
Abstract
Purpose:
Differentiated thyroid cancer (DTC) is rare in children. Previous studies have suggested that it has different clinicopathologic features and mutation profiles compared with adult DTC. However, those studies focused on a single or limited number of gene mutations. This study comprehensively investigated a large series of pediatric DTC for single point mutations in BRAF, HRAS, KRAS, NRAS, PIK3CA, PTEN, and TERT. It also analyzed associations between clinicopathologic features and the BRAFV600E mutation.
Patients and Methods:
Eighty-nine consecutive cases seen in children and adolescents (≤18 years) during 1998–2015 were identified. Rare variants of DTC were excluded, and the study focused on 72 (91.1%) classical papillary thyroid carcinoma (PTC) and seven (8.9%) follicular variant PTC. These included 68 (86.1%) females and 11 (13.9%) males, with a median age of 15.5 years (range 8–18 years). The clinical and histopathological data were obtained from medical records. DNA was extracted from paraffin-embedded tumor tissue, and was PCR-amplified and directly sequenced.
Results:
Mutations detected included BRAFV600E in 19/72 (26.4%) classical PTC samples, and in none of seven follicular variant PTC. Other mutations included: 1/78 (1.3%) successfully amplified tumor samples with TERT C228T ; 2/79 (2.5%) NRAS 61 (c.181C>A and c.182A>G); 1/73 (1.4%) PIK3CA exon 9 (c.1589A>G and c.1598C>T in one tumor); 1/79 (1.3%) PIK3CA exon 20 (c.2951G>A); and 1/74 (1.4%) PTEN exon 5 (c.295G>A). No mutation was found in HRAS, KRAS, NRAS12, PTEN exons 6, 7, and 8, and TERT C250T . No significant association was found between BRAFV600E mutation and sex, extrathyroidal invasion, tumor multifocality, vascular invasion, lymph node or distant metastases, and persistent/recurrent disease.
Conclusions:
In pediatric DTC, the prevalence of the BRAFV600E mutation is significantly less common compared with adult DTC, and there is no association between this mutation and the histopathological features and outcome of PTC. PIK3CA, PTEN, NRAS 61, and TERT C228T mutations are rare.
Introduction
D
In addition to recognizing the increasing incidence of DTC in the last few decades, significant progress has also been achieved in the understanding of the molecular genetics of DTC (6). Somatic mutations involving a number of genes encoding components of the Mitogen-Activated Protein Kinases (MAPK) and the Phosphatidylinositol 3-kinase-AKT (PI3K-AKT) pathways are among the well-described genetic alterations in DTC (6). The BRAFV600E mutation is the most common mutation in PTC, while RAS mutations are common in follicular thyroid cancer (FTC) (6 –8). Mutations and copy number changes in the PIK3CA and PTEN genes occur in the less differentiated types of DTC (9). In all of these genes, single point missense mutations have been described with different rates in different subtypes of DTC. Another group of genetic alternations involve gene fusions, with RET/PTC1 and RET/PTC3 being characteristic rearrangements in PTC (10 –12), especially the radiation-induced PTC, and the PAX8/PPARy rearrangement in FTC (13 –15). Although there are extensive data on these genetic mutations in DTC, most of these data come from studies on adult patients, and there is a paucity of data on DTC in children and adolescents (referred to hereafter as pediatric DTC). In many regions of the world, including some parts of the Middle East, the data suggest an increasing incidence of Hashimoto's thyroiditis (16 –18). Hashimoto's thyroiditis has been associated with an increasing risk of DTC in both children and adults (19). Studies from Saudi Arabia have shown a clustering of thyroid cancer in females in the Central and the Eastern regions of the country, suggesting a role for environmental factors in the increased incidence of DTC (20).
