
Abstract
Background:
Medullary thyroid carcinomas (MTCs) complicated by ectopic Cushing's syndrome (CS) have a poor prognosis, partially due to the difficulty in controlling hypercortisolism by adrenal blocking drugs. Recent reports (including the initial follow-up of this patient) have suggested that tyrosine kinase inhibitors (TKIs) may be a therapeutic option due to an anti-secretory action on ACTH. However, there is a lack of long-term follow-up studies.
Patient Findings:
The case is reported of a 58-year-old man with MTC-related CS resistant to a combination of several anti-cortisolic drugs. Vandetanib, an oral multi-TKI that targets RET in particular, was initiated, and a rapid reversal of the hypercortisolism was observed without any change in tumor size. Vandetanib was briefly interrupted twice, once for 45 days because of side effects and a second time for 10 days to schedule surgical debulking. Each time, plasma cortisol and calcitonin levels increased after TKI withdrawal and were rapidly lowered by vandetanib reintroduction. As described in other cases of CS caused by MTC, a marked ACTH increase after desmopressin stimulation was observed before vandetanib therapy. In contrast, a blunted ACTH response to desmopressin was documented throughout the course of vandetanib treatment. This modulation of the tumoral ACTH production is a strong argument in favor of a TKI anti-secretory action. A left thyroid lobectomy and a modified neck dissection were performed one year after the initiation of vandetanib in order to reduce the tumor mass. An activating M918T RET (c.2753T>C) somatic mutation was identified in a lymph node metastasis.
Conclusion:
Three years and eight months after vandetanib initiation, there was no sign of recurrence of hypercortisolism. This case illustrates the long-term effectiveness of vandetanib in maintaining the control of hypercortisolism in MTC-related CS.
Introduction
M
Case Report
A 58-year-old man was hospitalized for diarrhea, muscle weakness, and a melancholic depression. A diagnosis of metastatic MTC was made with common sites of metastasis: cervical and mediastinal lymph nodes, the lung, liver, and bone. The initial plasma calcitonin level was 6900 ng/L (normal <10 ng/L). There was no family history of MTC, and the RET proto-oncogene germline mutation screening was negative. The clinical presentation led to the diagnosis of an associated ACTH-dependent CS. Dynamic tests were concordant with paraneoplastic CS: absence of ACTH response to CRH stimulation and unsuppressed cortisol after a high dose of dexamethasone. The desmopressin test resulted in a marked ACTH increase, as can be observed in ectopic CS (Fig. 1A and B).
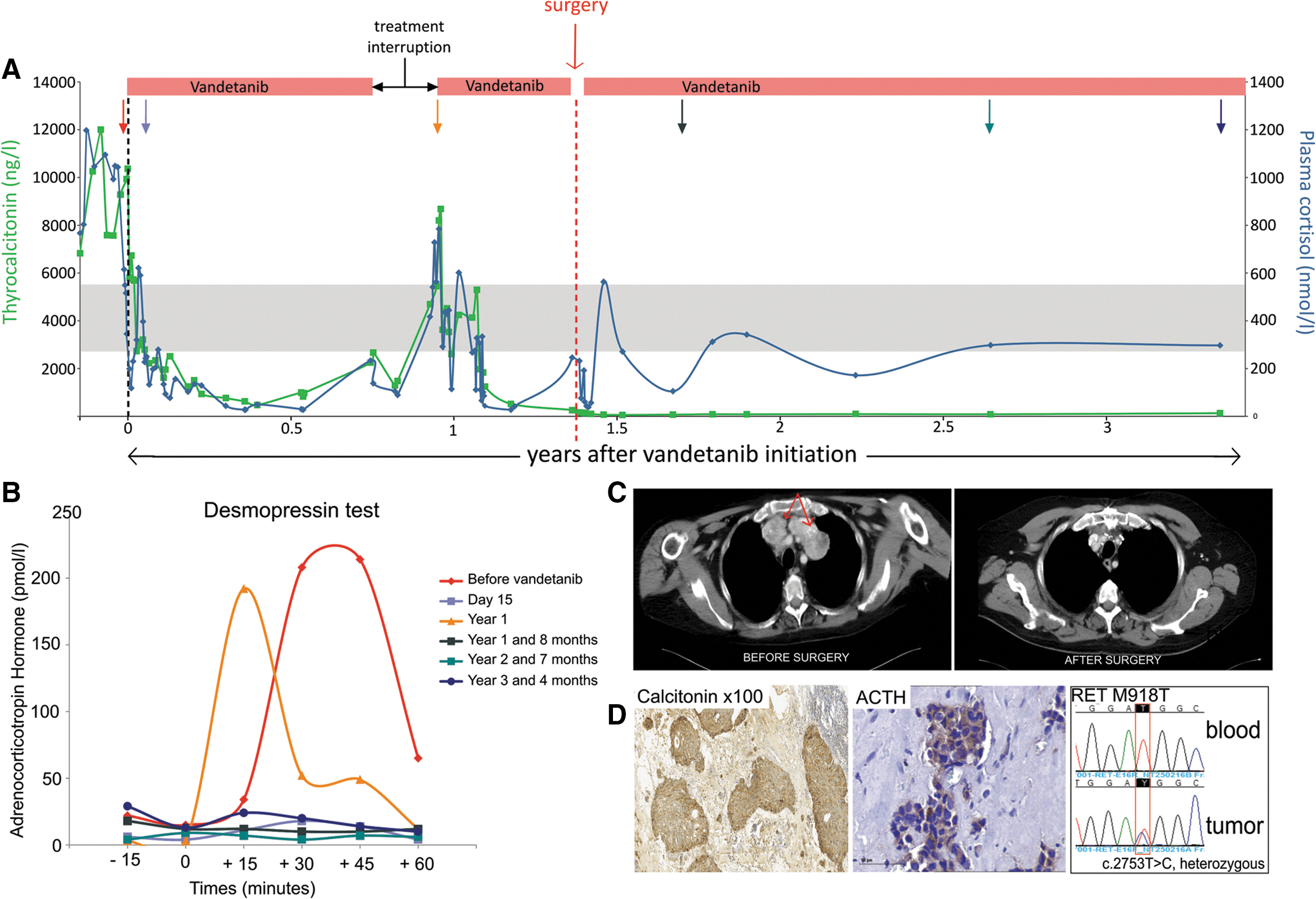
