
Abstract
Background:
Thyroid-related mortality has remained constant despite the increasing incidence of thyroid carcinoma. Most thyroid nodules are benign; therefore, ultrasound and fine needle aspiration (FNA) are integral in cancer screening. We hypothesize that increased nodule size at ultrasound does not predict malignancy and correlation between nodule size at ultrasound and pathologic exam is good.
Methods:
Resected thyroids with preoperative ultrasounds were identified. Nodule size at ultrasound, FNA diagnosis by Bethesda category, size at pathologic examination, and final histologic diagnosis were recorded. Nodule characteristics at ultrasound and FNA diagnoses were correlated with gross characteristics and histologic diagnoses. Nodules for which correlation could not be established were excluded.
Results:
Of 1003 nodules from 659 patients, 26% were malignant. Nodules <2 cm had the highest malignancy rate (∼30%). Risk was similar (∼20%) for nodules ≥2 cm. Of the 548 subject to FNA, 38% were malignant. Decreasing malignancy rates were observed with increasing size (57% for nodules <1 cm to 20% for nodules >6 cm). At ultrasound size cutoffs of 2, 3, 4, and 5 cm, smaller nodules had higher malignancy rates than larger nodules. Of the 455 not subject to FNA, 11% were malignant. Ultrasound size alone is a poor predictor of malignancy, but a relatively good predictor of final pathologic size (R 2 = 0.748), with less correlation at larger sizes. In nodules subject to FNA, false negative diagnoses were highest (6–8%) in nodules 3–6 cm, mostly due to encapsulated follicular variant of papillary carcinoma.
Conclusions:
Thyroid nodule size is inversely related to malignancy risk, as larger nodules have lower malignancy rates. However, the relationship of size to malignancy varies by FNA status. All nodules (regardless of FNA status) demonstrate a risk trough at ≥2 cm. Nodules subject to FNA show step-wise decline in malignancy rates by size, demonstrating that size alone should not be considered as an independent risk factor. Size at ultrasound shows relatively good correlation with final pathologic size. False negative rates are low in this series. Lesions with the appropriate constellation of clinical and radiographic findings should undergo FNA regardless of size. Both size and FNA diagnosis should influence the clinical decision-making process.
Introduction
A
At ultrasound, thyroid nodules characterized by marked hypoechogenicity compared with background thyroid, microcalcifications, and irregular margins are considered at increased risk of malignancy (4). As these features may be subject to decreased interobserver reproducibility, some authors have suggested nodule size as a more reliable predictor of malignancy (5 –7). Banks et al. developed a predictor model using nodule size, patient age, and FNA cytology to predict malignancy (8). Recent studies, however, have shown conflicting results as to whether nodule size may be used to distinguish at-risk lesions. Kamran et al. observed a 10.5% risk of malignancy in nodules sized 1.0–1.9 cm and a 15% risk in nodules >2 cm with no graded increase in risk in nodules >2 cm, suggesting a size-risk cutoff (7). Shrethsa et al. found no statistically significant difference in the rate of malignancy when thyroid nodules were stratified by size into three groups 0.5–0.9 cm, 1.0–3.9 cm, and ≥4 cm (9). In contrast, others have suggested lobectomy for nodules ≥4 cm given a malignancy rate of 22%, a rate that would otherwise justify at least partial thyroidectomy in a nodule diagnosed as suspicious for follicular neoplasm at FNA (3,10). Surgeons face the added dilemma of a potential false negative benign FNA biopsy in large thyroid nodules. Some authors argue that nodules >4 cm should be resected despite benign cytology given false negative FNA rates exceeding 10% in some institutions (11 –14). Finally, the question of thyroid nodule size and malignancy risk may also be complicated by poor correlation between nodule size at sonographic and pathologic examination, particularly for nodules larger than 1.5 cm, although few studies have examined this relationship (15).
Given the lack of studies correlating sonographic and histologic nodule size and conflicting data regarding nodule size and malignancy risk, we attempt to determine whether nodule size predicts thyroid malignancy, to study the relationship between nodule size at sonographic and pathologic exam, and to examine accuracy of FNA diagnosis by size.
Materials and Methods
Approval for this study was obtained from The University of Chicago Medical Center Institutional Review Board. We searched the pathology archives for all thyroid resection specimens between 2011 and 2013. In addition, the electronic medical record was manually reviewed for an associated sonographic examination as well as demographic information. The size at ultrasound, FNA diagnosis by Bethesda category, size at pathologic examination, and final histologic diagnosis were recorded for each nodule.
In patients with multiple nodules, each lesion was considered separately when definitive size and site correlation could be established. To ensure correct correlation, nodule site, size, and characteristics at ultrasound were matched with nodule site and size within the gross description at resection. Correlation between FNA and final diagnosis were used when applicable. Nodules for which definitive correlation could not be established were excluded. All cases diagnosed as follicular variant of papillary thyroid carcinoma at resection were reviewed by two pathologists (N.A.C., T.A.) in light of new diagnostic criteria for noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFT-P), and were reclassified if criteria were met (16).