Although there is also a trend of increasing incidence of DTC in children (21,22), it remains quite rare. Previous clinical and some molecular studies have suggested that it has different clinicopathologic features (23 –25) and genetic mutation profile (26 –30) compared with adult DTC. However, those studies focused on a single or a limited number of gene mutations in small samples. This study comprehensively investigated a large series of pediatric DTC for known single point mutations in BRAF, HRAS, KRAS, NRAS, PIK3CA, PTEN, and TERT. It also analyzed associations between clinicopathologic features and the BRAFV600E mutation in this pediatric sample. To the authors' knowledge, this is the first study that has analyzed the PI3K/AKT pathway in pediatric DTC, and it is the second study to report on TERT promoter mutation in pediatric DTC.
Patients and Methods
All children and adolescents aged ≤18 years (n = 89) seen at our institution during 1998–2015 were identified. The DTC subtypes included 72 (81%) classical PTC, seven (7.9%) follicular variant PTC, two (2.2%) tall-cell variant, three (3.4%) diffuse sclerosing subtype, three (3.4%) FTC, and two (2.2%) Hürthle-cell variant. The number of patients with tall-cell variants, diffuse sclerosing variant, FTC, and Hürthle-cell subtypes was too small for meaningful analysis, and only two cases (one tall-cell variant and one diffuse sclerosing subtype) were found to have a BRAFV600E mutation, with no mutations in the other genes. Therefore, these rare subtypes were excluded from further analysis, and the analysis was limited to classical PTC (72 cases) and follicular variant PTC (seven cases). These patients included 68 (86%) females and 11 (14%) males, with a median age of 15.5 years (range 8–18 years). Eleven (13.9%) patients were aged ≤11 years, 22 (27.8%) patients were aged 11.1–15 years, and 46 (58.2%) patients were 15.1–18 years of age. After obtaining Institutional Review Board approval, data were obtained from medical records. The median tumor size was 3 cm (range 1–8 cm). Tumor multifocality was present in 36 (45.6%), extrathyroidal extension in 29 (36.7%), and vascular invasion in 23 (29.1%) patients. Lymph node and distant metastases occurred in 61 (77.2%) and nine (11.4%) patients, respectively. All patients underwent near-total thyroidectomy, and 73 (92.4%) patients also underwent central ± lateral neck dissection (30 patients; 38%). Radioactive iodine (RAI) ablation/therapy was given to 73 (92.4%) patients, with a median dose of 107 mCi (range 29–210 mCi). Additional therapeutic interventions were performed in 32 (51.7%) patients, including additional surgeries in seven (8.8%), RAI in 10 (12.7%), or a combination of both in 15 (19%) patients. At a median follow-up of 5.4 years (range 1.2–16 years), 46 (58.2%) patients had an American Thyroid Association (ATA) response status of excellent, 27 (34.2%) were biochemically incomplete, two (2.6%) had a status of structurally incomplete, and one (1.1%) had an indeterminate status, while three (3.8%) were lost to follow-up after the initial RAI ablation.
Molecular studies: DNA isolation, polymerase chain reaction, and direct sequencing
The pathological tissue from each patient was examined by an experienced endocrine pathologist (H.A.), and the tumor tissue was carefully dissected from formalin-fixed paraffin-embedded tissues (FFPE). DNA was extracted using a commercial DNA extraction kit (catalog no. 56404 QIAamp DNA FFPE Tissue Kit; Qiagen) according to the manufacturer's instructions. DNA was quantified using a Nanodrop2000 spectrophotometer (Thermo Scientific), and DNA purity was assured by the A260/280 ratio of ≥1.8 indicating DNA with good purity. Polymerase chain reaction (PCR) and direct sequencing were undertaken using a Big Dye terminator v3.1 cycle sequencing reaction kit and an ABI PRISM 3730XL genetic analyzer (Applied Biosystems) to detect mutations in BRAF exon 15, HRAS, KRAS, and NRAS codons 12, 13, and 61 and TERT promotor mutations using the same primers and PCR conditions as previously described (8,31 –33).