Prolonged control of hypercortisolism by vandetanib in a medullary thyroid carcinoma harboring a M918T RET mutation. (
A sequential combination therapy with four anti-cortisolic drugs (metyrapone, mitotane, somatostatin analogues, and ketoconazole) had proved ineffective to normalize plasma cortisol (Fig. 1A). As previously reported (initial follow-up of 2.5 months), vandetanib was then initiated (300 mg once daily) (2). A rapid reduction of plasma cortisol and calcitonin was observed within a few days, independently of any antitumor effect. The disappearance of the ACTH stimulation by desmopressin under vandetanib suggested an anti-secretory action on ACTH. Cortisol substitution therapy was necessary to compensate for the secondary adrenal insufficiency.
The subsequent follow-up allowed further insight to be gained into the cortisol-lowering mechanism of action of vandetanib. The TKI was interrupted once after 10 months of treatment due to the apparition of seizures with no obvious etiology. A rapid rise of serum cortisol and calcitonin levels was observed, and for the second time, a marked ACTH response to desmopressin was documented (Fig. 1A and B). As a consequence, therapy with vandetanib was resumed and resulted again in a rapid lowering of cortisol and calcitonin levels. The reversible suppressive action of vandetanib on ACTH secretion (documented by several desmopressin tests throughout the follow-up; Fig. 1B) and stable disease without any tumor reduction after 17 months of TKI treatment led to surgical debulking being planned. Vandetanib was interrupted a second time, one week before and after the surgery. A neck dissection combined with a sternotomy was performed to remove the cervical and mediastinal lymph node metastases (Fig. 1C). Because the disease was already known to be metastatic, the thyroid surgery was limited to a left lobectomy (because of a suspicious nodule on ultrasound) to preserve thyroid function and avoid hypoparathyroidism, which could have complicated the vandetanib therapy. Pathological examination confirmed metastatic disease to the lymph nodes with positive immunostaining for calcitonin and ACTH (Fig. 1D). A primary MTC could not be identified in the left thyroid lobe (the nodule was an adenoma). As the remaining lobe was free of suspicious cytological findings, the possibility of a MTC arising from ectopic thyroid tissue could not be ruled out. Moreover, next-generation sequencing revealed a RET somatic mutation in one mediastinal lymph node metastasis. A c.2753T>C RET mutation has been identified in the tumor DNA (mutant allele frequency of 44%) and was not found in the germline. This mutation (p.M918T) is the most frequent RET mutation in sporadic MTCs (95%; Fig. 1D) (3).