The proportion of benign and malignant nodules by size categories (≤0.9 cm, 1–1.9 cm, 2–2.9 cm, 3–3.9 cm, 4–4.9 cm, 5–5.9 cm, and >6 cm) and by size cutoffs (<2 vs. ≥2 cm, <3 vs. ≥3 cm, <4 vs. ≥4 cm, and <5 vs. ≥5 cm) were compared using chi-squared and Fisher exact tests where appropriate. Receiver operator characteristic (ROC) curves were generated for ultrasound size and malignancy rates at final diagnosis through univariate logistic regression. Linear regression was performed to measure the correlation between ultrasound size and final pathologic size. Rates of malignancy by size were also calculated within each Bethesda category. All statistical analyses were performed using STATA 13 (College Station, TX).
Results
A total of 1003 thyroid nodules from 659 patients were included. All patients underwent partial or total thyroidectomy between 2011 and 2013. All 1003 nodules underwent ultrasound examination including measurement in centimeters, which was indicated in the ultrasound or FNA report. Of these 1003 nodules identified and measured at ultrasound, 548 were subject to FNA and 549 had gross or microscopic sizes indicated in the final pathology report. Patients had a mean of 1.52 nodules, with a mean nodule size of 2.42 cm at ultrasound. Of the 659 patients, 439 (67%) had a solitary nodule and 220 (33%) had multiple nodules: 2 nodules in 148 patients, 3 nodules in 40 patients, 4 nodules in 20 patients, 5 nodules in 8 patients, 6 nodules in 2 patients, and 8 nodules in 2 patients. Patient characteristics are listed in Table 1.
FNA, fine needle aspiration; US, ultrasound.
All nodules (n = 1003)
At final resection, 258 nodules (25.7%) were malignant. Of the malignant lesions, there were 231 (89.5%) papillary thyroid carcinomas, 15 (5.8%) follicular thyroid carcinomas, 5 (1.9%) poorly differentiated carcinomas, 1 (0.4%) anaplastic thyroid carcinoma, 5 (1.9%) medullary thyroid carcinomas, and 1 (0.4%) metastatic carcinoma (Table 2). The majority (81%) of papillary carcinomas measured between 0.1 and 3 cm on ultrasound (average 2.0 cm on ultrasound and 1.9 cm on final), while 86% of follicular carcinomas were between 2 and 5 cm on ultrasound (average 3.2 cm on ultrasound and 3.0 cm on final). Rates of malignancy by size groups were 31.9% (≤0.9 cm), 31.3% (1–1.9 cm), 21.3% (2–2.9 cm), 19.9% (3–3.9 cm), 20% (4–4.9 cm), 21.1% (5–5.9 cm), and 15.6% (>6 cm) (Table 3). Nodules ≤0.9 cm were used as the reference for calculation of the odds ratio. Nodules <2 cm had the highest rate of malignancy (∼30%). Rates were similar (∼20%) for nodules ≥2 cm (Fig. 1). Risk of malignancy using ultrasound size cutoffs of 2, 3, 4, and 5 cm was analyzed for this group of nodules. Larger nodules (≥2 cm, ≥3 cm, ≥4 cm) had lower rates of malignancy compared with smaller nodules. No significant difference was observed for nodules <5 cm compared to ≥5 cm (Table 4).
