
Abstract
Background:
Different and conflicting data have been published concerning thyrotropin (TSH) levels among small-for-gestational-age (SGA) and appropriate-for-gestational-age (AGA) newborns. The hypothesis of this study was that SGA preterm infants have higher TSH levels than those who are not underweight do.
Methods:
This cross-sectional study analyzed the TSH levels of all preterm newborns with a negative congenital hypothyroidism screening result (TSH <7.5 μIU/mL). Secondary variables were sex, birth weight (SGA, AGA), days of life at blood extraction, maternal origin, gestational age, and being a twin or not. Two multiple linear regression models were constructed comparing TSH levels in SGA and AGA or the z-score for birth weight and the remaining variables.
Results:
A sample including 5819 preterm infants was obtained: 53.8% male, 23.3% twins, and 3.3% SGA. TSH concentrations were 2.16 ± 2.0 μIU/mL for the SGA infants and 1.80 ± 1.5 μIU/mL for the AGA infants (p = 0.012), with a negative correlation (p < 0.001) between TSH levels and the z-score for the weight of the newborn. The multivariate analysis comparing TSH levels between SGA and AGA gave the following: SGA (B = 0.46, p < 0.001), Latin American mother (B = −0.16, p = 0.029), days of life at blood extraction (B = −0.26, p < 0.001), and gestational age ≤28 weeks (B = −0.56, p < 0.001). Using the z-score for the weight, the associations were: maternal origin North Africa (B = 0.19, p = 0.042), days of life at blood extraction (B = −0.27, p < 0.001), gestational age ≤28 weeks (B = −0.55, p < 0.001), and z-score for weight (B = −0.12, p < 0.001).
Conclusions:
Our multivariate analysis suggests that TSH concentrations are higher in SGA infants than they are in AGA infants, and this should be taken into account when establishing a reference interval appropriate for this population. The clinical relevance remains unknown, but lines of research are opened that may allow a better understanding of the long-term morbidities in these newborns.
Introduction
T
Disagreement exists regarding the definition of SGA. Some authors define SGA as those newborns whose birth weight is below the mean minus two standard deviations for gestational age (2), while other authors consider it to be a birth weight <10th percentile. SGA has also been defined more strictly as a birth weight falling below the third percentile (3). In all cases, values are based on the reference population. SGA affects >20% of births worldwide (4). Most SGA births occur in Africa and Asia, whereas the prevalence of SGA in Europe and the United States is around 8–12%, or >95,000 SGA births.
Due to fetal growth restriction and an immature metabolism at birth, SGA has been associated with several development disorders, including an increased risk of congenital hypothyroidism (5 –7). Certain hormones, especially thyroid hormones, are crucial for growth and neurocognitive development. Fetal growth restriction produces alterations in thyroid and adrenal function at birth (8), demonstrated by the higher thyrotropin (TSH) values seen in SGA infants compared with appropriate-for-gestational-age (AGA) infants (9), which might be explained by a reduction in the expression of thyroid receptor isoforms in the cerebral cortex and cerebellum in these fetuses (10).
Because thyroid hormones are crucial for growth and neurocognitive development, some studies have compared thyroid function in SGA and AGA based on the hypothesis that TSH concentrations differ between these two population groups. As different and conflicting results have been published (10 –12), a study was designed to elucidate whether thyroid function differs between SGA and AGA, and to establish the reasons for the conflicting results in the literature.
This study was performed in preterm infants because this group frequently has thyroid dysfunction (13,14), with SGA being an additional risk factor. The innovative aspect of this study is its focus on determining whether the lower weight for gestational age at birth of the preterm infant can influence TSH levels, eliminating the influence of other relevant variables through a multivariate analysis, since the confounding effect of other variables could show false associations. This methodology has not been applied in previous studies. Moreover, most authors have used birth weight and not z-score for gestational age and sex. The current methodology enables a better understanding of the relationship between SGA and TSH levels.
The hypothesis of the study was that TSH levels are higher in SGA preterm infants than they are in those who are not underweight.
Materials and Methods
Study population
Preterm newborns (gestational age <37 weeks) in the province of Alicante (Spain) born between 1 January 2008 and 31 December 2012 were included in this study.
Study design and participants
This cross-sectional study analyzed a sample of newborns and comprised the blood samples for the Neonatal Congenital Hypothyroidism Screening Program taken from all preterm newborns. This public screening program has a participation rate of 99.9% (15) of all newborns, which yields representative results for this population. Blood was drawn from the preterm newborns within a few days of birth through heel stick and dried on Whatman 903 paper.
Inclusion criteria were the following: having obtained parental informed consent, a sample with defined quality (15), a negative result in the congenital hypothyroidism screening (TSH <7.5 μIU/mL), and an age at sampling >24 hours but <8 days of life, following the recommendations of the Neonatal Congenital Hypothyroidism Screening Program of the Generalitat Valenciana, Spain (16).
