
Abstract
Background:
Iodine deficiency is an important modifier of the risk of thyroid cancer following irradiation. However, little information is available on the prevalence of iodine deficiency in Fukushima and its surroundings after the Fukushima Daiichi nuclear power plant accident that occurred in March 2011.
Methods:
In order to assess urinary iodine concentrations (UIC) and the prevalence of iodine deficiency and to elucidate any associations between demographic characteristics and UIC levels among children and adolescents aged ≤18 years at the time of the accident in Fukushima Prefecture and its surroundings, the data on voluntary UIC testing conducted by Hirata Central Hospital, Fukushima, were evaluated.
Results:
A total of 4410 children and adolescents with a median age of 10 years at examination underwent UIC testing between October 2012 and October 2015. Calculated for all the participants, the median UIC level was 204 μg/L (range 25–21,100 μg/L). There were 133 (3.0%), 732 (16.6%), and 1472 (33.4%) participants with UIC levels of <50, <100, or ≥300 μg/L, respectively. Based on the World Health Organization criteria for nutritional iodine status, no participants were severely iodine deficient (<20 μg/L), but 16.6% of the population were mildly (50–100 μg/L) or moderately (20–50 μg/L) iodine deficient. While no significant difference in UIC was noted between those who did and did not increase dietary iodine intake after the accident (p = 0.93), there were significant differences by year (p < 0.01), school level (p < 0.001), and residential area at the time of the accident (p < 0.001).
Conclusions:
This study demonstrates that the children and adolescents examined had a sufficient amount of iodine during the period 1.5–4.5 years after the nuclear accident. In addition to the differences in the scale and the countermeasures undertaken between the Fukushima and Chernobyl accidents, differences in dietary iodine intake might have played an additional role in resulting in the reportedly different radiation doses to the thyroid between the two nuclear accidents.
Introduction
T
Within these examples, thyroid cancer following nuclear accidents has become a particularly important public health issue. According to UNSCEAR, the 1986 Chernobyl accident has resulted in >6000 cases of thyroid cancer in the three countries of Belarus, Ukraine, and Russia alone, and it is predicted that new cases will continue to develop (9). Thyroid cancer is the only radiation-related cancer effect officially identified by the United Nations (UN) after the Chernobyl nuclear accident (10).
With respect to thyroid cancer following irradiation in the wake of a nuclear accident, age at the time of the accident and radiation exposure dose are known to be major risk factors. However, iodine deficiency can be another important modifier of the risk of thyroid cancer (8,11), since iodine deficiency facilitates the uptake of radioactive iodine by the thyroid, leading to increased radiation doses (12). While poor control of contaminated food products such as milk led to high levels of thyroid radiation exposure after the Chernobyl accident (13), radio-contaminated districts were inland and faced chronic iodine deficiency (14), which has been identified as an additional reason for the post-Chernobyl increase in thyroid cancer in local residents.
On March 11, 2011, the Great East Japan Earthquake and tsunami led to a nuclear accident at Fukushima Daiichi nuclear power plant, resulting in widespread dispersal of radioactive substances, including radioactive iodine, and unintentional radiation exposure among residents (15). The amount of radioactive iodine released after the Fukushima accident is estimated to be one-tenth (approximately 520 PBq) of the amount released by the Chernobyl accident (16), and direct measurements of thyroid exposure doses in children in Fukushima reported a mean dose of 4.2 mSv (17), which was far smaller than the reported levels after the Chernobyl accident, with some children receiving doses as high as 4000 mSv (10). Several studies were published on the childhood thyroid cancer rate in the area following the accident from Fukushima prefectural government and Fukushima medical university (18,19), which have implemented a thyroid ultrasound examination survey of the approximately 360,000 pediatric inhabitants who lived in Fukushima at the time of the accident in October 2011. However, there is little information on the prevalence of iodine deficiency, an important factor in the development of radioiodine-induced thyroid cancer, in Fukushima and its surroundings during the periods spanning the nuclear accident. It is generally accepted that the Japanese population has a sufficient iodine intake due to the high consumption of marine products rich in stable iodine (20). Nevertheless, the dietary patterns of Japanese children, a group susceptible to thyroid radiation exposure, have been changing in recent years due to Westernization and societal changes (21).