Statistical analysis
Continuous data were summarized as median and range or mean ± standard deviation (SD), and a t-test was used for significance analysis. Categorical data are expressed as numbers and percentages or ratios, and Fisher's exact test and the chi-square test were used for significance analysis. In all statistical tests used, a two-tailed p-value of <0.05 was considered significant.
Results
BRAFV600E mutation in pediatric thyroid cancer
The BRAFV600E mutation (Fig. 1) was detected in 19/72 (26.4%) classical PTC samples (Table 1), but it was not detected in any of the seven follicular variant PTCs.
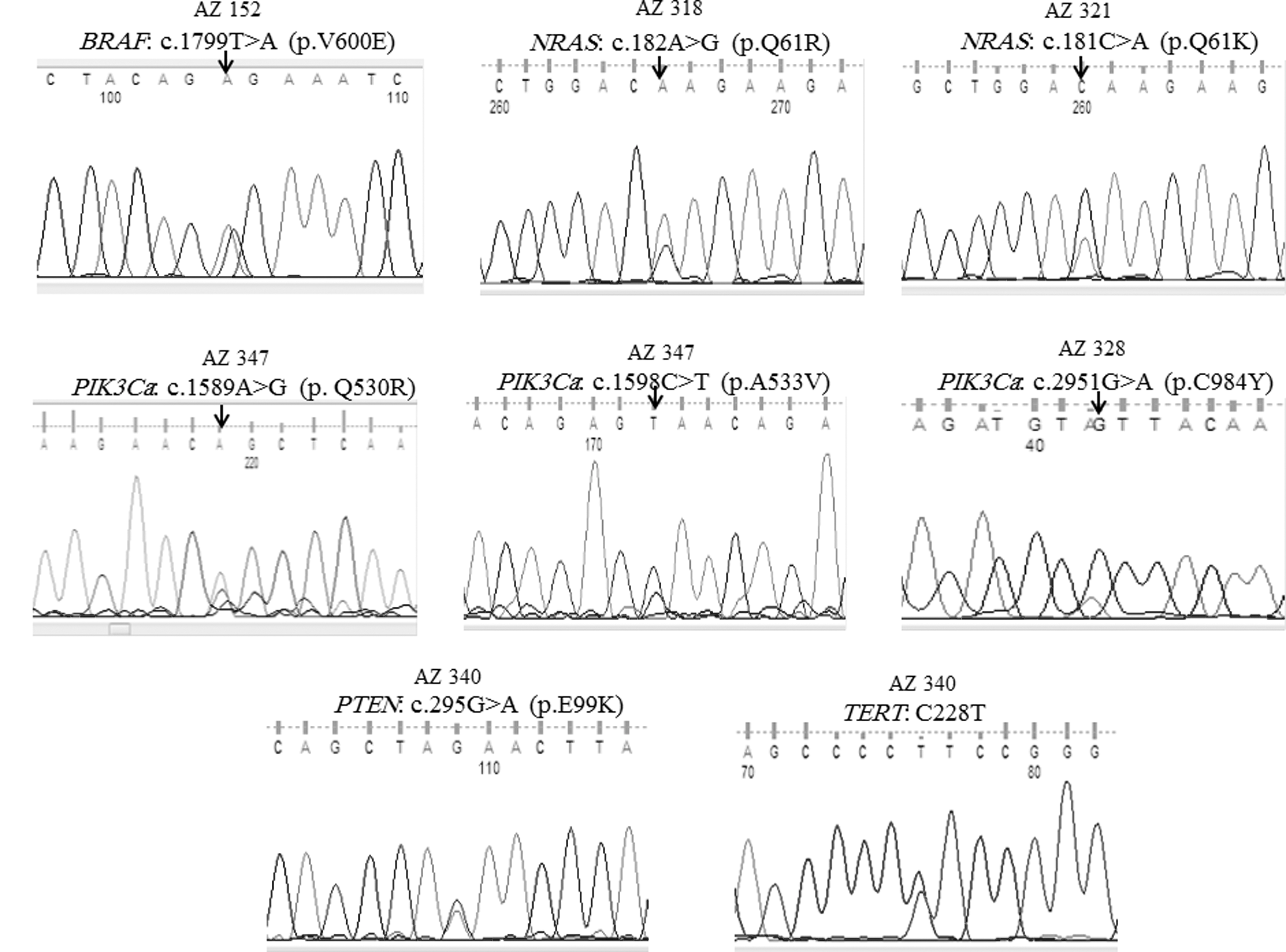
Sequence chromatograms showing various mutations detected in this series of pediatric differentiated thyroid cancer. Each mutation is labeled above each sequence showing the nucleotide and amino acid changes.
