
Abstract
Background:
The incidence of pediatric differentiated thyroid carcinoma (DTC) has been rising in recent years, and the main risk factors for recurrence are lymph node and distant metastasis at diagnosis. Other clinical features remain unclear, such as the impact of age, sex, and puberty. Furthermore, until now, this population has been treated using the same strategies used to treat adults. In 2015, the American Thyroid Association (ATA) published the first guidelines targeted at this age group. The aims of this study were to investigate the prognostic factors for early and long-term remission and also to validate the ATA risk stratification proposal in a population outside the United States.
Methods:
Clinical records from 118 patients <18 years old followed in two referral centers were reviewed. The median age was 12 years (range 4–18 years), and 20.3% (24 patients) were <10 years old at diagnosis. The median follow-up was 9.1 years. The majority were female (72%) and received total thyroidectomy and radioiodine therapy (RAI), and 61.8% were treated with more than one dose of RAI. The majority were classified as high risk (48.3%) by the new ATA pediatric guidelines due to distant metastasis (30 patients) or extensive lymph node involvement (27 patients). The remained were classified as low risk (31.3%) and intermediate risk (20.4%).
Results:
Females with no lymph node or distant metastasis and low ATA pediatric risk were more likely to have no evidence of disease (p < 0.05) within the first year and also in the long term. In this study, age did not significantly predict outcomes. Furthermore, patients also benefitted from multiple doses of RAI, but when the cumulative activity was >400 mCi, this benefit was diminished.
Conclusions:
This study shows that the ATA risk stratification proposal for pediatric patients is useful in predicting early and long-term outcomes in pediatric patients with DTC. In addition, it shows that sex and metastatic disease are important prognostic factors in pediatric populations.
Introduction
D
As observed in the adult population, the most common subtype of DTC is papillary thyroid cancer followed by follicular thyroid cancer, with medullary and poorly differentiated thyroid carcinoma being very rare in children (7). DTC is also more frequent in females of all ages (7 –9), but in young children, especially those who are pre-pubertal, the male-to-female ratio seems to be lower than that in older individuals (10).
The initial presentation in children and adolescents appears to be more aggressive than it is in adults (1,9,11,12), with a higher incidence of lymph node metastasis and distant metastasis, despite the apparent paradox of having an extremely low cancer-specific mortality rate (13 –16).
The reasons for the distinct presentation and prognosis in children and adolescents are not completely clarified, but they may be a reflection of specific metabolic and genetic characteristics of DTC in this age group. Recent studies showed that younger and pre-pubertal patients had a lower expression of the Na+/I− transporter (NIS), pendrin, thyrotropin (TSH) receptor, and DUOX in follicular cells (15,17) than post-pubertal patients and adults did. Clinically, it has also been suggested that younger children may have a more aggressive presentation than adolescents (18 –20). However, those studies included very few patients <10 years old and/or pre-pubertal patients.
Due to the many peculiarities and differences that are observed between adults and children, in 2015, the American Thyroid Association (ATA) published guidelines for children with thyroid nodules and DTC to provide recommendations for the evaluation and management of this disease in this specific group (21).
The aims of this study were to evaluate patients with DTC diagnosed <18 years of age in order to analyze the factors that may influence the success of initial therapy and long-term prognosis, and to validate the recently published ATA pediatric risk classifications for DTC.
Patient and Methods
This is a retrospective study of a cohort of patients diagnosed with DTC <18 years old. The data were gathered from the files of the Federal University of Rio de Janeiro (UFRJ) and of the National Cancer Institute (INCa). Between March of 1977 and December of 2015, 118 pediatric patients (≤18 years) with DTC were initially treated in both institutions. The initial thyroid surgery was either total thyroidectomy or partial thyroidectomy, and therapeutic neck dissections were routinely performed for clinically apparent abnormal cervical lymphadenopathy. In both institutions, it has not been the practice to perform prophylactic neck dissections in DTC. After obtaining the final pathology report, completion thyroidectomy was performed if indicated. Radioactive iodine (RAI) therapy with 131I was performed within two to six months after surgery for thyroid remnant ablation or therapy of distant metastases, and suppressive doses of thyroxine (TSH <0.05 mIU/L) were administered after initial treatment. Patients with medullary thyroid carcinoma or anaplastic thyroid carcinoma were excluded.