Measurement of urinary iodine concentrations (UIC) is a useful way to evaluate the status of dietary iodine intake and iodine deficiency (22,23). While the median UIC is regarded as an excellent biomarker of recent exposure to iodine in populations (24), the World Health Organization (WHO) defines iodine intake as “insufficient” for UIC levels of <100 μg/L, “adequate or more than adequate” for levels of 100–299 μg/L, and “excessive” for levels ≥300 μg/L (25). Hirata Central Hospital, located in Hirata village, Fukushima Prefecture, 40–50 km southwest of the Fukushima Dai-ichi nuclear power plant, has conducted UIC measurements free of charge, with a main focus on evaluating schoolchildren, since October 2012 (Fig. 1). The aims of the present study were twofold: (i) to assess UIC and the prevalence of iodine deficiency in children and adolescents aged ≤18 years at the time of the nuclear accident in Fukushima Prefecture and its surrounding areas affected by the widespread dispersal of radioactive iodine; and (ii) to elucidate any associations between demographic characteristics of the participants and UIC levels.
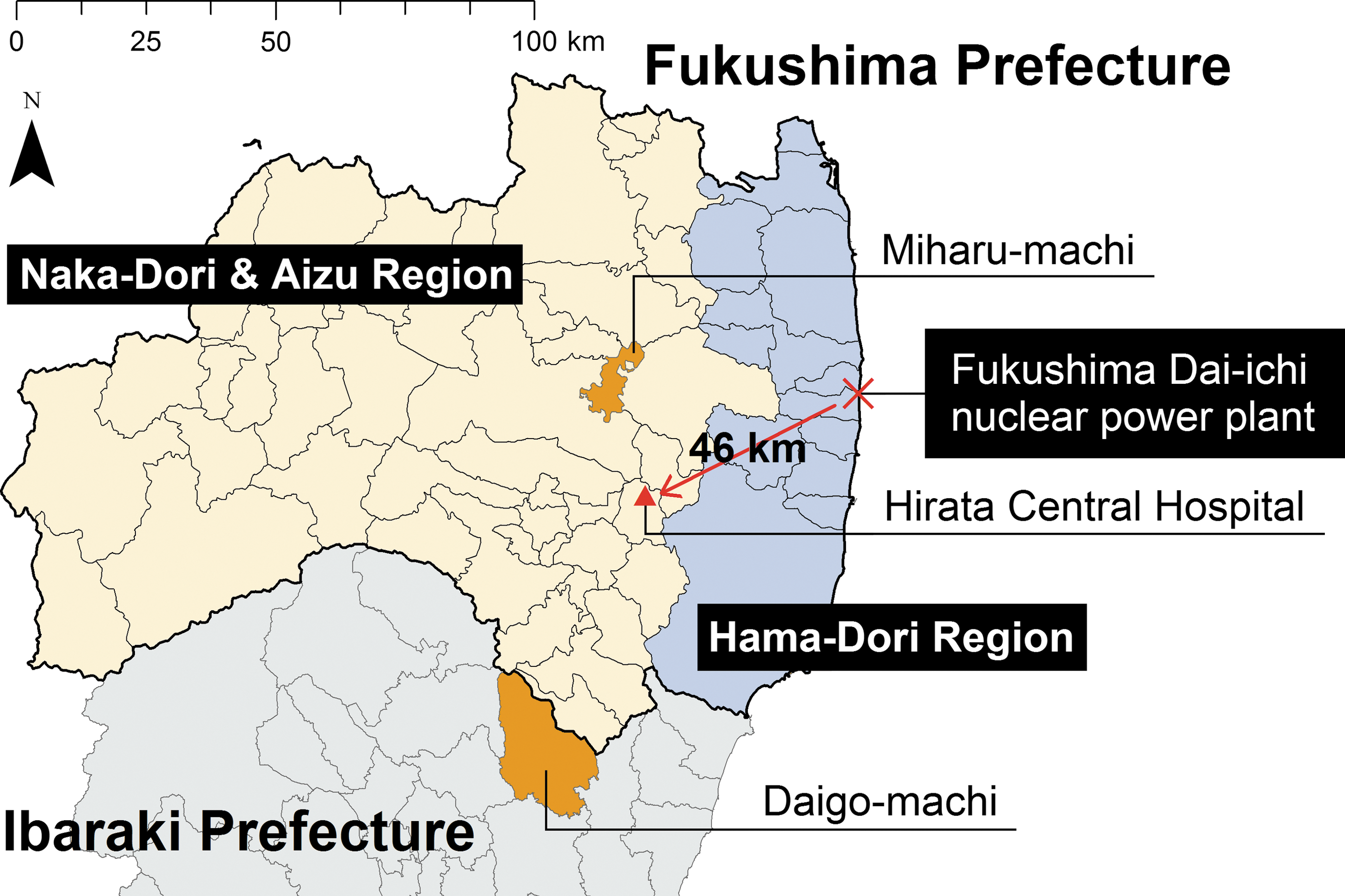
Location of Hirata Central Hospital in relation to the Fukushima Daiichi nuclear power plant. Miharu Town and Daigo Town, which have officially promoted urinary iodine screenings for residents, are highlighted.
Materials and Methods
Data setting and UIC measurement
This study retrospectively assessed the results of all children and adolescents aged ≤18 years who underwent UIC testing at Hirata Central Hospital from 2012 to 2015. Data extracted from screening records included the age of the participant at the examinations, sex, address prior to the accident, whether the address had changed following the accident, UIC levels, and dietary behavior for iodine intake inquired in the questionnaire (see below). For participants who underwent UIC testing on multiple occasions during this period, only the data from the first testing were subjected to analysis. The UIC was determined in the spot urine by the Sandell–Kolthoff reaction utilizing the kit produced by Hitachi Chemical Co., Ltd. (Tokyo, Japan). All urine samples were assayed in duplicate. The sensitivity of the assay was 25 μg/L, and both the inter- and intra-assay coefficients of variation were <10%.
