
Abstract
Background:
For patients with lung metastases of differentiated thyroid carcinoma (DTC), there is no consensus on the maximal size of metastatic lesions to use when determining the intensity of follow-up and additional therapeutic options. This study evaluated the clinical outcomes and survival of patients with metastatic DTC confined to the lung, using the maximal diameter of lung lesions in the initial computed tomography.
Methods:
This retrospective cohort study included 112 DTC patients with metastases confined to the lung. The clinical responses were evaluated according to changes in the serum levels of stimulated thyroglobulin or antithyroglobulin antibody, disease status was evaluated according to radiological findings, progression-free survival (PFS), and cancer-specific survival (CSS).
Results:
Macronodular lung metastases (≥1 cm) were observed in 27 (24%) patients, and these patients had significantly poor biochemical responses and disease status (p < 0.001, and p < 0.001, respectively), irrespective of radioactive iodine (RAI) avidity. After adjusting for age, sex, primary tumor size, extrathyroidal invasion, cervical lymph node metastasis, time of lung metastasis, and RAI avidity, the macronodular group also had shorter PFS and CSS (p = 0.009 and p = 0.03, respectively) than the micronodular group. From the multivariate analyses, RAI avidity was not an independent prognostic factor predicting PFS and CSS. In the subgroup analyses, RAI avidity was a significant prognostic factor associated with better PFS and CSS (p = 0.013 and p = 0.021, respectively) in the micronodular group only.
Conclusions:
The initial largest diameter of metastatic lesions is the most important prognostic factor for predicting poor clinical outcomes and survival in patients with metastatic DTC confined to the lung.
Introduction
T
The survival and prognosis of patients with metastatic DTC depend on several clinicopathologic factors, including pathological subtype, the number and distribution of metastatic sites (e.g., brain, bone, lung), tumor burden, age, and RAI avidity (12,13,16,17). In patients with LM, the size of metastatic lesions as measured by chest computed tomography (CT) may also be an important prognostic factor, and lesions of sub-centimeter size are associated with a better prognosis (4,18,19). A recent study proposed that the course of LM varies from rapid progression (disease progression in less than a year) to slow progression (progression over five or more years) (19). However, previous studies have included patients with various metastases, including those in the lung, bone, and other organs (4,18 –21). Hence, the results of such studies may not be valid in all cases because patients have different clinical features depending on the site of metastasis.
The current study evaluated the clinical outcomes and survival of patients with metastatic DTC confined to the lung according to the maximal diameter of lesions in the initial chest CT. It also evaluated the relative importance of prognostic factors, including RAI avidity, for predicting the survival of these patients at the time of diagnosis. The results, which are confined to cases of LM, may provide relevant information on parameters when determining the strength of follow-up and when considering additional therapeutic options.
Materials and Methods
Patients
Data from 190 patients (age >18 years) who had been diagnosed with LM-DTC (either at the time of initial diagnosis, during treatment, or at any time during follow-up) between 1995 and 2012 at Asan Medical Center (Seoul, Korea) were retrospectively reviewed. Of these, 161 patients who had undergone total thyroidectomy followed by high-activity RAIT and who had been under regular follow-up were included. A further 49 patients were excluded because 42 had DM in other organs, and seven had undergone metastasectomy for LM or had been treated with chemotherapy or molecular-targeted therapy, leaving 112 LM-DTC patients (including eight patients with microcarcinoma) in the present study. The study protocol was approved by the Institutional Review Board at Asan Medical Center. The Tumor, Lymph Node, Metastasis (TNM) classification system of the American Joint Committee on Cancer and the Union for International Cancer Control was used for pathological staging.
Diagnosis of lung metastases
The diagnosis of LM-DTC was according to clinical assessments, including the presence of RAI uptake in the lungs in diagnostic or therapeutic 131I whole-body scans (WBSs), chest CT, chest X-ray, 18F-fluorodeoxyglucose-positron emission tomography with CT (PET-CT), and/or pathological confirmation of lung nodules. WBS images were reviewed by two experienced nuclear medicine specialists. Synchronous LM was diagnosed in 90 patients, and metachronous LM was detected in the remaining 22 patients over a median follow-up of 8.6 years.
Classification of lung metastases according to the initial maximal size of lung lesions and RAI avidity
According to the initial chest CT findings, patients were classified as having micronodular LM when all metastatic nodules were <1.0 cm in diameter, and macronodular LM when any nodule was ≥1.0 cm in diameter. Twenty-four patients in the micronodular group had a normal chest CT without visible lung lesions. Lung metastases in these patients were confirmed by abnormal RAI uptake in WBS and/or single-photon emission CT (SPECT)-CT after excluding physiological uptake and contamination. All these patients had elevated stimulated thyroglobulin (sTg) levels without evidence of cervical lymph node metastasis and DM to other organs. Patients with visible RAI uptake in the lungs according to WBS were categorized as having RAI-avid LM; those without it or with uptake in <10% lung nodules were categorized as having RAI non-avid LM (19).