RAI therapy with 131I was repeated when patients presented with persistently elevated thyroglobulin (Tg) levels and if they showed significant uptake on the previous post-therapy whole body scan (WBS) and/or evidence of iodine-avid disease on a diagnostic WBS. The minimum interval for re-treating was 12 months. Diagnostic WBS was not routinely performed. The same group of physicians followed these patients throughout the entire treatment time. The activity of RAI administered was decided in a multidisciplinary board based on the postoperative pathology report, children's body surface, and the presence of lymph nodes or known distant metastases.
Laboratory studies
From 1977 to 1985, the functional sensitivity of the serum Tg assays was approximately 5 ng/mL. Between 1985 and 2000, a variety of Tg assays was used with functional sensitivities of approximately 1 ng/mL. Between 1986 and 1997, a variety of Tg assays was used with functional sensitivities of approximately 1 ng/L. From 1998 to 2001, a Tg assay with a functional sensitivity of 0.5 ng/L was employed. Starting in 2001 until 2010, serum Tg was quantified by a immunometric assay (Immulite) with a functional sensitivity of 0.2 ng/L, and from 2010 until today, the functional sensitivity dropped to 0.1 ng/L.
Evaluation of outcomes
Clinicopathologic features, treatments, and outcomes, such as age, sex, histology, specific variant, tumor size, extrathyroidal extension, tumor stage, presence of pathological node metastases, extension of thyroid resection and node dissection, and data from radioactive iodine therapy, were obtained. These factors were compared between patients, independent of their responses to the initial therapy. The patients were stratified by the following systems of risk categorization: Tumor, Node, Metastasis (TNM), employed by the American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) (22), which is widely used for all types of cancers; and the recently published ATA risk classification for DTC designed for children and adolescents (21).
Patients were considered to have no evidence of disease (NED) at the final follow-up if they had a suppressed serum Tg <1 ng/L, no detectable Tg antibodies, and no structural evidence of disease. Patients with suppressed Tg values >1 ng/L, stimulated Tg values >2 ng/L, or any evidence of disease on cross-sectional imaging (ultrasound, computed tomography [CT] scan, or magnetic resonance imaging), functional imaging (RAI scan or 18-FDG-PET scan), or biopsy-proven disease (cytology or histology) were considered to have persistent disease, either biochemical or structural. A recurrence was defined as new biochemical (suppressed Tg >1 ng/L and/or stimulated Tg >2 ng/L), structural, or functional evidence of disease that was detected following any period of NED. Progression was defined as patients with structural disease that showed any growth at the time of the last visit when the data were collected.
The ethical boards of both institutions involved approved this study. Informed consent was obtained from patients and/or their parents.
Statistical analysis
Numeric variables were expressed as the median and range when the distribution was not normal, and the mean and standard deviation when appropriate. For the first year and long-term outcomes, a simple exploratory analysis was performed using Cox's model, from which all significant variables were used to build a multiple model in which hazard ratios (HR) and their confidence intervals (CI) were calculated to predict the impact of the study variables. The HRs and HRs adjusted for each variable were compared to verify differences in magnitude that may indicate a modifying effect and/or confounders. The proportional hazards assumption was verified using Schoenfeld residuals. The Kaplan–Meier method was used to estimate survival, considering the time of initial therapy until remission. Log-rank and Peto tests were used to determine the factors associated with event-free survival. “Event free” was defined as the absence of persistence or recurrence of cancer. Differences were considered statistically significant when their corresponding p-values were <0.05. These analyses were performed using survival package from R software.
