy compared with a threshold for deterministic effects (ulcers) of 45 Gy. The highest absorbed dose in the bone marrow was 0.47 Gy, well below the 2 Gy threshold for myelotoxicity. In the kidney the highest absorbed dose was 0.60 Gy, again far from the threshold of 15 Gy for impaired renal function.
A single administration of RAI, even at the highest activity levels observed in this study (9.25 GBq), produced an almost negligible risk to patients in terms of tissue damage, suggesting that the RAI therapy is very safe in terms of inducing few, if any, acutely demonstrable adverse effects, at least while it does not achieve higher levels of cumulative activity after multiple treatments.
The absorbed doses in the studied population remained in most cases at similar levels among the age groups, and was found to be as high in young as in elderly patients, even when considering only those patients classified as low risk of recurrence of disease, except for the small group of male patients ≤25 years, whose absorbed doses to critical organs were statistically higher than those of older male patients. Given the increased susceptibility of younger individuals to the stochastic effects of radiation (22), these findings suggest that young patients treated with RAI are being subjected to a perhaps unnecessarily increased risk of developing a SPC.
Variation in the absorbed doses according to RAI uptake in remnant tissue
The dose factors derived by Jentzen et al. for absorbed doses in the salivary gland have a fixed value, but the dose factors established in ICRP Publication 53 to other organs vary according to the value of RAI uptake at 24 hours. The values of the dose factors for the kidney decrease mildly with the increase in the uptake value, and dose factors for the bone marrow and for the stomach increase for greater uptake values. Most of this variation, however, is quite gradual. The administration of 3.7 GBq (100 mCi) of RAI to a patient with an uptake of 0%, for example, would result in an absorbed dose of 0.13 Gy to the bone marrow, while the same activity for a patient with 5% uptake results in an absorbed dose of 0.14 Gy, or 0.17 Gy in an individual with 10% uptake (corresponding to a large amount of remnant tissue). The same values for the absorbed dose would be obtained if the patient with 0% uptake had received 4.0 GBq (approximately 108 mCi) and 4.85 GBq (131 mCi) of RAI, respectively. The amount of remnant thyroid tissue, as reflected in RAI uptake values, certainly has an impact on the estimated post-thyroidectomy internal dosimetry. However, the administered RAI activities are the major factor in the estimation of the absorbed dose to critical organs after RAI treatment.
Risk of SPC after RAI therapy
SPC refers to a new malignancy occurring independently in patients who have or have had other cancer. An increased risk of secondary malignancies after RAI treatment for DTC has been reported in several publications. Rubino et al. (23) studied a cohort of 6841 European patients with a mean age of 44 years, mean follow-up time of 13 years, and average activity administered per patient of 5.99 MBq (162 mCi). In total, 576 secondary malignancies were identified. Compared with the general population, the increased risk of SPC was 27% [CI 15–40%] after RAI therapy. SPCs associated with Na131I treatment included bone and soft tissue, colorectal, salivary gland cancers, and leukemia. Moreover, the increased statistical risk of solid tumors secondary to the primary cancer showed a direct relationship with the administered RAI activity. Rubino et al. concluded that there was an excess absolute risk of 14.4 cases of solid tumors and 0.8 cases of leukemia per 10 years among 10,000 patients with 1 GBq of administered Na131I, leading the authors to recommend reducing the RAI activities used in the treatment of DTC (23). Subramanian et al. (24), in a meta-analysis published in 2007, reported a greater incidence of SPC in thyroid cancer survivors, with an increase in relative risk of 1.20 [CI 1.17–1.24] compared with the general population (based on pooled data from six studies of 70,844 thyroid cancer survivors). The authors related the increased risk to treatment or genetic predisposition. Unfortunately, they did not explore the specific relationship between thyroid cancer treatment and SPM risk in their study. Brown et al. (25) investigated the Surveillance, Epidemiology, and End Results (SEER) database and analyzed 30,278 patients who developed DTC in a 30-year period (1973–2002). Patients who received RAI therapy presented a 16% higher risk of developing a SPC compared with patients who were not treated with RAI [CI1.05–1.27]. Another analysis using the SEER database, this time concentrating on patients with low-risk DTC (T1N0) treated with RAI, was published by Iyer et al. (26). These authors found an increased overall risk of 21% [CI0.93–1.54], corresponding to an absolute excess risk of 4.6 SPC cases per 10,000 person-years.