Thyroid function tests, serum levels of Tg, and antithyroglobulin antibodies
Thyrotropin (TSH) was stimulated in all patients by withdrawing thyroid hormone. When TSH levels were >30 mIU/L, serum free thyroxine (T4), TSH, sTg, and antithyroglobulin antibody (TgAb) levels were measured, as described previously (22). Briefly, serum Tg levels were measured using a Tg-plus RIA kit (Brahms AG, Hennigsdorf, Germany) with a functional sensitivity (20% interassay variation coefficient) of 0.2 ng/mL. Serum TgAb levels were measured with an anti-Tg RIA kit (Brahms AG) with a functional sensitivity (20% interassay variation coefficient) of 0.07 ng/mL. The status of TgAb was defined as positive when its level was >100 IU/mL (22).
Treatment and follow-up protocols
Patients who were not diagnosed with LM before the initial treatment underwent RAIT with 2.77–5.55 GBq (75–150 mCi) according to their initial pathological staging. A high fixed activity of 131I (7.4 GBq, 200 mCi) was administered to patients who were diagnosed with LM before the initial treatment. High-activity RAIT was usually performed over a 12-month interval. Generally, repeated RAIT was continued until abnormal RAI uptake disappeared as assessed by post-therapeutic or diagnostic WBS. The physicians also determined additional RAIT according to the clinical situations and cumulative RAI activities. Patients underwent RAIT after thyroxine withdrawal for five to six weeks, and serum levels of sTg/TgAb were then measured. All patients were treated with levothyroxine to suppress TSH and then regularly followed up with physical examinations, thyroid function tests, and measurements of Tg/TgAb serum levels every three to six months as previously described (22). Additional diagnostic imaging tests such as chest X-ray and chest CT were performed every 6–12 months, as needed.
Definitions of biochemical responses
After at least one course of RAIT, biochemical responses were defined according to dynamic changes in the serum levels of sTg or TgAb as follows: effective (≥25% decrease in sTg levels from baseline in patients with negative TgAb or ≥50% decrease in TgAb levels in patients with positive TgAb); stable (<25% change in sTg levels or <50% change in TgAb levels, respectively); or ineffective (≥25% increase in sTg levels or ≥50% increase in TgAb levels, respectively).
Definition of disease status during follow-up
For patients with macronodular LM, disease status was classified according to the Response Evaluation Criteria in Solid Tumors (RECIST v1.1) (23). For patients with micronodular LM, disease status was classified using criteria from a previous study (19). No evidence of disease (NED) was defined as no visible lesions in radiological imaging, no detectable RAI uptake in WBS, undetectable serum levels of sTg in patients with negative TgAb, or negative conversion of serum levels of TgAb in patients with positive TgAb. Stable disease (SD) was defined when the maximal diameter of lung nodules changed by <5 mm and <20%, and no new metastatic foci were detected in radiological imaging, regardless of changes in sTg or TgAb levels. Progressive disease (PD) was defined as ≥20% increase (at least 5 mm) the maximal diameter of lung nodules compared with the baseline, and/or new metastatic foci were identified in the lung and/or in other distant organs. Neither an increase in Tg nor an increase in TgAb level was considered as disease progression.
Definition of progression-free survival and cancer-specific survival
Progression-free survival (PFS) was defined as the time from the diagnosis of LM until the identification of PD. Cancer-specific survival (CSS) was defined as the time from the diagnosis of LM until the last follow-up or death from DTC progression.
Statistical analysis
All statistical analyses were conducted using R v3.10 (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline clinicopathologic characteristics of the study patients
The baseline clinicopathologic characteristics of the study patients are shown in Table 1. According to the initial maximal diameter of metastatic lesions, 85 (76%) patients were classified into the micronodular group, and 27 (24%) were classified into the macronodular group. The mean age at diagnosis of LM was 47.6 ± 16.1 years. Patients in the macronodular group (61.8 ± 11.4 years) were significantly older than those in the micronodular group (43.1 ± 14.8 years; p < 0.001). There was a significantly higher proportion of men in the macronodular group (56%) than in the micronodular group (28%; p = 0.012). The main pathological subtype in both groups was classical papillary thyroid carcinoma (PTC). In the micronodular group, 77 (91%) patients had classical PTC, two (2%) had follicular thyroid carcinoma (FTC), five (6%) had follicular variant-PTC, and one (1%) had another variant of PTC. In the macronodular group, 23 (85%) had classical PTC, three (11%) had FTC, and one (4%) had another variant of PTC. There were no significant differences in primary tumor size, rate of cervical lymph node metastasis, cases with lymphovascular invasion, median RAIT number, median initial RAI activity, median cumulative RAI activity, or initial sTg levels between the two groups. RAI-avid LM was significantly more frequent in the micronodular group (72%) than it was in the macronodular group (26%; p < 0.001).