Variables and measurements
The primary variable was the TSH value. Quantification of TSH was performed with the Perkin Elmer AutoDELFIA® Neonatal hTSH kit using a TSH cutoff value of 7.5 μIU/mL, as per the majority of the Spanish laboratories performing this test according to the Spanish Neonatal Screening Association (AECNE) criteria (15). The intra- and inter-assay cutoff values were 7.0% and 8.0%, and the sensitivity limit was 0.2 IU/mL. To ensure correct measurement, before each assay, an internal quality control must be passed. Required external quality assurance controls include a monthly AECNE quality assessment in neonatal early detection and a quarterly assessment by the Newborn Screening Quality Assurance Program of the Centers for Disease Control.
Secondary variables collected from each preterm infant from the patient data taken during blood sampling at the hospital were: sex, birth weight, days of life at blood extraction, maternal origin (Western Europe, Eastern Europe, America, North Africa, South Africa, and Asia), gestational age, and being a twin or not. Data collection was considered successful when the number of missing values in each of the variables was <1%.
The variables were grouped as follows: SGA when weight at birth was at least the third percentile for the weight of the infant based on data derived from an appropriate reference population, and AGA for the rest of the preterm infants. The third percentile was chosen because there is consensus on the proper definition of the severe forms of intrauterine growth restriction, and this is, in practice, almost identical to the criteria of two standard deviations (2,3). Gestational age was grouped according to the severity of prematurity (severe ≤28 weeks, mild 28–32 weeks, and late prematurity 32–37 weeks). These intervals were chosen based on the recommendations of the Standards Committee of the Spanish Society of Neonatology (17). Finally, z-scores for birth weight were calculated.
Sample size
The power of contrast was calculated for the difference between the means of the two independent groups with the sample collected (n = 5819). Using 95% confidence intervals (CI), an expected standard deviation in both groups of 2 μIU/mL, and to find a difference of 0.5 μIU/mL, the power of contrast was 99.9%.
Statistical analysis
The descriptive analysis of the quantitative variables was performed by calculating the means and standard deviations, while the quantitative variables were described using frequencies and percentages. TSH levels were compared between the defined weight groups (AGA and SGA) using the t-test (quantitative variables). Spearman's correlation coefficient was determined to examine the association between TSH levels and z-score for weight. Finally, a multiple linear regression model was constructed, using TSH levels as the dependent variable and SGA/AGA (weight <P3), sex, gestational age, days of life at blood extraction, maternal origin, and being a twin or not as independent variables. Thus, the possible influence of low birth weight on TSH levels was analyzed. Model assumptions were verified using graphical and analytical testing, and the goodness-of-fit was verified by the analysis of variance test. Another multivariate model was constructed with the above features, using the z-scores for birth weight as the variable in place of SGA/AGA, as these two variables show collinearity. All analyses were performed with a significance level of 5%, and for each relevant parameter, its associated CI was calculated. The statistical package used was IBM SPSS Statistics for Windows v19.
Ethical issues
The neonatal screening studies were approved by the Ethics Committee of the Valencian Community. Informed consent was obtained from each newborn's parent or guardian, in compliance with the current medical ethics legislation. The data, collected from routine clinical practice in neonatal screening, were anonymized and encrypted, satisfying the data protection law.
Results
In a sample of 5819 preterm infants, 190 (3.3%) were SGA. Table 1 shows the descriptive and analytical characteristics of the sample. Regarding the description of the variables, 23.2% of the children had at least one twin, the mean days of life at blood extraction was four, and the mean z-score for weight for gestational age and sex was −0.1.
Mean TSH for weight percentiles (t-test: t = 2.54, p = 0.012): (i) <P3: 2.16 ± 2.0; (ii) ≥P3: 1.80 ± 1.5.
Spearman correlation between TSH values and z-score for weight: −0.054, p < 0.001.
Goodness-of-fit of the models (ANOVA): (i) qualitative model: F = 42.44, p < 0.001; (ii) quantitative model: F = 44.07, p < 0.001.
TSH, thyrotropin; N/A, not applicable; CI, confidence interval; B, coefficient for the indicated factor; w, weeks; n (%), absolute frequency (relative frequency); x ± s, mean ± standard deviation; ANOVA, analysis of variance.