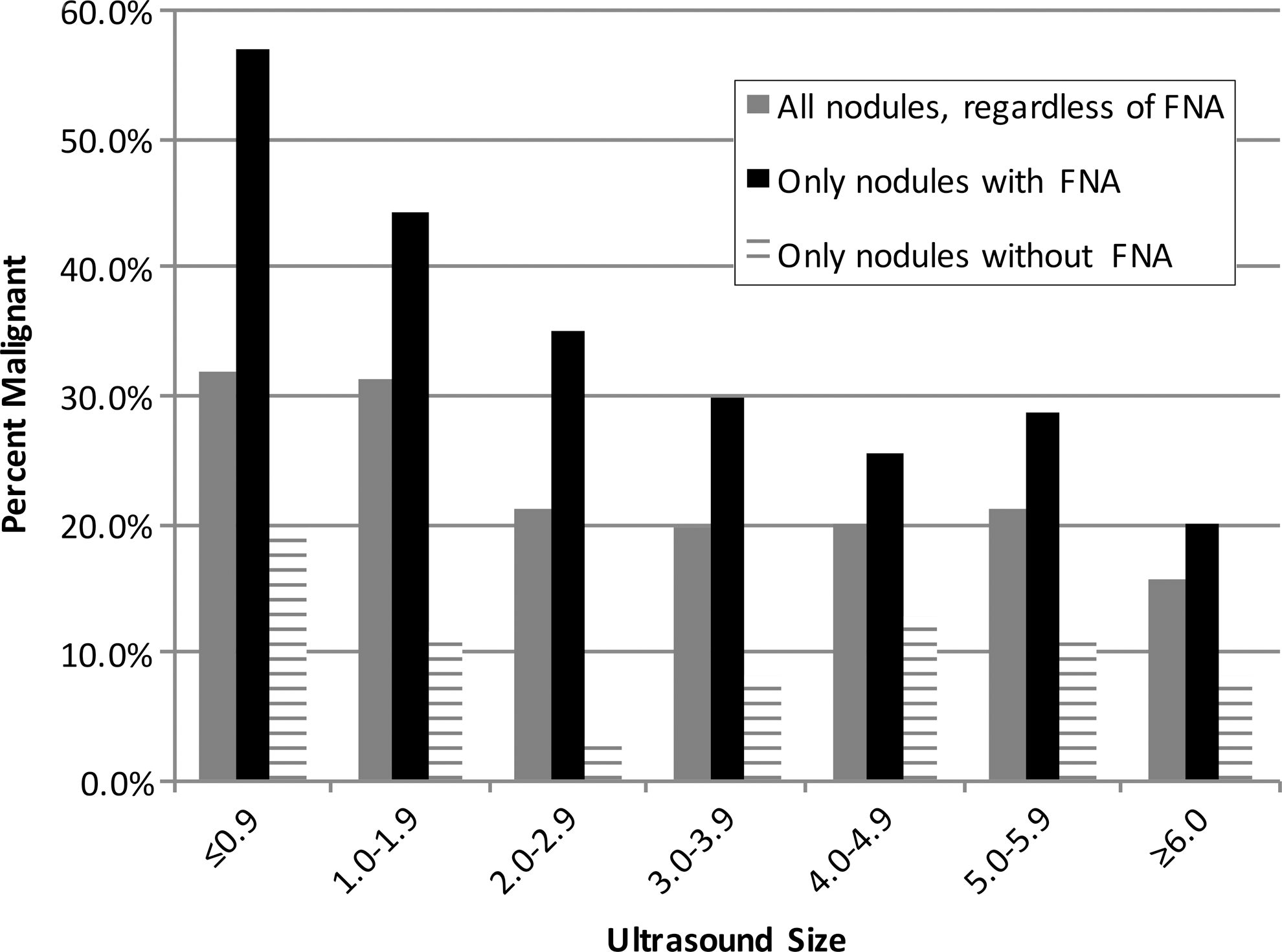
The highest rates of malignancy in each size category are in nodules that have undergone FNA (black bars). Considering all nodules regardless of FNA status, rates of malignancy decrease with increasing size and plateau at approximately 2 cm and above (gray bars). FNA, fine needle aspiration.
ANA, anaplastic thyroid carcinoma; FTC, follicular thyroid carcinoma; MED, medullary thyroid carcinoma; Other, metastatic carcinoma; PDC, poorly differentiated carcinoma; PTC, papillary thyroid carcinoma.
CI, 95% confidence interval; OR, odds ratio.
Nodules with FNA diagnosis (n = 548)
Of the 1003 nodules subject to partial or complete thyroidectomy, 548 underwent cytologic examination by FNA biopsy prior to resection. Of the nodules subject to FNA, 208 (38%) were malignant at final histology. Rates of malignancy by size groups were: 56.8% (≤0.9 cm), 44.3% (1–1.9 cm), 34.9% (2–2.9 cm), 29.7% (3–3.9 cm), 25.5% (4–4.9 cm), 28.6% (5–5.9 cm), and 20% (>6 cm) (Table 5). Of these biopsied nodules, all size categories had an increased rate of malignancy when compared with all 1003 nodules regardless of FNA status (Fig. 1). Analysis by ultrasound size cutoffs revealed lower rates of malignancy in larger nodules (≥2 cm, ≥3 cm, ≥4 cm, ≥5 cm), ranging from 24–31% in larger nodules to 39–47% in smaller nodules (Table 6).
Nodules without FNA diagnosis (n = 455)
Of the remaining 455 nodules subject to ultrasound examination but not fine needle aspiration biopsy, 11% were malignant at final histology. Rates of malignancy by size groups were: 19.8% (≤0.9 cm), 11.5% (1.0–1.9 cm), 3.2% (2.0–2.9 cm), 8.1% (3.0–3.9 cm), 12.8% (4.0–4.9 cm), 11.8% (5.0–5.9 cm), and 8.3% (>6 cm) (Table 7). Of these non-biopsied nodules, all size categories had a decreased rate of malignancy when compared with biopsied nodules and all nodules regardless of FNA status (Fig. 1). Analysis by ultrasound size cutoffs revealed no statistically significant difference between nodules ≥3 cm and <3 cm, ≥4 cm and <4 cm, or ≥5 cm and <5 cm. Nodules <2 cm had twice the risk of malignancy as nodules ≥2 cm (p = 0.0064) (Table 8).