Sawka et al. (27) conducted a systematic review and meta-analysis comprising 16,502 patients, and found an increased relative risk of 1.19 [CI 1.04–1.36] of a SPC in patients treated with RAI compared with individuals with DTC not treated with this radioisotope. Most studies discussed above compared the incidence of SPCs in DTC patients treated with RAI with the incidence of cancer in the general population. The increase in the number of SPCs demonstrated in those studies does not necessarily imply a causal relationship between RAI treatment and the development of a second malignancy. It is possible that some other underlying factor associated with the thyroid cancer itself may be responsible, or at least contribute to this elevation in the reported incidence of post-therapy cancer. Possibilities include genetic predisposition, exposure to other therapies (chemotherapy, external beam radiation therapy, and/or hormonal therapy), common environmental or dietary factors, and surveillance bias (7,28). An interesting characteristic of the study of Sawka et al. is that the authors tried to avoid the interference of these potentially confounding factors by comparing the incidence of SPC in two groups of DTC survivors: those treated with RAI and a control group who did not receive RAI as part of their treatment.
The carcinogenic risk related to RAI therapy of benign thyroid diseases using lower amounts of radioactivity than for the treatment of DTC was addressed by several studies. The Cooperative Thyrotoxicosis Therapy Follow-up Study Group followed almost 21,000 hyperthyroid patients after RAI therapy given between 1946 and 1964, corresponding to >385,000 patient-years (29). RAI treatment was not associated with a significant increase in cancer mortality (standardized mortality ratio [SMR] 1.02 [CI 0.98–1.06]) or to an elevation in the number of deaths of any specific cancer with the exception of thyroid cancer (SMR 3.94 [CI 2.52–5.86]). As patients dying from thyroid cancer were more likely to have toxic nodular goiter than Graves' disease (30% vs. 8%), the authors suggest the possibility that at least some of the excess thyroid cancer risk is related to underlying thyroid disease (nodular goiter). Holm et al. (30) studied cancer incidence and mortality in about 10,500 Swedish patients receiving RAI therapy for hyperthyroidism. Average absorbed doses to organs other than the thyroid were relatively low, with the highest doses to the stomach (0.25 Gy), and the authors reported that only the risk for stomach cancer increased over time (p < 0.05). Overall cancer risk, however, did not increase with administered RAI dose or with time since exposure. Ryödi et al. (31) published a study assessing the cancer morbidity and mortality in hyperthyroid patients treated with either RAI or surgery in 2015. They reported that the overall cancer incidence was not increased among the hyperthyroid patients compared to their controls (relative risk [RR] 1.05 [CI 0.96–1.15]), but the risk of cancers of the respiratory tract (RR 1.46 [CI 1.05–2.02]) and the stomach (RR 1.64 [CI 1.01–2.68]) was increased among the patients. The overall cancer mortality did not differ between the patients and the controls, and most importantly, the type of treatment did not affect the overall risk of cancer (hazard ratio [HR] for RAI vs. thyroidectomy 1.03 [CI 0.86–1.23]) or cancer mortality (HR 1.04 [CI 0.91–1.21]), indicating that the increased cancer risk in hyperthyroid patients is attributable to hyperthyroidism and shared risk factors, not RAI treatment. A systematic review study by Verburg et al. (32), comprising seven studies (including the works of Ron et al. and Holm et al.) covering a total of 54,510 patients, suggests that the evidence is not conclusive in favor of increased risk of carcinogenesis in RAI treatment for hyperthyroidism. Thus, although the BEIR VII Committee and other international bodies adopt the linear no-threshold risk model for stochastic effects, in practice, studies have failed to prove an increase in the incidence of SPCs in patients treated with RAI activities of up to 1.11 GBq (30 mCi).