When the mean TSH values between SGA and AGA were compared (Table 1), significantly higher levels (p = 0.012) were found in the SGA group. Comparing the z-score with the TSH values, a negative correlation was found (p < 0.001). In the multivariate analysis, using weight as a qualitative variable (SGA), the following factors were found to be significantly associated with TSH: SGA (B = 0.46, p < 0.001), Latin American mother (B = −0.16, p = 0.029), days of life at extraction (B = −0.26, p < 0.001), and gestational age ≤28 weeks (B = −0.56, p < 0.001). In the model using the z-score for birth weight, the associations were: North African origin (B = 0.19, p = 0.042), days of life at extraction (B = −0.27, p < 0.001), gestational age ≤28 weeks (B = −0.55, p < 0.001), and z-score for weight (B = −0.12, p < 0.001). The associations between weight and TSH values are shown graphically in Figures 1 and 2.

Predicted values of thyrotropin (TSH) using the qualitative model. Values adjusted by: sex, having a twin, weight <P3, maternal origin, days of life at extraction, and gestational age. p-Value obtained through the goodness-of-fit of the model (analysis of variance [ANOVA]).
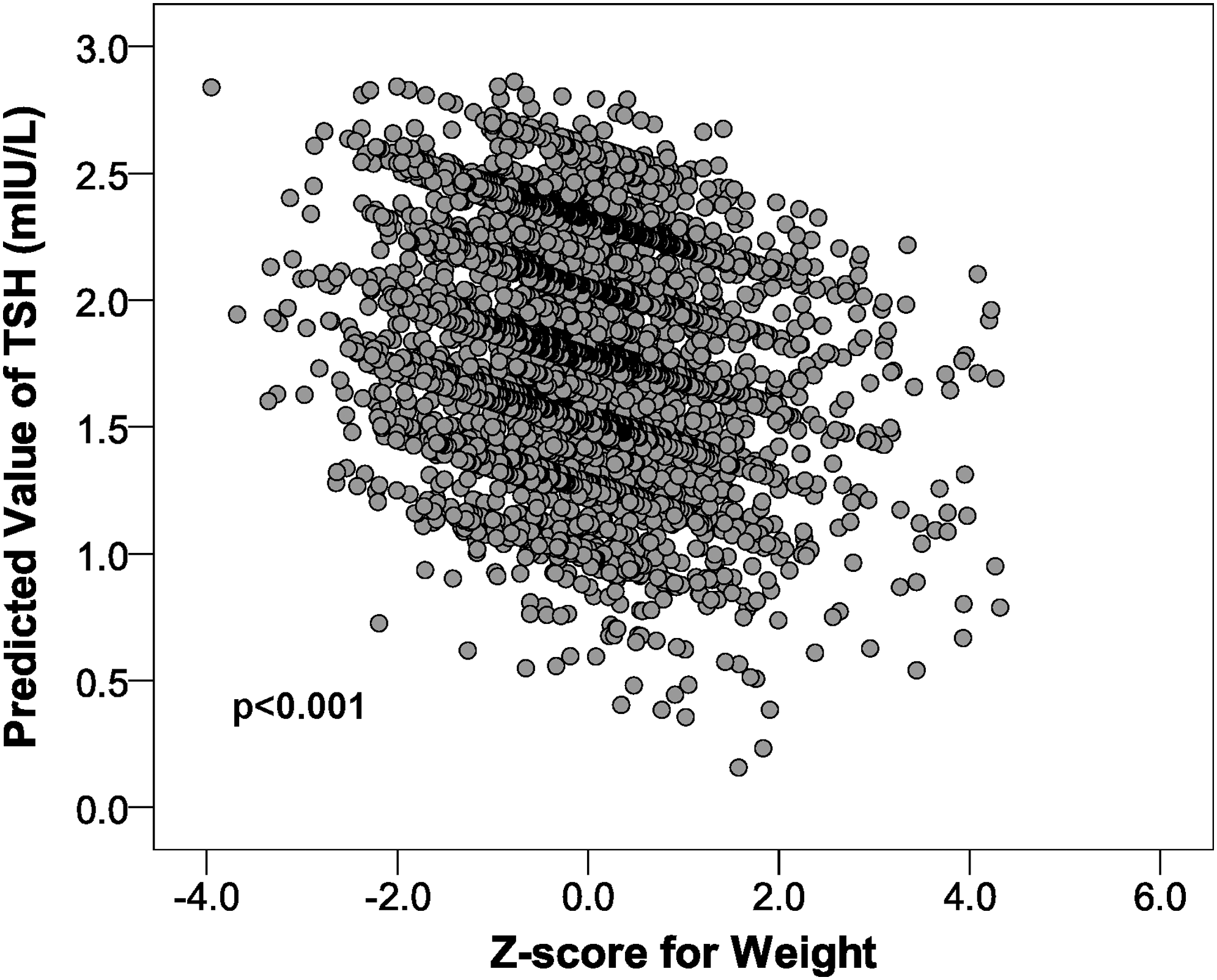
Predicted values of TSH using the quantitative model. Values adjusted by: sex, having a twin, z-score for weight, maternal origin, days of life at extraction, and gestational age. p-Value obtained through the goodness-of-fit of the model (ANOVA).
