
Abstract
Background:
Radiation exposure, especially in childhood, is known to increase the risk for the development of thyroid cancer. However, the prognosis of patients with thyroid cancer with a history of radiation treatment exposure remains unclear.
Methods:
One hundred and sixteen patients with a previous history of radiotherapy in the head and neck region were identified from an institutional database of 3664 patients with differentiated thyroid cancer treated between 1986 and 2010. Using the Kaplan–Meier method, disease-specific survival and recurrence-free survival were compared between patients with (RT; n = 116) and without (No RT; n = 3509) a prior history of radiation exposure.
Results:
The median ages of the RT and No RT cohorts were 52 and 47 years. The median follow-up for both groups was 54 months. Patients who had a prior history of radiation treatment exposure were more likely to be male (38.8% vs. 26.9%; p = 0.005) and older than 45 years of age (67.2% vs. 53.9%; p = 0.005). Other patient, tumor, and treatment characteristics were similar between the groups. There was no difference in the five-year disease-specific survival of the RT and No RT patients (97.4% vs. 98.7%; p = 0.798). The five-year recurrence-free survival was also similar between the RT and No RT patients (97.8% vs. 94.9%; p = 0.371).
Conclusion:
The findings suggest that differentiated thyroid cancer patients with a history of prior radiation treatment exposure have similar outcomes to those with no history of head and neck radiation exposure.
Introduction
T
Initially, an aggressive clinical nature was implicit with these radiation-related thyroid malignancies. Several studies concluded that a more destructive clinical course of PTC was evident in short latency cases, as well as a higher recurrence rate (5 –7). More aggressive pathological features, such as the prevalence of extrathyroidal extension (ETE), were described (8,9). The molecular biology of these exposure related tumors is related to increased frequency of RET rearrangements (10,11). Specifically, an increased frequency of RET-PTC3 rearrangements was observed. RET-PTC3 has been associated with solid, less differentiated papillary tumors, which are thought to produce a more aggressive progression of disease (5,12).
Although the clinical behavior of thyroid cancer due to radiation exposure from nuclear plant radiation exposure has been well described (13 –16), there is little published data on long-term outcomes of differentiated thyroid cancers induced by therapeutic radiation exposure from external beam radiotherapy. The aim of this study was to characterize the nature of therapeutic radiation-associated tumors further in order to determine if a more aggressive course is implicit, leading to poorer outcomes and prognosis.