It is important to note that none of the mentioned studies kept track of all patients throughout their lives, which is very difficult to do and which may lead to underestimation of the incidence of SPC. On the other hand, as seen in this study, the BEIR VII risk-estimation models add the excess annual risk of patients exposed to radiation to the age of 100 years, which may lead to an overestimation of the results.
This work shows that it is theoretically possible to translate a model developed to estimate the risk of carcinogenesis in the population of another country (Japan) to a local population using national or regional epidemiological and statistical data. In fact, that is exactly the purpose of the LAR model. It would be desirable, however, to have more studies specifically assessing the adequacy of the weights assigned to the EAR and ERR models for the translation of the risk estimation model of different types of cancer to the local population.
According to the estimates obtained for the studied population, the risk of incidence of a SPC is much higher in the stomach, in both women and men. The greatest risk of carcinogenesis in the stomach, in relation to other organs studied, is due to the high gastric absorbed doses combined with a much higher baseline incidence of stomach cancer in the general population compared with the other critical organs analyzed. Cancer of the salivary glands and leukemia are close in terms of incidence risk estimates, although the salivary glands receive a much higher absorbed dose (Table 2). However, besides the greater sensitivity of the bone marrow to the stochastic effects of radiation, cancer of the salivary glands is also less frequent in the general population than leukemia is (17, 33). The risk of inducing a SPC in the kidney is the lowest among the organs studied. The kidney is not a particularly sensitive organ to the carcinogenic effects of radiation (33), and the absorbed doses calculated on this site were much lower than the doses in the stomach and salivary glands, although they were higher than in the bone marrow.
Despite the similar absorbed doses, LAR estimates of cancer incidence in critical organs, particularly solid tumors, demonstrate a markedly increased risk of carcinogenesis in patients <30 years of age. These findings are in accordance with the results of the long-term cohort studies with atomic-bomb survivors (9). The risk of leukemia, although somewhat higher in the younger end of the age spectrum, maintains some stability in the adult age range (Figs. 2 and 3).
The comparison of the estimated risk of a radiation-induced SPC with an activity of 3.70 GBq to the small expected benefit of an RAI ablation, especially in young patients at low risk, strongly suggests that the lower activity effective to promote the elimination of thyroid remnants should be used. The curves obtained with the estimated values of the LAR of incidence of stomach cancer and leukemia for each value of RAI activity show that there is a significant reduction in the risk of carcinogenesis when the radioisotope activities usually administered in clinical practice are reduced. As shown in Figures 4 and 5, the estimated lifetime risk of incidence of stomach cancer and leukemia in a woman treated with RAI at 50 years of age diminishes from 0.17% to 0.05% and 0.04% to 0.01%, respectively, when the administered activity is reduced from 3.7 GBq (100 mCi) to 1.1 GBq (30 mCi). As a comparison, the risk of structural disease recurrence in low-risk DTC patients in the absence of RAI remnant ablation is up to 2% over 5 to 10 years of follow-up (12). Considering that RAI is a probable adjuvant therapy in cases of DTC recurrence, it might be worth considering offering RAI therapy with lower activities for remnant ablation.
Balancing the risks and benefits of RAI therapy
The main goal of post-surgery administration of RAI is to minimize DTC recurrence and death, primarily by eliminating residual microscopic disease (8,34). Even when the main purpose is the ablation of residual normal thyroid tissue, RAI administration presents some additional benefits: it improves the specificity of subsequent measurements of serum thyroglobulin as a tumor marker, increases the sensitivity of detection of metastatic disease on subsequent follow-up RAI whole-body scans, optimizes the therapeutic effect of any subsequent RAI treatment, and provides a post-ablation whole-body scan often revealing unknown local or distant metastases.