Results
The demographic and clinical characteristics and initial management are shown in Table 1. The majority of patients were female (72%), the youngest was four years old, and the oldest was 18 years old (median age = 12 years). Twenty-four patients were ≤10 years old at diagnosis, nine of whom were male. The mean tumor size was 2.8 cm, with 20% (24 patients) having a tumor >4 cm, and only 6.8% (eight patients) having tumors <1 cm. The median follow-up was 9.1 years. There were 111 (94%) patients with the classic variant subtype, and only seven (6%) patients with the follicular variant type. Patients who underwent total thyroidectomy corresponded to 82% (97 patients) of the sample, and 92.4% (109 patients) of patients received at least one initial therapeutic dose of RAI. The majority of patients had lymph node metastasis at the time of diagnosis (66%), and approximately 25.5% had distant metastasis, all in the lungs (Table 1). The patients were also stratified by risk of mortality and of recurrence/persistence. Using the TNM staging system 7th edition (22), as they were all <45 years old, 89 patients were in TNM stage 1 and 30 in stage 2. To predict recurrence, the ATA pediatric risk stratification system was used; 57 (48.3%) were considered high risk, 24 (20.4%) intermediate risk, and 37 (31.3%) low risk. As also shown in Table 1, the majority of patients had NED at the end of follow-up, a third still showed some evidence of disease, and five showed progression. Four of the five progressive patients had cervical lymph nodes that were enlarged, and one had an increase in the size and number of his lung metastasis, but they were still <1 cm. Only nine patients were not treated with at least one dose of RAI. Six were low risk, two intermediate ATA pediatric risk, and one high risk, but she had undetectable stimulated Tg three months after surgery. They all had NED at the end of follow-up. There were no deaths related to this cancer during follow-up.
RAI, radioactive iodine; TNM, Tumor, Node, Metastasis staging system; ATA, American Thyroid Association; NED, no evidence of disease.
Regarding the prognostic factors, two analyses were performed. In Table 2, the main predictors of early NED (within the first year after initial therapy) are shown. Girls, those with no lymph node metastasis at diagnosis, and those classified as low risk by the ATA pediatric risk stratification system (21) were more likely to have NED within the first year. Unifocality was marginally significant for the same outcome. None of the patients who presented with distant metastasis achieved NED within the first year. Age was not significant. However, the proportion of males showed a tendency to be higher at a younger age at 37.5% compared with 25.5% in patients younger and older than 10 years, respectively.
p-Value significant at <0.05. Statistically significant values are shown in bold.
None of the patients with distant metastasis at diagnosis were free of disease in the first year.
DTC, differentiated thyroid carcinoma; HR, hazard ratio; CI, confidence interval.
The second analysis focused on the long-term prognostic factors. The follow-up periods lasted up to 32 years, and female sex, the absence of lymph node metastasis, and the ATA pediatric risk stratification system remained factors related to better outcomes, even in longer periods of observation. Additionally, 33% (seven patients) of the group that presented with distant metastasis had NED at the end of the observation period. They all had diffuse lung disease with <1 cm on the CT scan. They had negative WBS when performed, no image or only residual calcified nodules on the CT scan, and undetectable stimulated Tg levels with negative antibodies. The presence of distant metastasis was shown to be a factor with a negative impact on NED in the long term. Neither age nor histology was significantly different in the cohort (Table 3 and Fig. 1).
