
Abstract

Goiter and hypothyroidism due to iodine deficiency became rare in the United States after the advent of iodized salt in the 1920s, but they continue to affect an estimated 2.2 billion people living in iodine-deficient areas globally (1,2). The recommended daily iodine intake is 150 μg for non-pregnant, non-lactating adults (3). Approximately 90% of ingested iodine is excreted in the urine, and the remainder is actively transported into the thyroid by the sodium–iodine symporter (NIS) and used to synthesize the thyroid hormones thyroxine (T4) and triiodothyronine (T3). Classification of iodine deficiency is based on median urinary iodine concentration: mild 50–99 μg/L, moderate 20–49 μg/L, and severe <20 μg/L.
A 67-year-old woman presented with a history of hypothyroidism and goiter. Her diet had consisted of only white rice for the past 10 years. Levothyroxine therapy had been recommended, but the patient declined, reporting intolerance to all foods and most medications except for organic white rice. To maintain nutrition, she sprinkled liquid compounded vitamins, amino acids, and electrolytes over her rice. She added iodine via Iodopen to the rice every third day, but then developed an intolerance to iodine.
Her exam revealed a mildly enlarged thyroid gland with an irregular texture. Over a three-month period, her thyrotropin (TSH) values ranged between 2.2 and 12.5 mIU/mL (reference range 0.5–3.5 mIU/mL) and free T4 (fT4) between 0.6 and 0.8 ng/dL (reference range 0.9–1.7 ng/dL). Thyroid peroxidase antibodies (TPOAb) were negative. Thyroid ultrasound demonstrated a 5 mm central cystic nodule and a 3 mm right spongiform nodule.
The patient's food and added dietary supplements, including organic rice enriched with sea salt, Soluvit (water soluble vitamins), pediatric liquid multivitamin, an amino acid and electrolyte blend, and rice supposed to contain 100 μg NaI (Iodopen), were analyzed and did not contain iodine. In addition, her 24 h urine iodine was 14 μg/24 h (reference range 75–500 μg/24 h), 24 h urine creatinine was 1.1 g/24 h (reference range 0.63–2.5 g/24 h), and iodine measured in seven urine samples obtained 1.5 h after ingestion of the Iodopen-enriched rice diet every third day was low at 16–57 μg/L (mean 33 μg/L; reference range 100–400 μg/L). A 24 h 123I uptake was elevated to 43.4%, and a thyroid scan showed diffuse distribution of the 123I (Fig. 1).
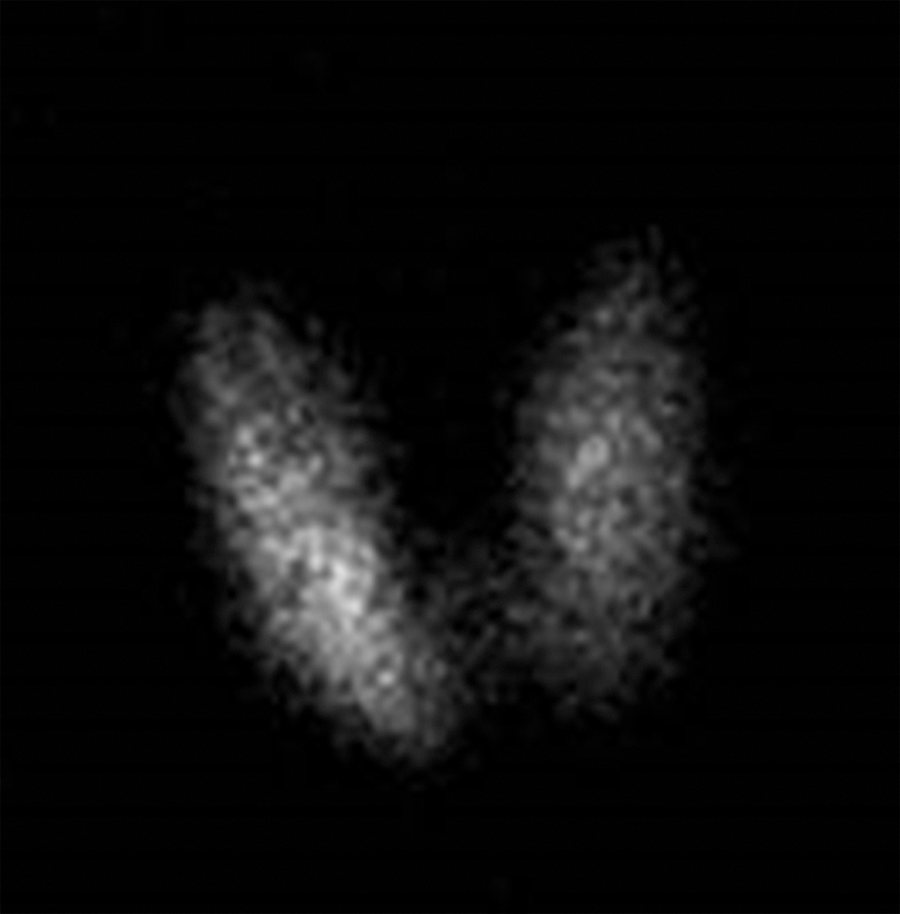
Twenty-four-hour 123I scan in an iodine-deficient patient.
In the United States, severe iodine deficiency is rare, but it should be considered, as low salt intake is now recommended and sea salt and kosher salt do not contain iodine unless added by the salt manufacturers and specified on the labels. Furthermore, vegans are moderately iodine deficient, since they do not consume dairy products, a major source of dietary iodine (4). Determining the median iodine in 10 daily spot urines can be helpful in making the diagnosis of iodine deficiency. An increased 24 h radioactive iodine uptake and goiter, while usually associated with hyperthyroidism, may be due to iodine deficiency, as was observed in this patient.