The reasons for lack of FNA biopsy in some large dominant nodules are variable and include (i) a prior FNA biopsy from an outside institution not reviewed by our department; (ii) nodule too calcified for FNA; (iii) history of medical thyroid disease such as Graves’ or Hashimoto's thyroiditis requiring resection regardless; (iv) clinical history of compressive symptoms requiring resection regardless; or (v) other indications for thyroidectomy where the results of an FNA played no role in the decision to remove the thyroid lobe or gland. All 13 “unbiopsied” nodules larger than 3 cm that were malignant on final diagnosis underwent FNA at outside institutions. Because these FNAs were not reviewed by our pathologists, we did not include the FNA results in this dataset. Outside diagnoses were benign (3 cases), follicular lesion of undetermined significance (2 cases), follicular neoplasm (3 cases), suspicious for papillary thyroid carcinoma (PTC; 2 cases), and PTC (3 cases).
Ultrasound size as a predictor of malignancy
Receiver operating characteristic curves were used to determine whether ultrasound size can predict malignancy were generated for all three groups (all nodules, only nodules with FNA, and only nodules without FNA). ROC analysis showed that ultrasound size is a poor predictor of malignancy in all nodules (n = 1003, AUC = 0.577) (Fig. 2), in those that underwent FNA (n = 548, AUC = 0.615), and in those that did not undergo FNA (n = 455, AUC = 0.601).
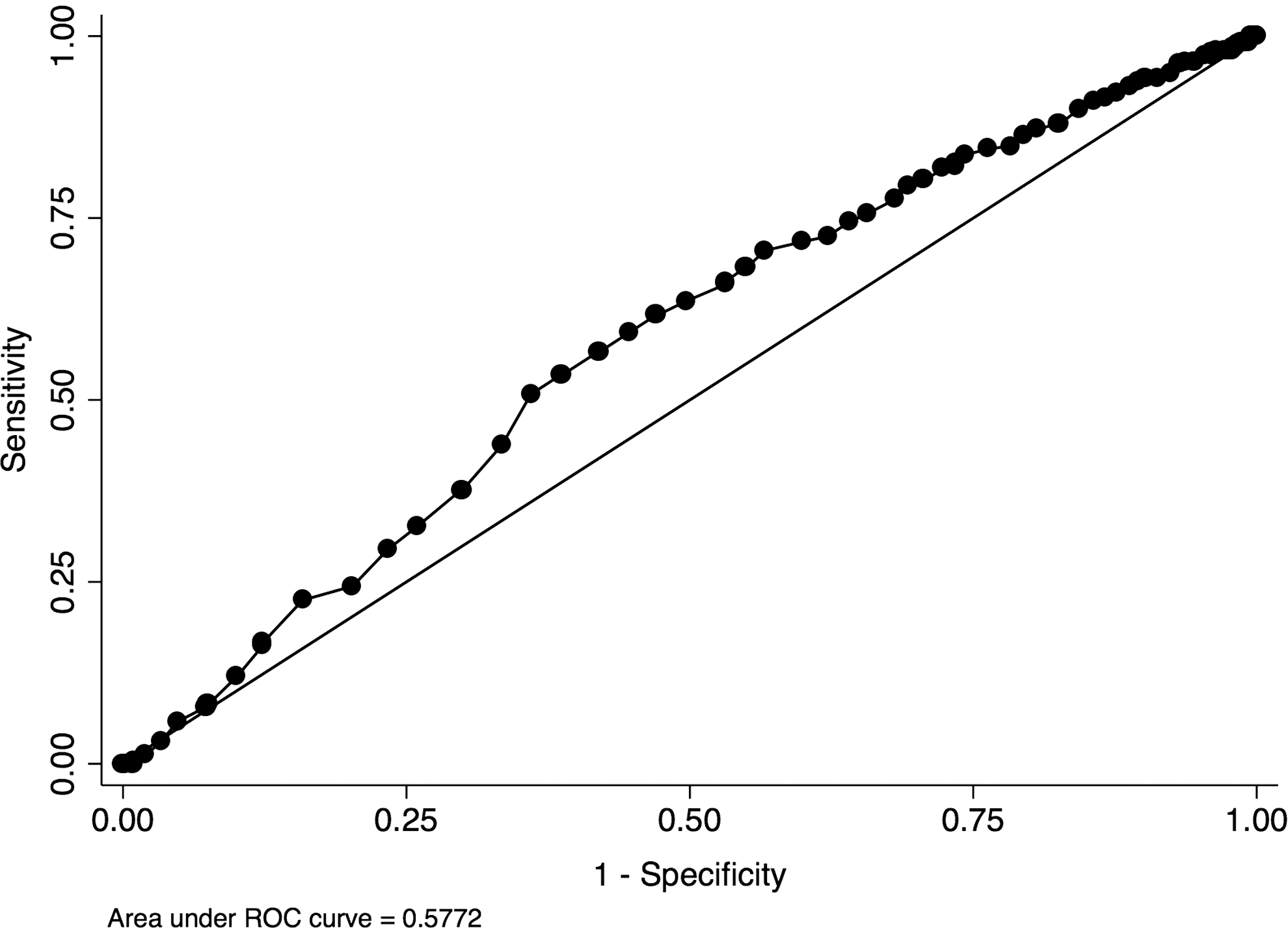
Ultrasound size alone is a poor predictor of malignancy in all thyroid nodules regardless of FNA status (n = 1003, AUC = 0.577), in those that underwent FNA (n = 548, AUC = 0.615, not pictured), and in those that did not undergo FNA (n = 455, AUC = 0.601, not pictured). AUC, area under the curve; ROC, receiver operating characteristic.