Methods
Following Institutional Review Board approval, 116 patients with a previous history of radiotherapy to the head and neck region (RT) were identified from an institutional database of 3664 patients with differentiated thyroid cancer treated between 1986 and 2010. Thirty-nine patients with a self-reported history of Chernobyl exposure were excluded from analysis, as duration and proximity of exposure could not be verified from retrospective review. The inclusion criteria are shown in Figure 1.
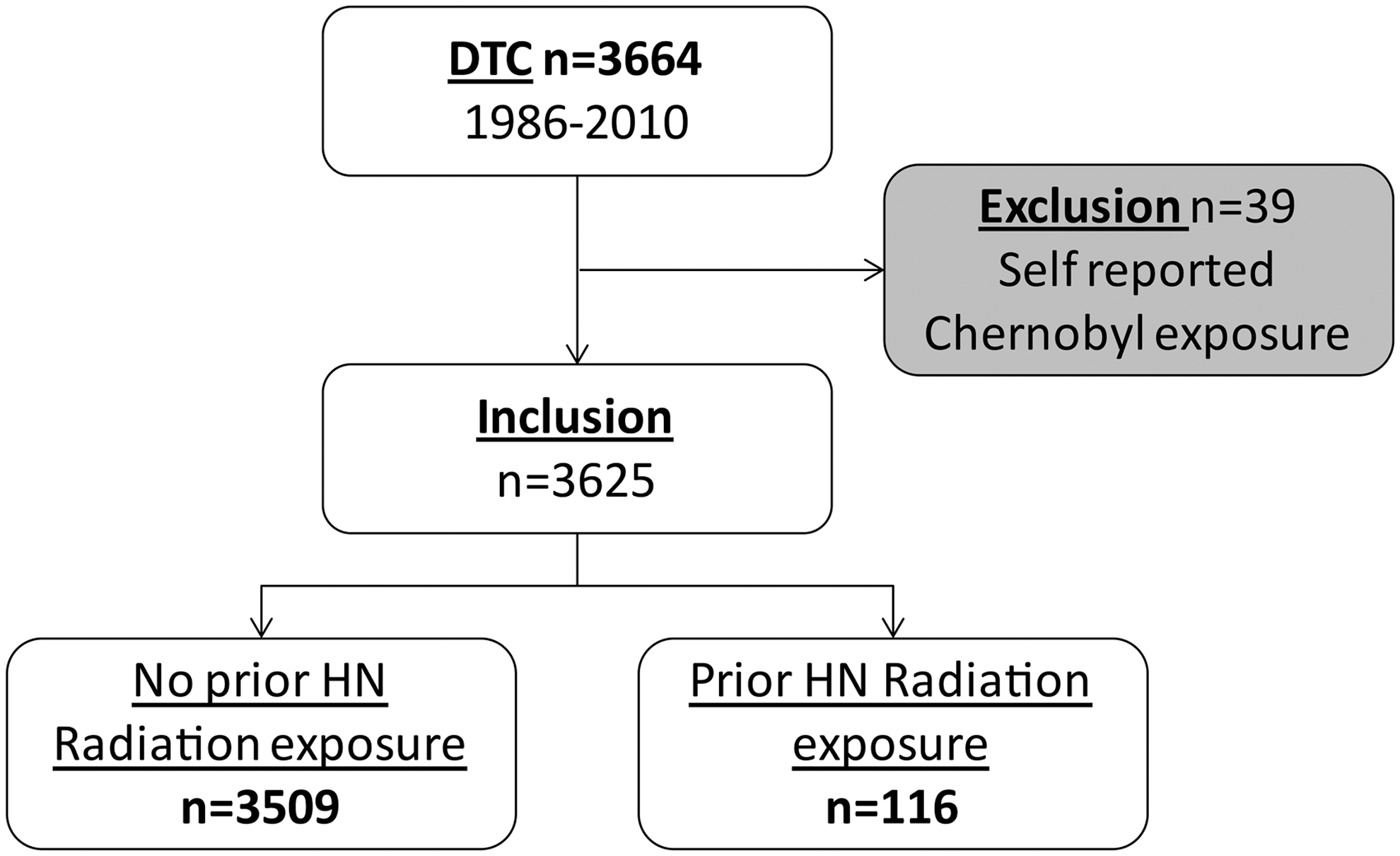
Inclusion criteria.
Patient demographics and primary surgical and histopathological details were recorded. Details of the 116 patients with previous therapeutic radiation exposure were also recorded. The date, location, and treatment of all recurrence events, as well as last follow-up with a Memorial Sloan Kettering Cancer Center (MSKCC) physician from the thyroid cancer multidisciplinary team, were recorded.
The institutional policy is not to perform elective central or lateral neck dissections. The follow-up for locoregional recurrence during the early years of this cohort was based on preoperative clinical examination, and if enlarged lymph nodes or thyroid-bed nodules were palpated, ultrasound (or other imaging studies) and fine-needle aspiration were performed. From 2000 onwards, preoperative ultrasound was increasingly used for the assessment of the central and lateral compartment lymph nodes. Postoperative thyrotropin (TSH) suppression was practiced based on recurrence risk for all patients.
Disease outcomes included disease-specific survival (DSS) and recurrence-free survival (RFS). Locoregional recurrence events required biopsy confirmation. Biochemical disease in the absence of imaging disease was not considered sufficient evidence of tumor recurrence. Distant recurrence events were determined from imaging studies with or without biopsy confirmation. Imaging studies to detect recurrence included ultrasound, diagnostic radioactive iodine (RAI), and computed tomography and positron emission tomography scans. DSS was calculated using the date of last follow-up with an MSKCC physician from the thyroid cancer multidisciplinary team. All patients with evidence of active structural disease at the time of last follow-up and who died during follow up were considered to have had disease-specific death. Details of death were determined from the social security death index and hospital records.