Since October 2012, Hirata Central Hospital has offered voluntary UIC measurements and thyroid ultrasound examinations free of charge for residents of Fukushima and its surrounding areas who were <18 years of age at the time of the accident in March 2011. Local municipalities including Miharu-machi, located in the Nakadori region of Fukushima Prefecture, and Daigo-machi, Ibaraki Prefecture, have facilitated yearly thyroid ultrasound examinations and UIC testing for all primary and secondary school students in these towns. Their geographical locations, relative to the nuclear power plant, are shown in Figure 1. This screening program is publicized online, in general magazines, and newspapers.
Questionnaire about dietary intake of iodine
On the occasion of the UIC testing, to assess potential changes of dietary habits, all participants were questioned about their dietary intake of iodine. All participants answered a yes-or-no question about whether they proactively started to consume foods rich in iodine after the accident.
Analysis
In order to assess any effects of age, sex, pre-accident residential area, and post-accident dietary behavior on UIC levels, the analyses outlined below were performed.
(i) Median UICs were compared between those who proactively increased their dietary iodine intake after the accident and those who did not using a nonparametric Wilcoxon rank-sum test.
(ii) For those who reported no proactive increases in their iodine intake after the accident, differences in UIC by sex, year of test (2012, 2013, 2014, 2015, defined as the government's financial year that runs from April 1 to March 31), school level (preschool, ages ≤6 years; primary school, 6–12 years; secondary school, 12–15 years; and high school, 15–18 years), and residential address at the time of the accident (outside of Fukushima Prefecture, Hamadori, Nakadori, and Aizu) were assessed using the Wilcoxon rank-sum test for sex, and the Kruskal–Wallis test for year of test, age bracket, and residential address at the time of the accident.