Ultrasound size as a predictor of pathologic size
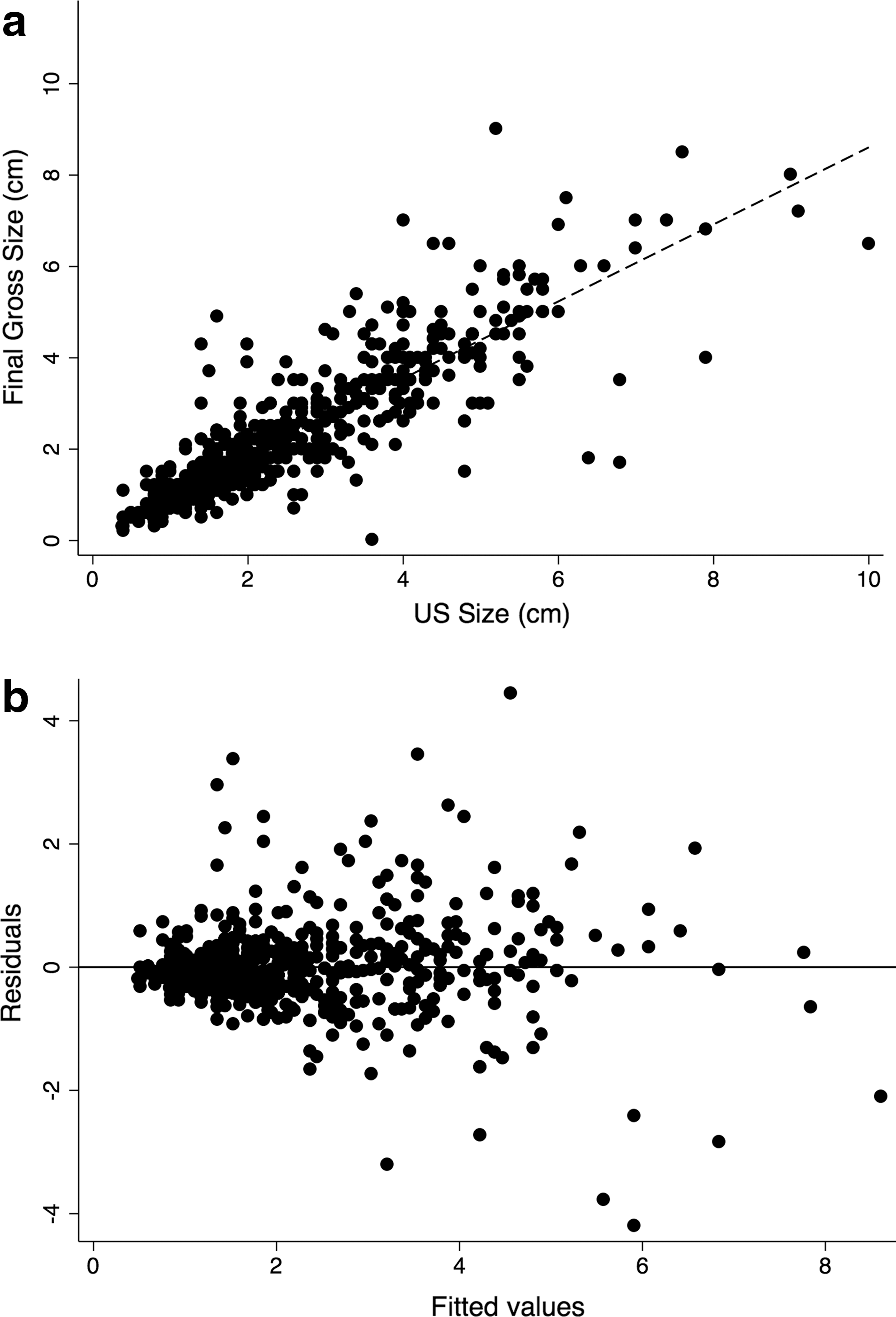
Nodule size at ultrasound was compared to final size at pathologic examination for both benign and malignant nodules (n = 549). Linear regression demonstrated that preoperative ultrasound size does correlate with final pathologic size (R 2 = 0.748; p < 0.001), however, ultrasound tends to overestimate the pathologic size of thyroid nodules by 15.7% (95% CI, 19.8–11.6%) (Fig. 3a). Significant heteroscedasticity in the residual plot demonstrates that ultrasound size correlates less with final pathologic size for larger nodules in a bidirectional, nonlinear manner (Fig. 3b).