Statistical analysis was carried out using SPSS v21 (IBM Corp., Armonk, NY). Patients with and without prior RT exposure were compared using Pearson's chi-square test. Survival outcomes were analyzed using the Kaplan–Meier method. Outcomes data were calculated at five years. Univariate analysis was carried out by the log rank test. A p-value of <0.05 was considered significant. A multivariable Cox proportional hazards model for RFS was used to determine the unadjusted and adjusted hazard ratios for prior radiation.
Results
Indications for initial radiotherapy to the head and neck
A total of 116 (3.3%) patients had a prior history of radiotherapy to the head and neck region. The patients received radiation between the years 1929 and 2009. The median age at radiation treatment was 28 years (range 5–77 years). The median time from radiation treatment to thyroid cancer diagnosis was 23 years (range 1–73 years). Figure 2 shows the initial indication for radiation to the head and neck. The most common indication was for treatment of hematological malignancies (40%), followed by primary head and neck cancers (34%). Radiation was also used in the treatment of a range of benign skin and glandular conditions (30%). The doses of radiation ranged from 40 Gy for hematological conditions to 66 Gy for head and neck cancers. The radiation was delivered with parallel opposed fields prior to 2000 and by intensity-modulated radiation therapy (IMRT) after 2000. Details of dose and fields of radiation for patients who had received radiation at outside institutions were not available.

Indication for prior head and neck radiotherapy.
Comparison of patient, tumor, and treatment characteristics
Table 1 shows the comparison between those with and without radiation exposure. The median ages of the RT and No RT were 52 and 47 years at the time of surgery. The median follow-up time for both groups was 54 months (range 1–313 months and 13–332 months, respectively). Patients who had a prior history of radiation exposure were more likely to be male (38.8% vs. 26.9%; p = 0.005) and older than 45 years of age (67.2% vs. 53.9%; p = 0.005).
Statistically significant values are shown in bold.
Less than TT includes thyroid lobectomy, isthmusectomy, and subtotal thyroidectomy.
RT, radiation theray; TT, total thyroidectomy; ETE, extrathyroidal extension; RAI, radioactive iodine.
Treatment characteristics were similar between the RT and No RT patients, including the extent of thyroidectomy (p = 0.717), neck dissection (p = 0.063), and use of postoperative RAI therapy (p = 0.097). Tumor characteristics were similarly distributed between the two groups. The groups were also comparable in terms of histology (p = 0.159), ETE (p = 0.261), multicentricity (p = 0.985), T stage (p = 0.054), N stage (p = 0.079), and M stage at presentation (p = 0.602).
Outcomes
No difference was detected in the five-year DSS of RT and No RT patients (97.4% vs. 98.7%; p = 0.798; Fig. 3). Similarly, there was no significant difference in five-year RFS between RT and No RT patients (97.8% vs. 94.9%; p = 0.371; Fig. 4). To determine if RT was a predictor for recurrence, a Cox proportional regression analysis was carried out calculating unadjusted and adjusted hazard ratios for RFS (Table 2). As expected, the traditional factors of age, sex, T stage, N stage, and M stage had significant hazard ratios on unadjusted analysis, which remained significant after adjusting for other variables. Previous RT was not significant, even after adjusting for these other variables.