(iii) The WHO defines iodine deficiency at the population level as “mild” for UIC levels of 50–100 μg/L, “moderate” for levels of 20–50 μg/L, and “severe” for levels <20 μg/L (26). For the purpose of analyzing the associations between iodine deficiency and characteristics of the participants, it would be preferable to divide the participants with UIC levels of <100 μg/L into three groups. However, only a small number of participants were found to have “moderate” or “severe” iodine deficiency (see Results), which would have diminished the statistical power of the analyses. Thus, the participants were classified into two dichotomous groups: <100 μg/L or ≥100 μg/L. Next, a multiple logistic regression model was constructed to identify factors associated with UIC levels of <100 μg/L. To minimize potentially unobserved cofounding effects of evacuation on iodine intake via changed lifestyles in evacuation sites, those reporting post-accident address changes were excluded from the logistic regression.
All analyses were carried out with STATA/MP v13.1 (Stata Corp, College Station, TX). p-Values of <0.05 were considered as significant.
Ethics
This study was approved by the Hirata Central Hospital Internal Review Board (20160316-2). Informed consent was received from all subjects, or their guardians, participating in this study.
Results
From October 2012 to October 2015, a total of 4410 children and adolescents aged ≤18 years at the time of the accident underwent UIC testing. The age range of participants was 1–18 years old (median 10 years), and 2139 (48.5%) of them were female (Table 1). The numbers of primary and secondary school students in Miharu and Daigo were 1423 and 1155, respectively. The total number of primary and secondary school students were 1379 in Miharu for fiscal year 2013, and 1113 in Daigo for fiscal year 2014, and 1221 (88.5%) and 1118 (99.6%) of these participated in this UIC testing in the corresponding fiscal years, respectively.
Percentage in row.
Percentage in column.
Wilcoxon rank-sum test.
Chi-square test.
Figure 2 displays the distribution of UIC levels in individual participants. The levels ranged between 25 and 21,100 μg/L, with a median of 204 μg/L. Fifty percent (n = 2206) fell within the normal range (100–299 μg/L) as per the WHO definition, and there were 133 (3.0%), 732 (16.6%), and 1472 (33.4%) participants with UIC levels of <50, <100, or ≥300 μg/L, respectively. No participants were below the threshold of severe iodine deficiency (<20 μg/L).
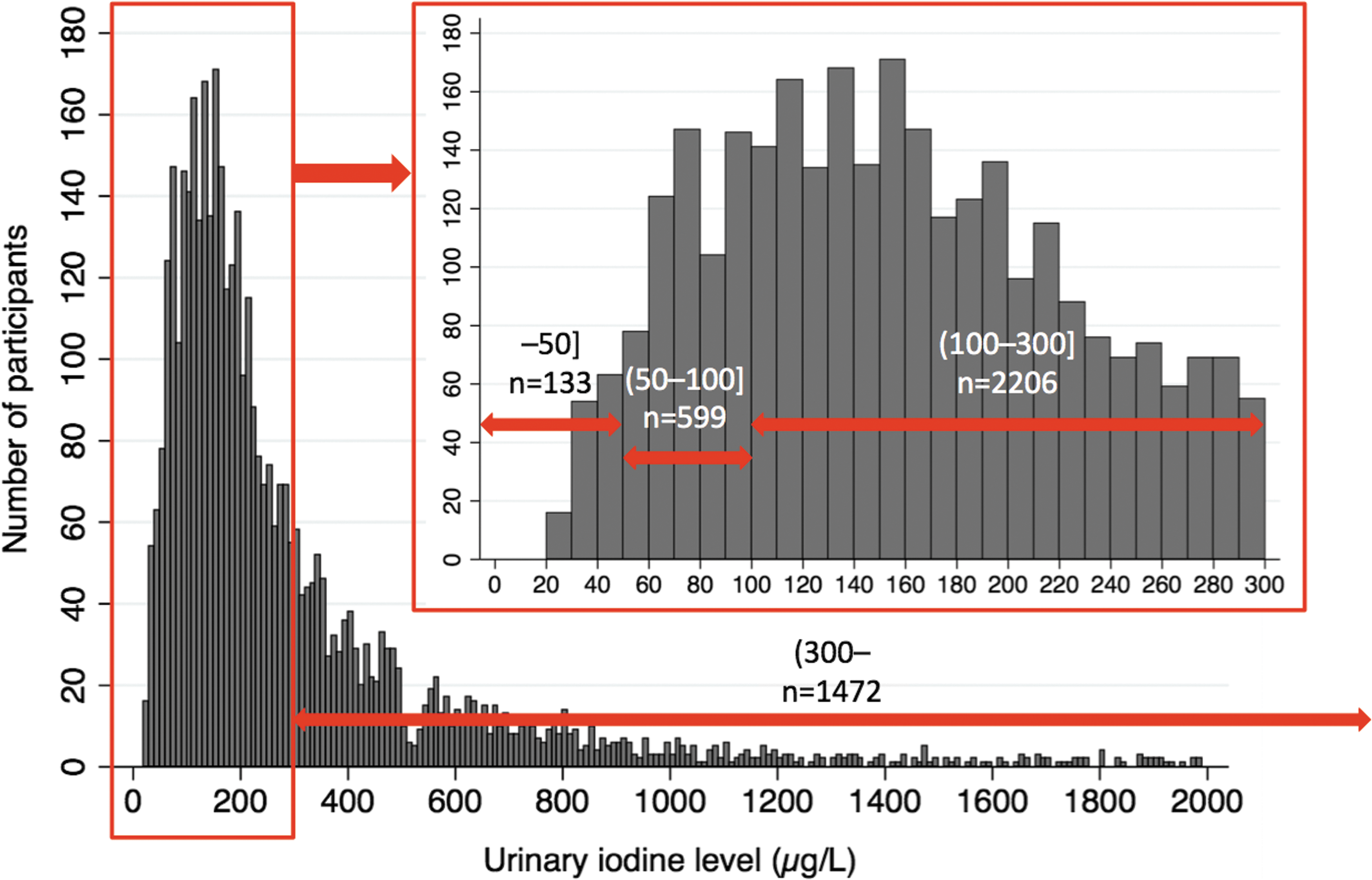