Total number of cases which have been successfully amplified by polymerase chain reaction.
Other genetic mutations in pediatric thyroid cancer
Other genetic mutations occurred rarely in pediatric DTC (Table 1). Only six patients had mutations in genes other than BRAF (Table 1 and Fig. 1). These mutations included 1/78 (1.3%) TERT C228T , 2/79 (2.5%) NRAS 61 (c.181C>A and c.182A>G), 1/73 (1.4%) PIK3CA exon 9 (c.1589A>G and c.1598C>T in one tumor), 1/79 (1.3%) PIK3CA exon 20 (c.2951G>A), and 1/74 (1.4%) PTEN exon 5 (c.295G>A) mutation. No mutation was detected in codons 12/13 and 61 of HRAS and KRAS and codon 12 of NRAS, PTEN exons 6, 7, and 8, and TERT promotor mutation C250T. The clinical, pathological, and outcome data of the six patients with these mutations are summarized in Table 2.
DTC, differentiated thyroid cancer; ETE, extrathyroidal extension/invasion; MF, tumor multifocality; RAI, radioactive iodine; LNM, lymph node metastasis; CPTC, classical papillary thyroid cancer; FVPTC, follicular variant papillary thyroid cancer.
Association of BRAFV600E mutation with histopathological features of PTC
BRAFV600E is the only mutation that occurred frequently enough to allow for a statistical analysis between its occurrence and the histopathological features and outcome of pediatric DTC. That analysis showed no significant association between BRAFV600E mutation and sex, age at diagnosis, tumor size, extrathyroidal invasion, tumor multifocality, vascular invasion, lymph node or distant metastases, and persistent/recurrent disease at 6–12 months after RAI and at the last follow-up visit (Table 3).
Discussion
Pediatric DTC remains rare, despite its increasing incidence (21,22). This has resulted in sparse data on its clinical, pathological, and molecular features. Relatively small series from different parts of the world have strongly suggested that DTC in the pediatric age is significantly different from that in adults in terms of its clinical presentation, pathological features, and outcome (23 –25,34 –38). In these series, pediatric DTC frequently presented with more aggressive features with higher rates of extrathyroidal invasion and lymph node and distant metastasis, and a higher tendency for persistent/recurrent disease (23 –25,34 –38). Despite these aggressive features at the time of the initial presentation, the long-term outcome is favorable, and disease-specific mortality is exceedingly rare (22,24,25). These differences in the clinicopathologic features and outcome of pediatric DTC have recently motivated the ATA to develop specific management guidelines for pediatric DTC (30).