(
Of these 549 nodules, 241 (43.9%) were malignant at final diagnosis. A significant change in size in these nodules (at final pathologic examination compared with ultrasound) would be clinically relevant for staging purposes. Therefore, a detailed analysis of this subgroup was performed. Most carcinomas would have either stayed within the same stage (n = 169, 70%) or changed by one stage (n = 68, 28%) (Table 9). Of those that changed by one stage, 49 would have decreased and 19 would have increased stage. Four carcinomas (2%) changed by two stages: one changed from T3 to T1b (this nodule measured 6.8 cm on ultrasound but 1.7 cm on gross examination—however, the histologic description notes diffuse intrathyroidal lymphatic spread, perhaps accounting for the larger sonographic size); and three changed from T1b to T3 (in one case, the ultrasound size was 1.6 cm but the carcinoma diffusely involved an entire lobe of 4.9 cm; the other two nodules were in the same lobe in the same patient: they were measured separately on ultrasound at 2 and 1.4 cm; however, the gross interpretation was of a single nodule measuring 4.3 cm).
Of 241 malignant thyroid nodules, the majority (n = 169; 70%) would have stayed in the same stage category. Forty-nine (20%) would have decreased by one stage, and nineteen (8%) would have increased by one stage. Four (2%) would have changed by two stages: one decrease and three increases.
Accuracy of FNA diagnosis
The malignancy rates by Bethesda System Category for each size group were analyzed (Table 10). In nodules with a benign (Bethesda II) FNA diagnosis, the overall malignancy rate was 3.2% (5/155) (so-called “false negative” rate). The highest false negative rates (6–8%) were in nodules between 3 and 6 cm. In nodules with a malignant (Bethesda VI) FNA diagnosis, occasional benign diagnoses were rendered at final histologic examination (overall 2.6% “false positive” rate).
All false negatives were reviewed in detail: The single false negative nodule <3 cm measured 1.4 cm at ultrasound and required several passes by FNA. It was a calcified classic PTC measuring 1.2 cm at final examination. Of the 4 nodules ≥3 cm, 3 were encapsulated follicular variants of papillary thyroid carcinoma, all of which met criteria for NIFT-P on retrospective review; 1 was a classic papillary thyroid carcinoma that had a simultaneous FNA of a benign nodule on the contralateral lobe which was read as atypia of undetermined significance, potentially reflecting a labeling swap. There were two additional nodules not included in the table due to lack of ultrasound size: one measured 1.7 cm on neck CT scan and was called benign on FNA and follicular carcinoma on final pathology; the other appeared as an ill-defined area on ultrasound, was called benign on FNA, and a 0.7 cm papillary microcarcinoma was identified at final histology.
All false positives were reviewed in detail, and all three patients underwent total thyroidectomy: There were two possible false positive nodules <3 cm. One measured 0.9 cm on ultrasound, was called PTC on FNA, was frozen intraoperatively, and was a 1.5 cm “atypical follicular focus” at final diagnosis. A papillary microcarcinoma was identified on the contralateral lobe. This atypical focus likely represents carcinoma but could not be diagnosed with certainty. The other measured 1.1 cm on ultrasound and was called PTC on FNA. On final histology, multifocal papillary microcarcinomas (0.5 cm or less) in a background of benign colloid nodules were found. In this case, it was not clear if the microcarcinoma or the benign colloid nodule underwent FNA. In both cases, carcinoma was found in the thyroid. The single false positive nodule >3 cm measured 4.6 cm on ultrasound and was diagnosed on FNA as “malignant tumor cells” with medullary carcinoma as a possibility. The final diagnosis was a 4 cm microfollicular adenomatous nodule with marked nuclear pleomorphism attributed to severe endocrine type atypia.
Discussion
Management of thyroid nodules is based on clinical context, ultrasound features, and fine needle aspiration biopsy. The vast majority of nodules are benign; therefore, appropriate classification is crucial to avoid unnecessary thyroid surgery. This study examined the relationship between nodule size and malignancy risk and attempted to characterize the relationship between nodule size at ultrasound and at pathologic exam as well as the accuracy of FNA diagnosis.