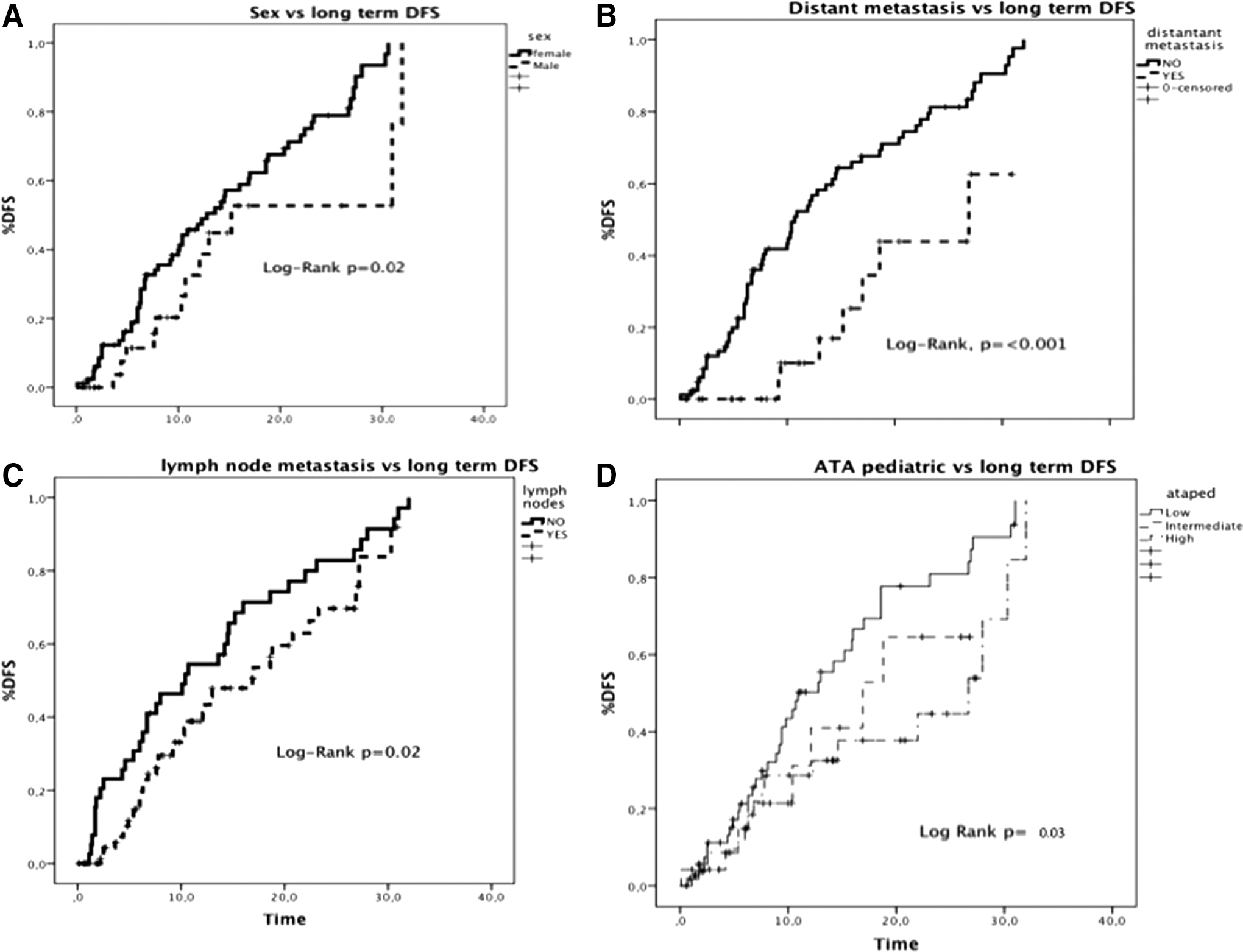
Prognostic factors related to long-term disease-free survival (DFS). (
p-Value significant at <0.05. Statistically significant values are shown in bold.
Cumulative RAI activity was also analyzed in these patients. Figure 2 shows that there was a significant increase in patients who achieved NED when they were submitted to multiple doses (p < 0.001), particularly when the doses increased from 100 to 200 mCi. However, in this population, very few additional patients achieved NED after >400 mCi of cumulative activity of 131I (p < 0.05). Initial body weight was available for 89 (75.4%) patients. When cumulative RAI activity was analyzed according to body weight and final status, 38 patients had NED with 1–5 mCi/kg, rising to 5–10 mCi/kg in 12 patients, and no additional patients reached remission >10 mCi/kg (p = 0.0001).