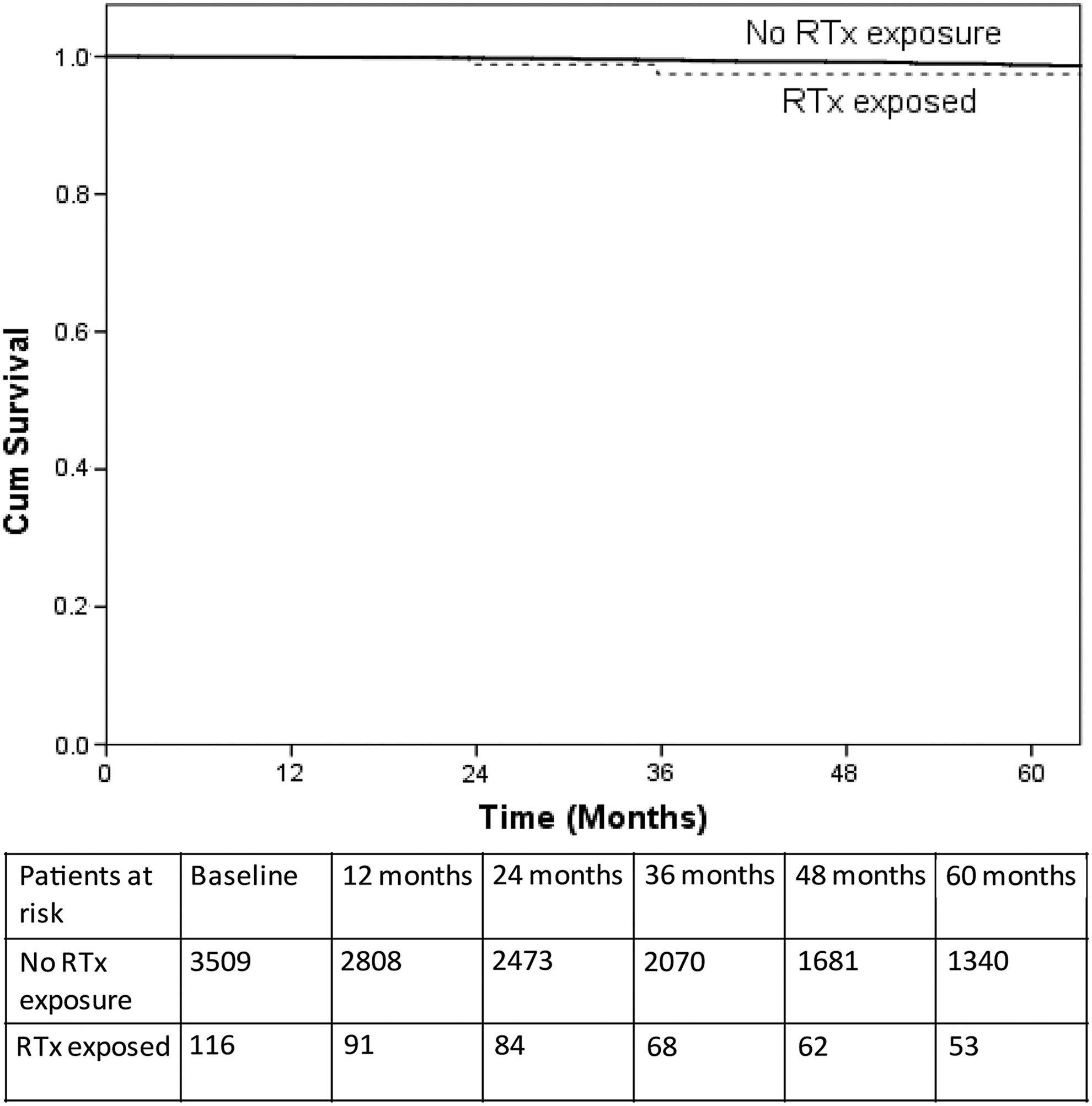
Kaplan–Meier graph for five-year disease-specific survival.
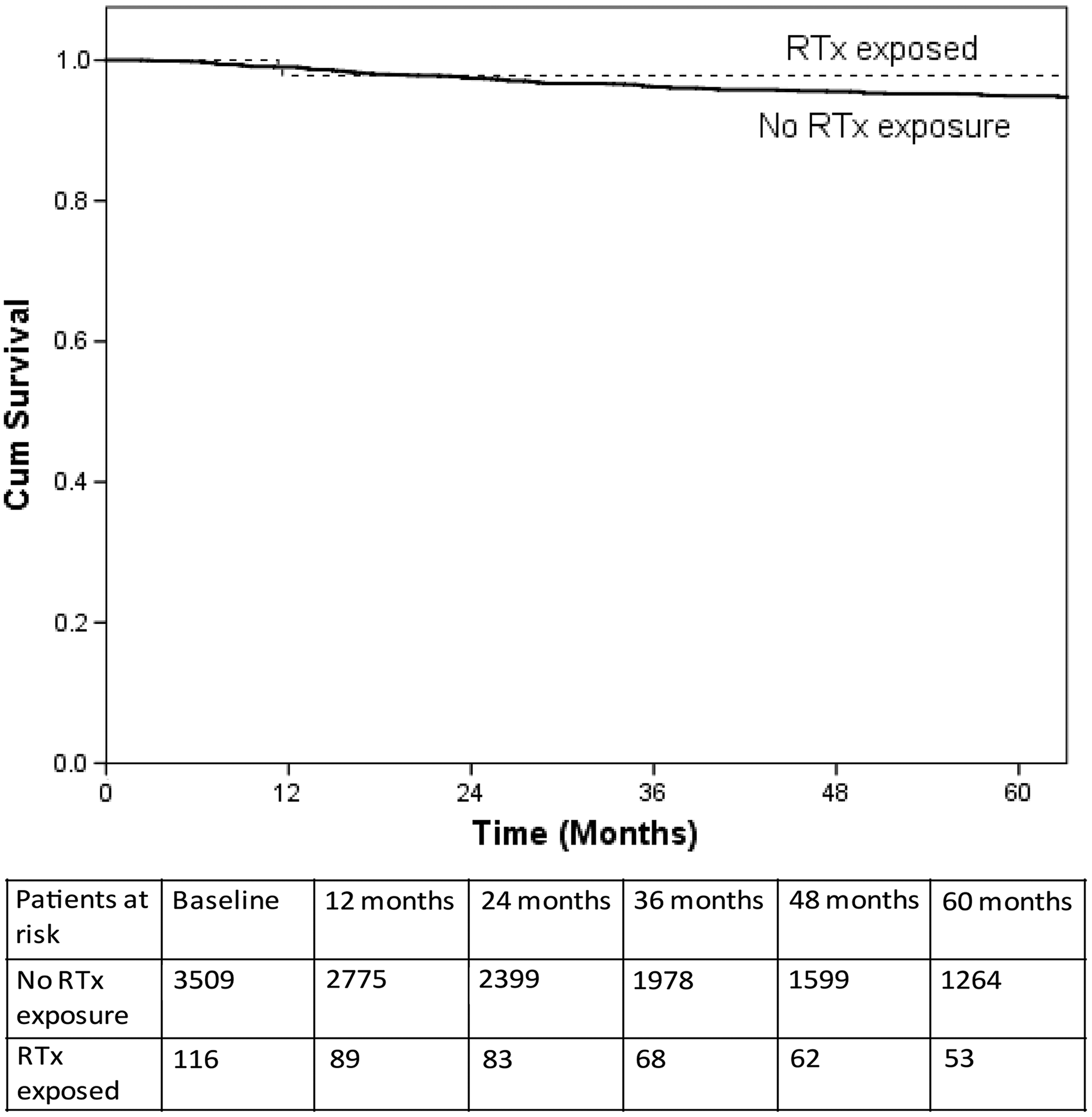
Kaplan–Meier graph for five-year recurrence-free survival.
HR, hazard ratio; CI, confidence interval.
Discussion
There is no consensus as to whether thyroid cancers induced by therapeutic external beam radiation therapy are more aggressive than those arising sporadically. As such, there is controversy as to whether such patients should be treated with more extensive surgery, including elective central compartment neck dissection, and receive adjuvant RAI. The aim of this study was therefore to determine if thyroid cancers in patients with prior exposure to therapeutic radiation had a poorer outcome compared to those who did not. This study provides evidence that outcomes are similar, and it suggests that a history of prior therapeutic radiation exposure should not impact on decision making in the management of patients with differentiated thyroid cancer.
There has been much debate about whether thyroid cancers induced by radiation from nuclear incidents are more aggressive. In the wake of the accident at Chernobyl, radiation exposure was thought to produce more aggressive thyroid cancers. Some groups characterized several markers of aggressive morphology, including solid phenotype, lack of typical architectural differentiation, and limited thyroglobulin content (17 –19). Pacini et al. compared 472 radiation-associated pediatric thyroid cancers in