The percentages of subject numbers are presented in parentheses, unless otherwise stated. Statistically significant values are shown in bold.
PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; FV-PTC, follicular variant PTC; LN, lymph node; RAI, radioactive iodine; sTg, stimulated thyroglobulin; IQR, interquartile range.
Biochemical response and disease status according to micronodular and macronodular lung metastases
Biochemical responses according to the serum levels of sTg or TgAb were significantly different between the micronodular and macronodular groups (p < 0.001; Fig. 1A). In the micronodular group, RAIT was effective in 62/85 (73%) patients, and ineffective in only 11 (13%) patients. However, in the macronodular group, RAIT was effective in 7/27 (26%) patients, and ineffective in 12 (44%) patients. The disease status of LM was compared between the two groups over a median of 7.9 years of follow-up after LM diagnosis (Fig. 1B). In the micronodular group, at last follow-up, 13 (15%) patients were classified as having NED, 53 (62%) as having SD, and 19 (23%) as having PD. In the macronodular group, no cases were classified as having NED, seven (26%) as having SD, and 20 (74%) as having PD. There was a significant difference in disease status between the two groups according to repeated RAIT (p < 0.001).
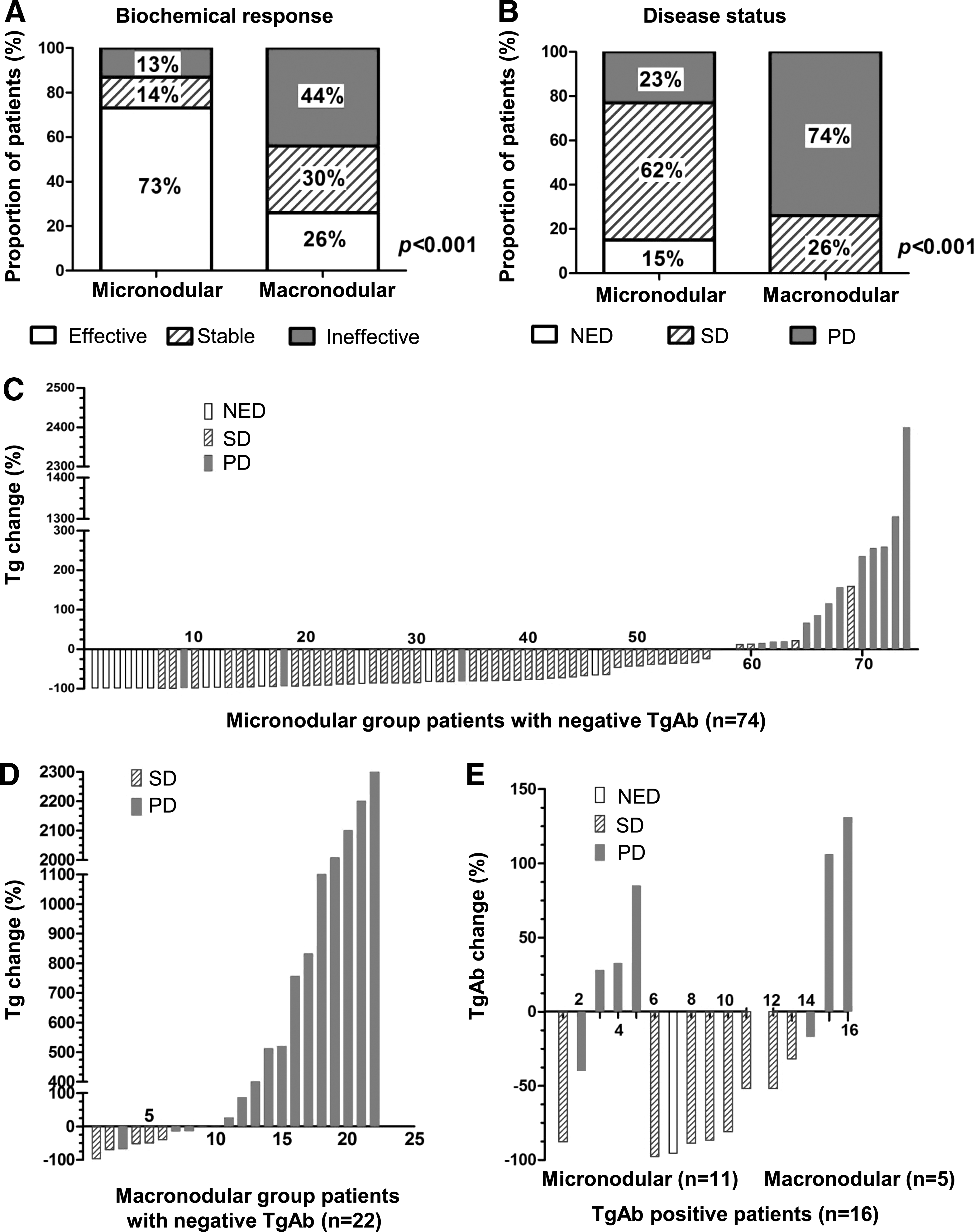
Clinical outcomes of the study patients with lung metastases from differentiated thyroid carcinoma (DTC) according to the initial maximal diameter of the metastatic lesions. The biochemical response
Sixteen of 23 (70%) patients and 19 of 20 (95%) patients without effective biochemical responses (including stable and ineffective cases) showed structural disease progression in the micronodular and macronodular groups, respectively. In addition, 3/62 (5%) patients and 1/7 (14%) patients were classified as having PD, despite having effective biochemical responses in the micronodular and macronodular groups, respectively (Fig. 1C–E).