Several studies published over the last several decades, especially by Mazzaferri, provide scientific evidence supporting the use of RAI in DTC treatment (35 –38). In 1997, Mazzaferri (37) reported the results of a comparison on the outcome in 1004 patients with DTC who underwent thyroid RAI remnant ablation/therapy (151 patients) or who were either treated with thyroid hormone alone (755 patients) or given no postoperative medical therapy (98 patients). The median follow-up time was 18.7 years for patients treated with thyroid hormone alone, 21.3 years for those given no adjunctive medical therapy, and 14.7 years for those treated with thyroid remnant ablation, and the endpoints measured were cancer recurrence, development of distant metastases, and death due to thyroid carcinoma. Tumor recurrence was about threefold lower (p < 0.001), fewer patients developed distant metastases (p < 0.002) and there were fewer cancer deaths (p < 0.001) after RAI than after other forms of postoperative treatment, an effect observed only in patients with primary tumors ≥1.5 cm in diameter and, in the case of cancer deaths, in patients aged ≥40 years at the time of initial treatment. Nevertheless, the beneficial effects of RAI were not apparent in patients with isolated tumors <1.5 cm that were not metastatic to regional lymph nodes or invading the thyroid capsule, indicating that RAI had no impact on outcomes in patients with low-risk disease. In a systematic review and meta-analysis of the effectiveness of RAI remnant ablation for DTC, Sawka et al. (39) concluded that patients with low-risk DTC may benefit from RAI remnant ablation by decreased risk of locoregional recurrence (RR 0.31 [CI 0.2–0.49]) and decreased risk of distant metastatic disease (absolute decrease in risk 3% [CI 1–4%]). However, the authors point out that results are inconsistent among studies for some outcomes, and the incremental benefit of remnant ablation in low-risk patients treated with bilateral thyroidectomy and thyroid hormone suppressive therapy is unclear.
The recently published ATA guidelines state that there is little evidence to suggest that RAI may improve long-term thyroid cancer outcomes in low-risk DTC patients (12). Thus, the decision to treat low-risk DTC patients with RAI should be undertaken carefully, based on a balance between its risks and benefits. Estimates of radiation carcinogenesis obtained in this study allow us to make a risk–benefit analysis with quantified information about the risk. From the result of this analysis, and based on the number of SPCs predicted by the estimation models, it is strongly recommended that activities >1.85 GBq (50 mCi) should be avoided for remnant ablation in low-risk patients—especially in younger individuals in whom the risk of radiation-induced SPC is greater. The administration of an activity of 1.11 GBq (30 mCi) is probably more appropriate, since there are already important studies demonstrating that the ablative effectiveness of this level of RAI activity (40,41) and its stochastic risk profile are adequate.
A limitation of this study is due to the fact that it is a cross-sectional study in which internal dosimetry was obtained by absorbed dose coefficients, which were calculated based on the kinetics of a standard human model, the so-called reference man. This model may not reflect satisfactorily the average biokinetics of the studied population. However, due to practical difficulties, the nuclear medicine services of the hospitals in which the study was conducted did not perform pre-therapeutic internal dosimetry estimations. On the other hand, the empiric dosimetric evaluation of a few patients would not necessarily reflect the kinetics of the ethnically diverse Brazilian population. Therefore, the use of dose coefficients based on standard human models remains an effective way of retrospectively estimating the internal dosimetry of a large group of patients treated with RAI.
In conclusion, RAI treatment is safe in terms of deterministic effects, because even when high activities are administered, they do not deposit absorbed radiation doses in critical organs that exceed the thresholds for significant tissue reactions. Only the cumulative administration of very high activities may cause more severe deterministic effects. The increased likelihood of a SPC is the most significant adverse effect when using RAI in the treatment of DTC, and the use of mathematical models established by BEIR VII allows the theoretical quantification of the carcinogenesis risk in a local population, facilitating the analysis of the risk–benefit ratio of RAI administration. The models demonstrate the substantial magnitude on the reduction of the risk of SPC appearance when there is a progressive decrease in the administered activity of RAI, reinforcing the importance of administering the smallest activity that is effective for DTC therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.