Belarus with 369 non-radiation-induced pediatric thyroid cancers of a similar age at diagnosis in Italy and France. Regional lymph node metastases were seen in 65% of the Belarusian cases, and 8% had distant metastases. Tronko et al. similarly described 241 radiation-associated pediatric thyroid carcinomas in Ukraine. Lymph node involvement was recorded in 62% of these cases, while distant metastases were seen in 17% of the patients. Nodal disease is an adverse prognostic factor for PTC recurrence (20 –22). Thus, the clinical picture supported an aggressive demeanor of these Chernobyl-associated thyroid cancers. However, cumulative evidence now suggests that while radiation exposure contributes to the development of thyroid cancer (1 –3), the prognosis once the disease is treated is no different to sporadic forms (23 –25). In 2006, the World Health Organization (WHO) brought together data from Belarus, Ukraine, and Russia, estimating that there had been in total about 15 deaths attributable to radiation-induced thyroid cancer in a combined cohort of 4837 patients (26). That equates to a disease-specific mortality of only 0.3%. Furthermore, Williams et al. reported that the aggressiveness and morphological features of Chernobyl-related childhood PTC were similar to those not associated with radiation exposure (27). Rumyantsev et al. similarly concluded that the overall presence of nodal disease, frequency of vascular invasion, and multifocal tumors did not differ between both groups (28).