In addition to the fact that the clinical profile is different, the small series of patients also suggested a different molecular profile of pediatric DTC compared with its adult counterpart (26,28,39 –41). These studies suggested a lower rate of single point mutations and a higher rate of gene rearrangements (27). BRAF and RAS mutations are associated with genetic instability and lower expression of the sodium–iodide symporter (NIS) (42,43). Low rates of these mutations in children with DTC may explain the generally better response of pediatric DTC to RAI and the lower rate of dedifferentiation and progression to more aggressive types of thyroid cancer (30). These points were highlighted in the recently released ATA guidelines for the management of thyroid nodules and thyroid cancer in children (30). These mutations and other molecular pathways associated with aggressiveness of PTC were also comprehensively reviewed in a recent publication (44). However, data on the molecular aspects of pediatric DTC are limited due to its rarity. Previous studies mostly included a small number of patients and focused on single or a limited number of genetic alterations (recently reviewed by Cordioli et al.) (45). This present study examined one of the largest series of pediatric DTC and comprehensively characterized the vast majority of single point genetic mutations that are known to occur in DTC.
The BRAFV600E mutation is the most common mutation in adult PTC (6). However, its prevalence in pediatric PTC has been variable but mostly much lower than that in adult PTC (27,40,46,47). Previously, a prevalence of 23% was found in 55 patients with pediatric DTC (26). The current study extended the search for this mutation and included an additional 22 pediatric patients, making a total of 79 patients with PTC or one of its variants. However, the rate of occurrence of the BRAFV600E mutation remained essentially the same (24.0%), confirming the results from the previous study and studies from other populations (26,28,41,48). By contrast, the prevalence of the BRAFV600E mutation in adult PTC patients is 48% (26), similar to that reported from many other populations (7). Thus, this difference in the rate of the BRAFV600E mutation between adult and pediatric DTC in an ethnically homogenous population strongly suggests that the lower prevalence of the BRAFV600E mutation in pediatric DTC is an intrinsic feature of these tumors and is not due to racial/ethnic differences in the rate of the BRAFV600E mutation between the present population and others. In fact, similar findings of low BRAFV600E prevalence in pediatric DTC have been reported in other populations (Table 4).
PCR, polymerase chain reaction; SSCP, single-strand conformation polymorphism analysis.
Several studies have identified a significant association between the presence of the BRAFV600E mutation and aggressive histopathological features, recurrence, and mortality in adult DTC (7,49 –52). The situation is different in pediatric DTC. Many studies have not shown a significant association between the BRAFV600E mutation and these features in pediatric DTC (28,39,53). The current study also did not find any association between BRAFV600E and sex, extrathyroidal invasion, tumor multifocality, vascular invasion, lymph node or distant metastases, and persistent/recurrent disease (Table 3). This apparently paradoxical situation in the association between BRAFV600E and aggressive tumor features and outcome in pediatric versus adult DTC is not well explained. It has been known that age is a strong predictor of tumor aggressiveness and outcome of DTC. It is possible that the age effect dominates over the BRAFV600E effect. In addition, TERT promoter mutations were found to exert a synergistic prognostic effect with BRAFV600E in PTC (54,55). Since TERT is common in adult DTC and very rare in pediatric PTC (26), it is possible that the tumorigenic effect of BRAFV600E is influenced by TERT promoter or other genetic mutations; when those mutations are rare or absent such as in pediatric DTC, the BRAFV600E effect significantly decreases or disappears.
RAS mutations have been reported to occur with variable rates in adult DTC, depending on the tumor histotype (6,8,56). Its prevalence is about 40% in FTC, 11% in PTC, 11% in Hürthle cell carcinoma, 33% in poorly differentiated thyroid carcinoma, and 53% in anaplastic thyroid carcinoma (ATC) (57). These mutations occur mostly in the NRAS isoform (8,57). In pediatric DTC, RAS mutations have been rarely investigated. In three studies that included 84 patients of non-radiation-induced pediatric DTC, only three (4%) patients had RAS mutations (29,58,59). The mutation rate ranged between 0% and 7.4%, and they were all NRAS 61 mutations (29,58,59). The rate of RAS mutations is even lower in radiation-associated pediatric DTC. No RAS mutation was found in three studies including 75 patients of radiation-associated pediatric DTC (29,59,60). Similarly, in the present study, a low rate of RAS mutations was found, with only two (2.5%) patients carrying NARS 61 codon mutations (Table 1).