Ultrasound size and malignancy risk
Several large studies have examined the value of thyroid nodule size as a predictor of malignancy; however, results are discrepant. In a recent meta-analysis, Shin et al. summarized the findings of 10 studies that looked at thyroid nodules with pre-operative FNA diagnoses, post-operative histologic diagnoses, and size comparisons of at least 3 cm (17). Three studies demonstrated a higher risk of malignancy in nodules ≥4 cm compared with those <4 cm: 24% versus 12% in 571 patients (18), 58.2% versus 37.3% in 159 patients (19), and 15% versus 12.3% in 4955 patients (7). One study showed a higher risk of malignancy in nodules ≥3 cm compared to <3 cm (23.2% versus 18% in 765 patients); however, in the subset that underwent surgical resection, there was no difference (23.1% versus 18% in 262 patients) (20). Five studies concluded that larger nodules were not at increased risk of malignancy compared to smaller nodules (n = 451, 1068, 3013, 621, 84) (9,11,17,21 –24). One study demonstrated an inverse relationship between size and malignancy risk, with increasing size showing decreasing risk in a nonlinear manner (25). This group examined outcomes in 676 patients undergoing thyroidectomy over a 17-year period at a tertiary care center. They observed an overall malignancy rate of 23.6% (n = 160). The mean nodule size was significantly larger for benign nodules (4.4 ± 2.4 cm) versus malignant nodules (3.3 ± 2.2 cm) (p < 0.001). In the subset of patients (n = 549) who underwent FNA biopsy prior to surgery, the mean size in benign versus malignant nodules as a function of FNA diagnostic category was not statistically significant (25). Kamran et al. examined 7348 nodules in 4955 patients over a 14-year period with an overall malignancy rate of 13% (7). They observed no graded increase in malignancy risk for nodules >2 cm: 10.5% in nodules <2 cm versus 15% in all nodules >2 cm. These findings suggest that a size-risk threshold exists at approximately 2 cm. Interestingly, when examined by type of thyroid malignancy, the rate of follicular carcinoma increased with increasing nodule size, while an inverse relationship was observed with papillary thyroid carcinoma and nodule size (7), perhaps explaining conflicting results observed by previous authors.
We examined nodule size and final pathologic diagnosis in 659 patients with 1003 nodules and observed the highest malignancy risk in nodules <2 cm (∼30%), with no graded decrease in risk beyond the 2 cm threshold (∼20%). Like Kamran et al. (7), we found a risk cutoff at 2 cm; however, they found lower risk in smaller nodules, while we found higher risk in smaller nodules. We observed that when FNA was performed prior to resection (548 nodules), size increase in centimeter increments corresponded to a step-wise decrease in malignancy rate (with the exception of a small increase at 5–5.9 cm) (Table 5; Fig. 1). Using ultrasound size thresholds as a tool for prediction of malignancy in all 1003 nodules, we found higher risk of malignancy in nodules <2, <3, and <4 cm (11.2, 8.7, and 7.5% difference in risk, respectively). Evaluating only nodules with FNA, we found greater differences in the risk of malignancy at the same size thresholds (16.0, 15.6, and 15.6% difference in risk, respectively). We also found a significant difference in risk (14.7%) using a 5 cm threshold (Tables 4 and 6). In nodules not subject to FNA, we only found a significantly higher risk (7.7% difference) in nodules <2 cm compared with ≥2 cm. The higher rates of malignancy in nodules undergoing FNA (versus nodules subject to only ultrasound examination) implies that nodules chosen to be aspirated by the ultrasonagrapher have more worrisome sonographic features and result in more frequent malignant diagnoses. Appropriate triage by ultrasonographic characteristics in conjunction with size can aid in nodule evaluation and prediction of malignancy risk.
Ultrasound size and pathologic size
Review of the literature regarding radiology–pathology correlation of thyroid nodules reveals only a few articles dedicated to the topic. Bachar et al. examined ultrasound size and pathologic size in 292 patients with papillary thyroid carcinoma over a 5 year period. They observed significant size discrepancies for papillary thyroid carcinoma at ultrasound examination for small and large nodules. Approximately 18% of nodules >1 cm at ultrasound were found to be <1 cm at pathologic exam. The findings were similar for nodules >4 cm at ultrasound, of which 7.2% were found to be <4 cm at pathologic examination. Given these data and the confounded clinical evaluation that may result from a nodule size misclassification, the group advocated consideration of size discrepancies in clinical decision making (15). Deveci et al. similarly found a correlation of ≤50% for nodules measuring >1 cm and concluded that these discrepancies may lead to unnecessary FNA and surgery (24).
We observed relatively good correlation between ultrasound size and pathologic size. In general, ultrasound tended to overestimate size compared with pathologic examination, perhaps due to apparent coalescence of nodules on imaging. Furthermore, smaller nodules correlated somewhat better than larger nodules, in which sonographic size determination may not have reflected pathologic size.
The heteroscedasticity observed in our residual plot for ultrasound size versus final pathologic size signifies that the variability in the range of final pathologic sizes is unequal across ultrasound sizes. In this case, larger nodules tended to vary more in final size and are measured both smaller and larger than at ultrasound. Clinically, this variability is important if large nodule size is an indication for surgery. Specific size thresholds used to qualify a patient for surgery may have less value if the size of a large nodule at ultrasound is less predictive of its final size. Considering size discrepancies, most malignant nodules (70%) would have stayed within the same stage, 21% would have decreased stage, and 9% would have increased stage, most by only one stage.