The results of urinary iodine screenings, and concentration distributions for all participants. No participants had severe iodine deficiency (urinary iodine concentrations <20 μg/L).
Analysis 1
In answer to the question of whether participants increased their iodine intake, 617 (14.0%) reported a proactive increase after the accident (Table 1). There were significant differences across the years of examinations in the proportions of participants who proactively increased iodine intake (p < 0.001), with the largest value being observed in 2012 (40.3%), after which it decreased year after year (7.7–20.1%). Among those who reported proactive increases in dietary iodine after the accident, few had been living outside of Fukushima at the time of the accident (6.0%), and comparatively large proportions had been living in Fukushima's Hamadori and Nakadori + Aizu regions (18.8% and 17.7%, respectively; p < 0.001). As there was a small number of test participants from the Aizu region (n = 13), the data from the Nakadori + Aizu regions were combined for analyses. There were no statistically significant differences in sex and school level between those who did and did not proactively increase iodine intake after the accident. Furthermore, there was no significant difference in UIC levels between those who did and did not proactively increase iodine intake after the accident (median 202.5 vs. 213.0; p = 0.93).
Analysis 2
In the group reporting no post-accident increase in dietary iodine, no significant differences were found in UIC levels by sex. However, there were significant differences by year (p < 0.01), school level (p < 0.001), and residential area at the time of the accident (p < 0.001; Table 2).
Analysis 3
Table 3 presents the results of the logistic regression analysis. The covariates included in the final model are school model (categorical: preschool [reference], primary school, secondary school, and high school), sex (binary: male [reference] and female), and pre-disaster residential area (categorical: outside of Fukushima [reference], Hamadori, and Nakadori + Aizu). Compared with primary school students, there was a significantly higher proportion of UIC levels <100 μg/L in preschool and secondary school students (odds ratio [OR] 1.92 [confidence interval (CI) 1.45–2.53], p < 0.001; and OR 1.45 [CI 1.16–1.81], p < 0.01). Furthermore, compared with those living outside of Fukushima, residency in Hamadori was associated with a significantly higher proportion of UIC levels <100 μg/L (OR 1.50 [CI 1.04–2.17], p < 0.05).