To the authors' knowledge, the PI3K/AKT pathway has rarely, if ever, been investigated for mutations in pediatric DTC. This study is the first to investigate mutations in PIK3CA and PTEN in a relatively large pediatric sample. Low rates of these mutations were found, with only four mutations: two in exon 9 of PIK3CA in one tumor, one previously described mutation in PIK3CA in exon 20, and another known mutation in PTEN exon 5 (Table 1). In a previous study of 207 adult PTC from the same ethnic population as the patients in the present study, four (1.9%) patients had PIK3CA mutations (61). These mutations occurred in exon 9 and 20 of the PIK3CA but occurred in different codons compared with the ones found in this study (61). However, the rate (1.9%) of PIK3CA mutations in that report is only slightly higher than the rates found in this study (∼1.3%) (61). Hence, it seems that PIK3CA and PTEN mutations are uncommon in adult and pediatric well-differentiated types of thyroid cancer, but they seem to occur more commonly in the less differentiated types of thyroid cancer and ATC (9).
TERT promoter mutations have recently gained significant attention. Since their original description in thyroid cancer in 2013 (33), several studies have identified them in different parts of the world (reviewed by Alzahrani et al. and Liu and Xing) (32,62). Their overall rate in thyroid cancer is about 12–15%, with much higher rates in the less differentiated subtypes compared with DTC (32,62). In addition, they have been found to correlate with more aggressive histopathological features and outcomes of thyroid cancer (32,62). They have also been reported to be associated with the BRAFV600E mutation, and to confer worse prognosis when they occur together in the same tumor (54,63). A very low rate of these mutations has recently been reported in 55 patients with pediatric thyroid cancer (26). In the current study, the search was extended to a larger sample of pediatric DTC, and a similar low rate of TERT promoter mutations was found in pediatric DTC, confirming the previous findings and suggesting a minor or no role for TERT promoter mutations in pediatric DTC (26).
This study is one of the largest studies on the molecular genetics of pediatric DTC. It comprehensively analyzed most of the known single point mutations in pediatric DTC, including, for the first time, PIK3CA and PTEN mutations in this age group. However, this study has a number of shortcomings. No search was made for fusion genes such as RET/PTC 1, RET/PTC 3, or PAX8/PPARy due to technical difficulties related to isolation of RNA from FFPE tissue. This is a significant shortcoming, especially in pediatric DTC, since previous studies have shown high rates of these translocations. However, a large sample of pediatric DTC was comprehensively screened for the somatic single point mutations, including the recently described TERT promoter mutations and the rarely if ever investigated mutations in pediatric DTC (i.e., PIK3CA and PTEN mutations). Conventional Sanger sequencing was used, although there is recent trend to use high-throughput next-generation sequencing (NGS). However, the large number of gene variants identified with NGS makes it in part difficult to determine their significance. Sanger sequencing is considered a gold-standard method when specific genes/mutations are being investigated such as in this study. Despite the fact that this series is one of the largest series of pediatric DTC in which somatic mutations have been studied, it remains relatively small for analyzing potential correlations between these mutations and the histopathological features and outcomes of pediatric DTC. This was only possible for the BRAFV600E mutation but not for other genetic mutations, which occurred rarely.
In summary, the present study shows that the rate of the BRAFV600E mutation is much lower in pediatric DTC compared with the rates reported in adult DTC, and there is no association between this mutation and the histopathological features and outcomes of PTC. TERT C228T , NRAS 61, PIK3CA, and PTEN mutations are rare in pediatric DTC and are mutually exclusive of each other. Collectively, these findings strongly support the notion that pediatric DTC is distinct from adult DTC, not only in its clinical and histopathological features, but also in its molecular and biological profiles.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of Research Centre Administration of the King Faisal Specialist Hospital and Research Centre and the staff of the Department of Molecular Oncology.
Author Disclosure Statement
The authors have nothing to disclose.