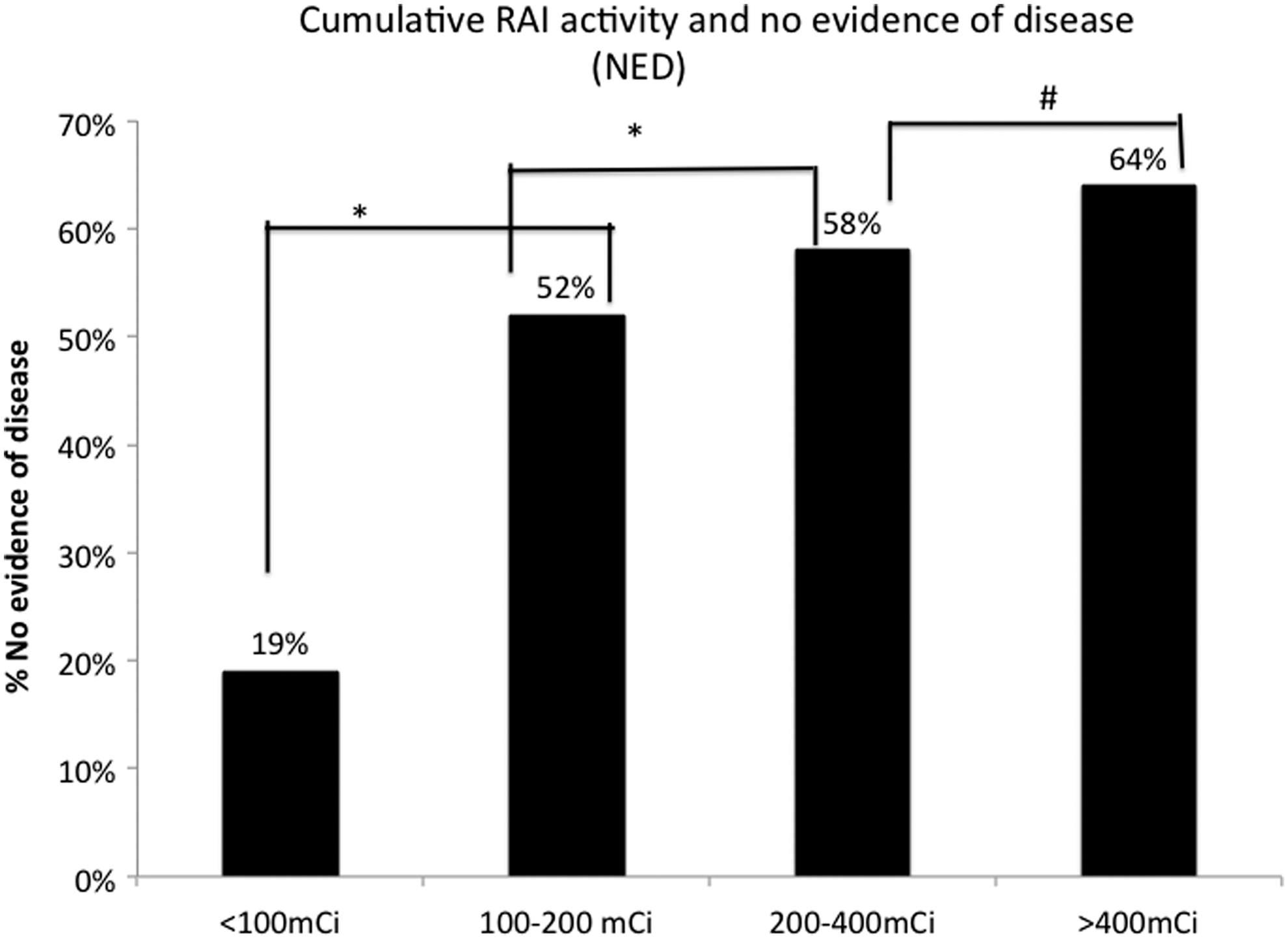
Patients treated with a cumulative radioiodine activity of <100 mCi were less frequently with no evidence of disease than those treated with 100–200 mCi were (p < 0.05) and also than those treated with a cumulative activity of 200–400 mCi compared with 100 mCi and 100–200 mCi. However, the benefit of further treatment was not seen >400 mCi.
Regarding RAI side effects in this cohort, one patient was seen with a parotid adenoma after 12 years of RAI with a cumulative activity of 950 mCi, and two with transient leucopenia, one after a cumulative activity of 350 mCi and the other after 600 mCi. Both had a spontaneous recovery. One patient with diffuse lung metastases had an asymptomatic mild expiratory flow limitation shown by spirometry. Twenty-five of the 85 females became pregnant during follow-up with no pre- or postnatal complications, and no infertility issues were reported.