CI, confidence interval.
Discussion
The present study found that the children and adolescents in Fukushima and its neighboring areas had been taking sufficient amounts of dietary iodine during the period 1.5–4.5 years after the Fukushima nuclear power plant accident. The median level of UIC among all of the participants was 204 μg/L, well above the lower end of adequate iodine intake as per the WHO recommendations (100 μg/L).
The UIC was <100 μg/L in only 16.6% of the participants, and there were no subjects with a UIC <20 μg/L. The WHO recommends that the proportion of individuals with a UIC <50 μg/L should be <20% in a given population (26), and in the present study, the proportion of participants falling under this subcategory was as low as 3.0%. Overall, there were extremely few participants found to be severely iodine deficient, and most participants can be regarded as having ingested sufficient amounts of iodine with their daily diets during the years spanning 2012–2015. The findings in the present study are comparable with the results of urinary iodine screening reported in previous studies involving Japanese schoolchildren (25,27).
Furthermore, this study found no statistically significant differences in UIC between those who did and did not increase their dietary iodine intake after the accident. The present study revealed that 14.0% of the participants increased their dietary intake of iodine after the accident. While the reason for this behavior is not clear, radiation-related fear may have played a role, similar to what was reported after the Chernobyl accident (28). However, it is assumed that fear of radiation diminished year after year, since the proportion of participants reporting proactive increases of iodine intake decreased year after year. A previous study found that a higher proportion (23.1%) of children and adolescents in Fukushima increased their intake of seaweed during the period 20–30 months after the accident compared with this study, which may be an observation suggesting a declining fear for radiation over time (29). Collectively, the present findings indicating a lack of significant changes in UIC, irrespective of the altered dietary behaviors after the accident, may suggest that the participants in this study had already ingested sufficient amounts of iodine before the nuclear accident.
However, caution should be used in interpreting the UIC data by year of examination, group, and residential areas in this study. While no significant sex-dependent differences in UIC were found in Analysis 2, there were significant differences with respect to year, school level, and residential area at the time of the accident. Results of the multivariate analysis (Analysis 3) indicate that compared with primary school students, preschool and secondary school students were at a higher risk of iodine deficiency (<100 μg/L; Table 3). The same trend could be seen in the residents of the Hamadori region in Fukushima compared with the residents outside of Fukushima (Table 3). While the reason for these trends is unclear, there are some potential factors. For the variable of year, it is worth noting that this study began and ended in October, meaning that only such data that were obtained between October through January for years 2012 and 2015 were available due to the data organization based on the Japanese fiscal year, which runs from April to March. This might have caused seasonal confounding with respect to the variable of year, resulting in the observed significant differences in Analysis 2. However, these differences across the years of examination disappeared when tested by multivariate analyses (Analysis 3). The finding of a lower UIC in Hamadori, the coastal region of Fukushima, may be caused by the post-accident changes in dietary iodine supply due to restrictions placed on fishing. Most of the data from outside of Fukushima came from residents of Daigo, Ibaraki Prefecture, where a radiation leak accident occurred in 2013 (30). It is possible that this nuclear accident urged the population in Daigo to increase their iodine intake for prevention purposes for several years, which may have resulted in the significant differences in UIC between the residential areas examined. This may have led to the overestimation of odds ratios in the Hamadori and Nakadori + Aizu districts. The observed differences in UIC between the various age brackets and regions might reflect differences in ingredients used for school meals, and/or differing food customs by region and age. Children younger than school age are the most susceptible group to radioactive iodine exposure, and therefore the lower UIC levels detected in this subgroup may merit further investigations including nutritional surveys.