In the perioperative period, cortisol levels began to increase again. Vandetanib was resumed, and until the time of publication, it has remained effective in controlling hypercortisolism and calcitonin levels (Fig. 1A). The patient has now been on vandetanib therapy for three years and eight months without noticeable lesions and with good control of the calcitonin levels at 132 ng/L.
Discussion
MTC-related Cushing's syndrome is difficult to manage, as hypercortisolism is usually resistant to cortisol-lowering drugs. In addition to the present case, reversal of CS in MTC by vandetanib has been reported in two other cases (4,5). The first case was a 17-year-old boy with multiple endocrine neoplasia type 2B due to a germline M918T RET mutation. He had metastatic MTC complicated by ectopic CS. Vandetanib was effective in controlling hypercortisolism one month after initiation of therapy and during the next 26 months when the TKI was discontinued due to tumor progression (4). The second case was a 37-year-old woman with a sporadic MTC (with unknown somatic RET mutational status). Reversal of the CS was documented one month after initiation of vandetanib therapy. The biochemical response was still present at the time of the publication (eight months) (5). In these three cases, cortisol and calcitonin levels decreased rapidly on vandetanib, and independently of any tumor mass reduction. This rapid anti-secretory effect, which is dissociated from a tumor-reducing effect, reinforces the hypothesis of an anti-secretory action on ACTH by vandetanib on MTC cells. A possible explanation could be a direct inhibition of RET by vandetanib. RET was mutated in at least two of the three cases. Sporadic MTC is characterized by the presence of a somatic RET mutation in 41% of cases (3). Ectopic CS is very uncommon in MTC, suggesting additional molecular alterations leading to aberrant ACTH expression. The anti-secretory effect of vandetanib in MTC-related CS suggests that under certain circumstances, RET (or other targets of the TKI) may drive ACTH secretion. This kind of regulation has been demonstrated in vitro between oncogenic RET and calcitonin secretion, after RET kinase inhibition (6). The RET kinase seems to control signaling pathways, which regulate peptide secretion. Moreover, this effect seems to be reversible, as suggested by the rapid increase of cortisol and calcitonin after vandetanib withdrawal. The present case is the first report of prolonged control (three years and eight months at the time of this publication) of MTC-related CS by vandetanib, without secondary resistance. Resistance occurring during vandetanib therapy has been described; one reported mechanism seems to consist in the acquisition of a secondary RET mutation at codon 804 (7).
Two other TKIs have been used for the therapy of paraneoplastic CS associated with MTC. Sorafenib has been demonstrated to reverse hypercortisolism in seven days in a sporadic MTC (somatic RET mutational status unknown) for a period of 15 months until tumor progression (8). One hypothesis offered by the authors is a decrease of ACTH synthesis by inhibition of the MAPK pathway due to targeting of BRAF by sorafenib. The suppressive effect of sorafenib on ACTH and cortisol secretion was also reversible after discontinuation of sorafenib (8). Sunitib has also been shown to control MTC-associated CS, with a short follow-up of five months (9).
Another interesting aspect of the present case is the absence of MTC in the thyroid on pathological examination. Perhaps an ectopic MTC could be the explanation, as previously suggested in another case associated with CS (10).
In conclusion, the present case demonstrates that vandetanib may be a potent therapeutic tool for long-term control of CS associated with some MTC.
Footnotes
Acknowledgments
We thank Nirubiah Thuraiajasingam for technical assistance with searching RET mutation.
Author Disclosure Statement
The authors have nothing to disclose.