Discussion
In a large sample of 5819 preterm infants, after applying the multivariate models using those variables that could influence the TSH of the preterm child (sex, twin, days of life at extraction, maternal origin, and gestational age), it was found that as intrauterine growth restriction increases, TSH levels are higher, using the restriction variable both qualitatively and quantitatively (Table 1 and Figs. 1 and 2). The importance of controlling for confounding factors that may affect the results is emphasized, as it is thought that they are the cause of the conflicting published results that find no differences in TSH levels between SGA and AGA. Some of these confounding factors or causes of disagreement include: incorrect distinction between preterm and SGA, not collecting prematurity data (preterm infants have higher TSH levels than term newborns) or the day of sample extraction (samples extracted before one day of life have higher TSH concentrations as a consequence of passing from a warm intrauterine medium to a colder extrauterine medium), misclassification of SGA, or studies with a small sample size.
The main strength of this study is the clinical idea of studying a group of preterm infants with varying degrees of intrauterine growth restriction through a multivariate analysis, unlike other authors who have studied the differences in the statistical means. Growth restriction was used quantitatively rather than the simple classification into two groups: AGA and SGA. The statistical power obtained by the large sample size must also be highlighted, which minimizes information bias, as the variables studied are automatically included. Furthermore, since all births are covered under the universal and free healthcare system, the sample represents nearly 100% of the overall population, minimizing selection biases. A limitation of the study is the measurement of TSH exclusively, without including thyroid hormones, such as free thyroxine (fT4), the levels of which are very important for interpreting TSH levels, especially in preterm infants, who are at risk for developing transient hypothyroxinemia of prematurity or mild hyperthyrotopinemia with normal fT4 (18). This was not possible because in this region, fT4 is generally not measured in the neonatal screening. Additionally, the influence on thyroid function of the following variables was not considered: maternal thyroid function, medically assisted reproduction, respiratory distress, and concomitant drugs (18 –20). These variables are not currently recorded in the neonatal screening and should be taken into account in future studies with multivariate models.
Similar results are obtained in term SGA infants, but the results are more contradictory than they are in preterm infants (10,11). The main reason for the higher TSH levels is unknown, although its origin could be multifactorial, as there are many hypotheses establishing its cause, including uterine stress with growth restriction, non-thyroidal illness, compensatory response to mild suppression of the thyroid gland, caloric restriction, immaturity of the hypothalamic–pituitary–thyroid axis (immaturity of the type 1 deiodinase enzyme or transient hypothyroxinemia of prematurity, low thyroxine-binding globulin), or less efficient thermogenic response, among others.
Neonatal screening studies assessing the association between TSH levels and birth weight in term and preterm children found a negative correlation, that is, higher TSH levels are associated with low birth weight. The justification for this association is not clear, though several possible explanations exist. First, fetal distress causes fetal hypoxia and acidosis, leading to increased TSH and decreased fT4, which can protect the fetus, reducing oxygen requirements (21,22). Second, fetal malnutrition itself can affect the synthesis of T4 by reducing the availability of its precursor thyroxine (10).
A clear example of confounding in this sense is the study of the relationship between TSH levels and other variables such as maternal age or multiple births (23) that predispose to premature or underweight birth. The influence of the variation in TSH levels is due solely to the variables premature birth and underweight birth. If this information is not collected, there is a risk that confounding factors may be present.
In this study, the variables sex, gestational age, being a twin, maternal age, and days of life at blood extraction did not affect the variation in TSH values. The lack of influence of the variable days of life at blood extraction is because samples taken before one day of life are not included in the study according to the quality criteria (15) established for the samples.
The clinical significance of high neonatal TSH values is under debate. Based on the importance of proper thyroid function, especially during pregnancy, for the overall development of the organism, some large cohort studies (24,25) in the United Kingdom and the United States associate high neonatal TSH values with a lower intelligence quotient and impairment of higher psychological processes at four years of age, although several small-sized studies argue otherwise (26). Further clinical significance of high neonatal TSH levels in SGA and preterm infants includes the need to establish an appropriate reference interval for this population that assures improved screening for congenital hypothyroidism. This is of great importance because some children with these characteristics could miss being screened (27).
In conclusion, this study suggests that TSH concentrations are higher in SGA than they are in AGA, and this should be taken into account when establishing an appropriate reference interval for SGA infants. The clinical relevance remains unknown, but avenues of research have been opened that may allow a better understanding of long-term morbidities of these newborns.
Footnotes
Acknowledgments
The authors thank Maria Repice for linguistic revision of the English version of this paper. No external funding was received for this study.
Author Disclosure Statement
No competing financial interests exist.