With regards to outcomes from therapeutic radiation exposure, the present results also suggest that outcomes of patients with a history of radiation exposure are not different from that of sporadic forms of the disease. This is supported by several studies that describe the clinical behavior of external radiation therapy–induced thyroid cancers and sporadic PTC of similar histotypes (23 –25). Gow et al. reported on a cohort of eight patients with primary thyroid cancer and 17 patients with thyroid cancer diagnosed after therapeutic radiation for various childhood malignancies. All patients were alive at the time of publication, with a median follow-up 22.6 years after diagnosis of primary malignancy and 3.6 years after the diagnosis of secondary malignancy. The radiation-associated thyroid cancers respond well to therapy, and patients have a good prognosis compared with those with thyroid cancer without radiation history. Shore reports an overall mortality of just 4.6% in such cases (15). In an institutional review of 426 patients who underwent thyroidectomy for malignancy, Furlan et al. report that while ionizing radiation does increase the risk of developing thyroid cancer, it does not increase the adverse course of the disease progression. In their series, the estimated cumulative distant metastases-free survival and local RFS were similar for those with exposure to radiation and those without. They also report no statistical differences for both groups in regards to distant metastases, lymph node involvement, and recurrence rate. Some studies have commented on the higher prevalence of tumor multicentricity in radiation-exposed patients, leading to recommendations of more aggressive surgical resection. However, Furlan et al. and DeGroot et al. both reported similar frequencies of tumor multicentricity in both exposed and unexposed groups (24,29). In the present cohort, it was found that tumor multicentricity was also almost identical among both groups. In those patients with previous radiation therapy, 50.1% (p = 0.985) exhibited multifocal tumors, while 49.9% (p = 0.985) of those patients with no radiation exposure had tumors with multiple lesions. It should be noted that multifocal data were not available for 271 patients in the cohort. The present results and those from these other reports indicate that similar treatment approaches should be recommended for both unexposed patients and those exposed to therapeutic radiation, with an emphasis on continued follow-up to assess for disease recurrence in the long term.
As with most retrospective studies, the present work has its limitations. While it was possible to classify the heterogeneous indications for radiation therapy in this cohort, it was not possible to determine dose or age of exposure. Thus, the cohort with radiation exposure may not be standardized, and may be unrepresentative of the population as a whole. Another point to note is the exclusion of self-reported Chernobyl exposures to ionizing radiation. As expected, the ambiguity of self-reporting threatens to skew the results, as it would not be possible to characterize the dose of radiation received or the proximity to the disaster. However, analysis of these exposures may shed light on the nature of those thyroid cancers directly resulting from a nuclear accident. Lastly, it is possible that with longer follow-up, there may be a difference in recurrence rates between the radiation-exposed and -unexposed cohorts. However, the majority of recurrences in thyroid cancer are detected in the first three years following treatment (30). Therefore, it is unlikely that the results would be different with longer follow-up.
It is concluded that outcomes in terms of both survival and recurrence are similar between radiation-exposed and -unexposed groups. The present data and the literature support the conclusion that therapeutic radiation exposure is not prognostic of outcomes in DTC. Therefore, the extent of surgical and adjuvant treatment should be based on the usual tumor and patient characteristics, irrespective of radiation exposure.
Footnotes
Acknowledgments
This research was funded in part through NIH/NCI Cancer Center Support Grants P30 CA008748.
Author Disclosure Statement
The authors have nothing to declare.