Survival analysis according to micronodular and macronodular lung metastases
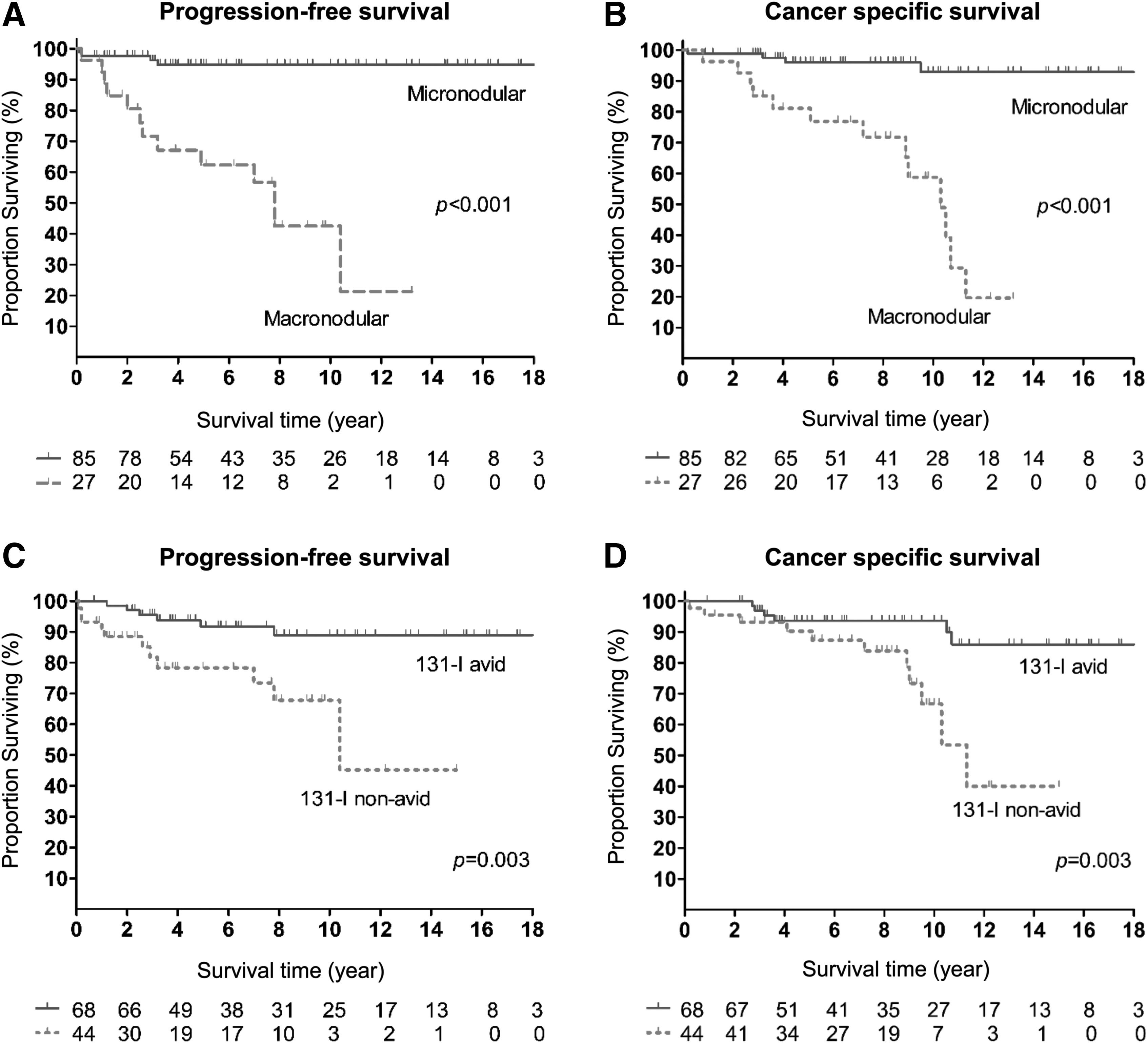
PFS (Fig. 2A) and CSS (Fig. 2B) were significantly shorter in the macronodular group than they were in the micronodular group (p < 0.001 and p < 0.001, respectively). Patients with RAI non-avid LM had significantly shorter PFS (Fig. 2C) and CSS (Fig. 2D) than those with RAI-avid metastasis (p = 0.003 and p = 0.003, respectively). From the univariate analyses, PFS was also significantly shorter in older patients (≥45 years) and those with larger primary tumors of >4 cm in size (p = 0.005 and p = 0.021, respectively; Supplementary Table S1 and Supplementary Fig. S1; Supplementary Data are available online at
Progression-free survival
From the multivariate analyses, macronodular LM was found to be an independent prognostic factor associated with shorter PFS after adjustments for age, sex, primary tumor size, extrathyroidal extension, cervical lymph node metastasis, onset time of LM, and RAI avidity (HR = 9.19 [CI 1.75–48.36], p = 0.009; Table 2). Macronodular LM was also a significant prognostic factor associated with shorter CSS in the multivariate analyses (HR = 6.74 [CI 1.22–37.37], p = 0.03; Table 2).
Model 1 is adjusted for age and sex. Model 2 is adjusted by Model 1, tumor size, extrathyroidal extension, and cervical lymph node metastasis. Model 3 is adjusted by Model 2 and onset of lung metastasis. Model 4 is adjusted by Model 3 and RAI avidity. p-Values were calculated using a Cox proportional hazard model. Statistically significant values are shown in bold.
DTC, differentiated thyroid carcinoma; PFS, progression-free survival; CSS, cancer-specific survival; HR, hazard ratio; CI, confidence interval.
Survival analysis according to RAI avidity