It is not possible to conclude from the present findings alone that children and adolescents in Fukushima and its surrounding areas were not iodine deficient as a whole during the periods spanning both the pre-accident and early post-accident periods after the release of radioactive iodine from the damaged nuclear power plant. Given the post-accident restrictions placed on planting and shipping farmed and fished products, it is likely that there were changes in societal dietary habits (31,32), and therefore it may be incorrect to assume that post-accident UIC levels represent pre-accident levels. During the period of social disruption that occurred immediately after the nuclear accident, there was a loss of crucial supplies such as electricity, gas, and water, and many evacuees may have been forced to change their life-styles, including sole reliance on foods rationed out at evacuation centers, a factor beyond their control (33). Further research should place more attention on possible changes in dietary habits before and after the accident, and on dietary patterns of evacuees.
Direct measurements of thyroid radiation exposure after the Fukushima nuclear accident were reported to be overwhelmingly smaller than those after the Chernobyl accident (17). While this difference may be explained by various factors, one is the reported difference in the released amount of radioiodine between Chernobyl and Fukushima, with the latter being one-tenth of that of the former (16). Another factor may be the rapid evacuation and restrictions placed on the shipping and circulation of contaminated food products implemented by the Japanese government, which may have helped substantially to mitigate radiation exposure to the thyroid (34). In addition to these two reasons, the present study suggests that the overall sufficient intake of stable iodine in Fukushima residents may have prevented the thyroid from being exposed to radioactive iodine.
This study provides several useful implications that reach above and beyond the role of radiation exposure on thyroid cancer in after the Fukushima accident. First, while most participants were found to have a sufficient intake of iodine, a minor proportion of them fell within the category of mild (50–100 μg/L) or moderate (20–50 μg/L) iodine deficiency. In comparison to the group with sufficient iodine levels, the slightly deficient group may have a higher risk of developing thyroid cancer. Even so, in the previous reports of the WHO and UN on the environmental radiation in Fukushima, the role of dietary iodine intake was not taken into account in dose estimations of thyroid radiation exposure in affected residents (35,36). In order to have a better understanding of the actual radioiodine doses to the thyroid after the nuclear accident, it would be preferable to incorporate the stable iodine intake into analyses. The results of the present study may hopefully be a basis for future investigations addressing this aspect. Second, in marked contrast to iodine deficiency, excess iodine intake may also raise the risk of thyroid cancer, unrelated to radiation exposure (37). While the WHO defines UIC levels of ≥300 μg/L as excessive (24), 33.4% of the participants in this study were found to have very high levels of UIC. When assessing the risk of thyroid cancer in young individuals exposed to the Fukushima accident, it may be necessary to consider the possible effect of excessive iodine intake on thyroid cancer risk as well, rather than limiting the focus on radiation exposure.
Limitations
There are several limitations to this study. First, the urinary iodine screening was conducted on a voluntary basis, and thus the data obtained may not be representative of all areas of Fukushima Prefecture. Second, the UIC measurement is known as a test prone to a large day-to-day variation in a given individual (38).
Conclusion
The present study found subtle but statistically significant differences in the UIC among participants with respect to the year of examination following the Fukushima accident, subject age, and residential area. As a whole, the children and adolescents examined in this study had ingested sufficient amounts. In addition to the differences in the scale of the accident and countermeasures undertaken between Fukushima and Chernobyl, differences in dietary iodine intake might have played an additional role for the reportedly different radiation doses to the thyroid between the two nuclear accidents.
Footnotes
Acknowledgments
We would like to thank Fumihiko Sagawa (Director of Healthcare Corporation Seireikai), Masahiko Nihei, Yu Sakuma at Hirata Central Hospital, Megumi Murakami, and Miki Abe at the Hirata Radiation Research Center. We are also greatly appreciative of the staff working for the municipalities, especially those of Miharu Town and Daigo Town. The study could not have taken place without their assistance. We additionally thank all people who made donations for the administration of the thyroid screening program at Hirata Central Hospital, especially Cataloghouse, Inc.
Author Disclosure Statement
Nothing to declare.