Discussion
WDTC in children seems to be a distinct disease from that in adults, and the recent effort to create a task force and publish guidelines targeted to pediatric patients is highly important. This study validates the stratification of the ATA pediatrics guidelines in a Latin American population and also with a considerably large sample size of patients <10 years old at diagnosis followed at a single center. The findings of the study demonstrate that stratification using the ATA pediatric guidelines is useful in predicting recurrence risk in children and adolescents, especially in predicting remission in those with a low risk of recurrence. Interestingly, the intermediate- and high-risk groups behaved similarly within the first year of follow-up but differed markedly in the long term. This finding suggests that intermediate-risk ATA pediatric patients have a higher probability of achieving remission in the long term than high-risk patients, but this takes longer to occur than in low-risk patients.
Regarding the clinical presentation and outcomes, in the present study, there was a high incidence of lymph node metastasis (66%) and distant metastasis (25.5%). Golpanian et al. also found a higher incidence of lymph node metastasis, especially in those with tumors >1 cm. As was also observed in other studies, the metastatic spread to cervical lymph nodes was associated with an increase in recurrence rate but not survival (6). In the present data, the survival rate was 100%.
Previous data corroborate the findings of the present study and demonstrate a higher proportion of female sex in children with DTC. The proportion of females was 74.4% in patients aged >10 years and 62.5% in patients ≤10 years old (8,23). Furthermore, this study shows that male patients may exhibit a more aggressive disease course than females do, either within the first year or long term, showing a higher frequency of persistent disease at the end of follow-up. Similar to other studies, this study show that lymph node metastasis and distant metastasis are the most important predictors of persistent disease (13 –15). Age is not a significant risk factor for recurrence/persistence, as reported in other studies (19,20). Nevertheless, some authors found that younger children have a higher risk of relapse (24,25).
The choice of initial therapy is crucial for the long-term outcomes in this population. Most of the studies observed that total thyroidectomies are better than partial surgeries. Patients who received RAI as part of their initial treatment and those who received higher cumulative activities, especially >100 mCi, had a lower probability of recurrence than those who underwent a less intensive therapy (25 –27). In this study, patients who received higher cumulative doses of RAI, in particular doses >200 mCi, were more likely to be cured than those who received lower doses, and there was an important improvement in remission rates when patients were submitted to an additional course of RAI. However, as there is not a control group, it is not possible to know how those patients would behave if the subsequent RAI therapy was held for longer. In a study with >10 years of observation, Biko et al. showed that Tg levels in children and adolescents may decline over the years without additional therapy (28), which might suggest that a good response is being attributed to re-treatment but could happen spontaneously. There are still many controversies regarding the type of initial treatment to administer in this population and the safety of higher activities of RAI. Chow et al. reported a reduced risk of recurrence in patients who received RAI, and similar to the present findings, they did not detect secondary malignancies related to the therapy (15). Other authors have also reported that RAI appears to be safe (14,29). Marti et al., however, found an increase of 4.4 excess cases per 10,000 people per year for secondary primary malignancies, especially of primary salivary carcinomas (30). Some degree of mild myelosuppression was also reported (30,31). It is important to use RAI selectively, and there is no evidence of benefit in patients without local or distant metastasis and in those with intra-thyroidal disease. In the 2015 pediatric ATA guidelines (21), RAI was recommended for every patient as the initial therapy, unless the criteria for remission is already achieved after surgery (stimulated Tg <2 ng/mL and no uptake of iodine in the thyroid bed), and multiple treatments with RAI are only recommended for persistent locoregional or local disease that cannot be resected or for presumed iodine-avid distant metastasis. Treatment should be based on the increased risk of recurrence/persistence instead of the overall mortality, and lifelong follow-up is required (32 –36). Many studies showed that all patients should be treated with TSH suppression (12,37,38), but further careful analyses are needed because the regulation of the hypothalamus–pituitary–thyroid axis can differ in children (39).
In conclusion, this study shows that males and those with lymph node and distant metastasis are more likely to have persistent disease in the long term. Additionally, it shows that the recently proposed risk stratification for children and adolescents is a useful tool in predicting outcomes and can help to tailor the initial therapy and follow-up intensity in order to avoid overtreatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.