Ultrasound size and accuracy of FNA diagnosis
Recent studies have argued that large thyroid nodules have greater rates of malignancy but may not be associated with a decrease in accuracy of cytology, with overall false negative rates (malignant histology of a nodule with benign cytology) ranging from <1% to 12% (7,9,26,27). Others have observed higher false negative rates in nodules ≥3 or 4 cm (10–13% in larger nodules compared to 5–6% in smaller nodules) (14,19,20,28 –30) leading to a recommendation for surgery as management of these nodules, regardless of FNA diagnosis (10,31). Our raw data appear to support somewhat increased false negative rates in nodules ≥3 cm (5.8% for all nodules ≥3 cm versus 1.2% for all nodules <3 cm); however, 3 of the 4 false-negative results in nodules ≥3 cm were encapsulated follicular variants of papillary thyroid carcinoma (FVPTC). All 3 cases were reviewed by 2 pathologists (N.A.C., T.A.), and all met criteria for NIFT-P (noninvasive follicular thyroid neoplasm with papillary-like nuclear features) (16). If these three nodules are not considered definitively malignant, the difference in false-negative rates based on size disappears: 1.4% for all nodules ≥3 cm versus 1.2% for all nodules <3 cm. Interestingly, FVPTCs have been described as a common source of false negatives, possibly due to sampling error (9,20,32 –34), but they are also more frequently diagnosed as Bethesda III, IV, or V on cytology (35 –37). Eliminating the FVPTCs from studies with high false negative rates in larger nodules yields false negative rates of 4–5% in nodules ≥3 or 4 cm (10,14,28). Given the new classification of encapsulated FVPTCs, false negative rates and overall rates of malignancy are expected to decline.
Fewer studies have addressed false positive rates, likely because of lower rates compared to false negatives. Our false positive rate was low (2.6%, 3 cases total) and includes 2 equivocal cases in which either the final diagnosis was “atypical” and likely malignant or site correlation between benign and malignant nodules in the same thyroid could not be established with certainty. In both equivocal cases, carcinoma was present in the total thyroidectomy specimen. In a single nonequivocal false positive case, the patient underwent total thyroidectomy for benign disease diagnosed as malignant on cytology.
Limitations
This study was conducted retrospectively at a single medical center and is limited by referral and selection bias. A proportion of the patient population included those referred specifically for thyroid resection. Patients known to have benign nodules by FNA may not have been referred to our center, potentially resulting in a higher incidence of malignant cases. Also, thyroid nodule characteristics at ultrasound are important factors in the decision to proceed to fine needle aspiration biopsy. This study did not analyze the role of nodule characteristics at ultrasound in the clinical decision making process. Nodules appearing suspicious at ultrasound are more likely to be selected for FNA biopsy and therefore represent a potential source of selection bias.
In addition, definitive correlation between ultrasound and pathology reports was often difficult due to lack of precise location reporting. On occasion, ultrasound reports specified a dominant nodule, while gross examination revealed multiple nodules in the same lobe. If the nodules were similar in size, it was unclear which nodule was measured at ultrasound. Every effort was made to ensure adequate correlation; however, some cases remained ambiguous and were excluded from analysis. Size reporting at gross or histologic exam is also known to be subject to interobserver variability, as there is no clear consensus for measuring tumor foci that are adjacent but discontinuous.
Finally, this study is limited by data bias. It is unlikely that every benign sub-centimeter nodule was analyzed at the time of gross examination or documented in the final report. However, sub-centimeter nodules are commonly identified at ultrasound and subject to fine needle aspiration biopsy at our institution. The smallest nodule subject to FNA in this study was 0.4 cm, was diagnosed as suspicious for papillary carcinoma on FNA, and was papillary carcinoma on histology. All malignant nodules less than 1 cm that were subject to fine needle aspiration were double-checked by the principle investigator, and all maintained correlation. Because we were able to establish correlation between ultrasound, FNA diagnosis, and final diagnosis, we did not exclude cases under a minimal size threshold. We acknowledge that subcentimeter nodules may not undergo aspiration and/or resection at all institutions, which may result in varying rates of malignancy for subcentimeter nodules.
Conclusion
All thyroid nodules, regardless of size, possess malignant potential. Large size should not be considered an independent predictor of malignancy, as larger lesions do not have an intrinsically increased risk of malignancy in this study. Instead, larger nodules tend to have lower rates of malignancy compared with smaller nodules. Additionally, nodules determined to meet criteria for fine needle aspiration have overall higher rates of malignancy. False negative rates (when correcting for encapsulated follicular variants of papillary carcinoma) are low (<2%). All lesions with the appropriate constellation of clinical and radiographic findings should undergo fine needle aspiration biopsy regardless of size. Minimal size discrepancies between ultrasound and pathologic size could be taken into account for larger nodules when determining clinical management. Both size and FNA diagnosis should influence the clinical decision-making process. We advocate that nodules of all sizes should undergo FNA biopsy when clinically and radiographically appropriate to guide further management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.