The association between RAI avidity and survival was also evaluated using multivariate analyses (Table 3). In the unadjusted model, RAI non-avid LM was associated with significantly shorter PFS (HR = 4.18 [CI 1.52–11.47], p = 0.005) and shorter CSS (HR = 4.22 [CI 1.51–11.78], p = 0.006). However, after adjusting for age, sex, tumor size, extrathyroidal invasion, cervical lymph node metastasis, onset time of LM, and the maximal diameter of lung nodules, there were no significant associations between RAI avidity and PFS (HR = 1.05 [CI 0.24–4.64], p = 0.946, Model 5) or CSS (HR = 1.14 [CI 0.26–5.10], p = 0.858, Model 5). RAI non-avid LM was not an independent prognostic factor predicting shorter PFS and CSS in the multivariate analyses.
Model 1 is adjusted for age and sex. Model 2 is adjusted by Model 1, tumor size, extrathyroidal extension, and cervical lymph node metastasis. Model 3 is adjusted by Model 2 and onset of lung metastasis. Model 5 is adjusted by Model 3 and maximal diameter of lung nodules. p-Values were calculated using a Cox proportional hazard model. Statistically significant values are shown in bold.
Clinical outcomes according to RAI avidity in the micronodular and macronodular groups
To evaluate the clinical importance of RAI avidity in each group, subgroup analyses were performed. In the micronodular group, RAI non-avid LM was significantly associated with poor biochemical responses (p < 0.001; Fig. 3A) and disease status (p < 0.001; Fig. 3B). RAI avidity was a significant prognostic factor associated with better PFS (p = 0.013; Fig. 3C) and CSS (p = 0.021; Fig. 3D) only in patients with micronodular LM. In the macronodular group, RAI avidity was not associated with biochemical responses (p = 0.394; Fig. 3E) or disease status (p = 0.99; Fig. 3F). Further, RAI avidity was not associated with longer PFS (p = 0.391; Fig. 3G) or longer CSS (p = 0.629; Fig. 3H) in patients with macronodular LM.
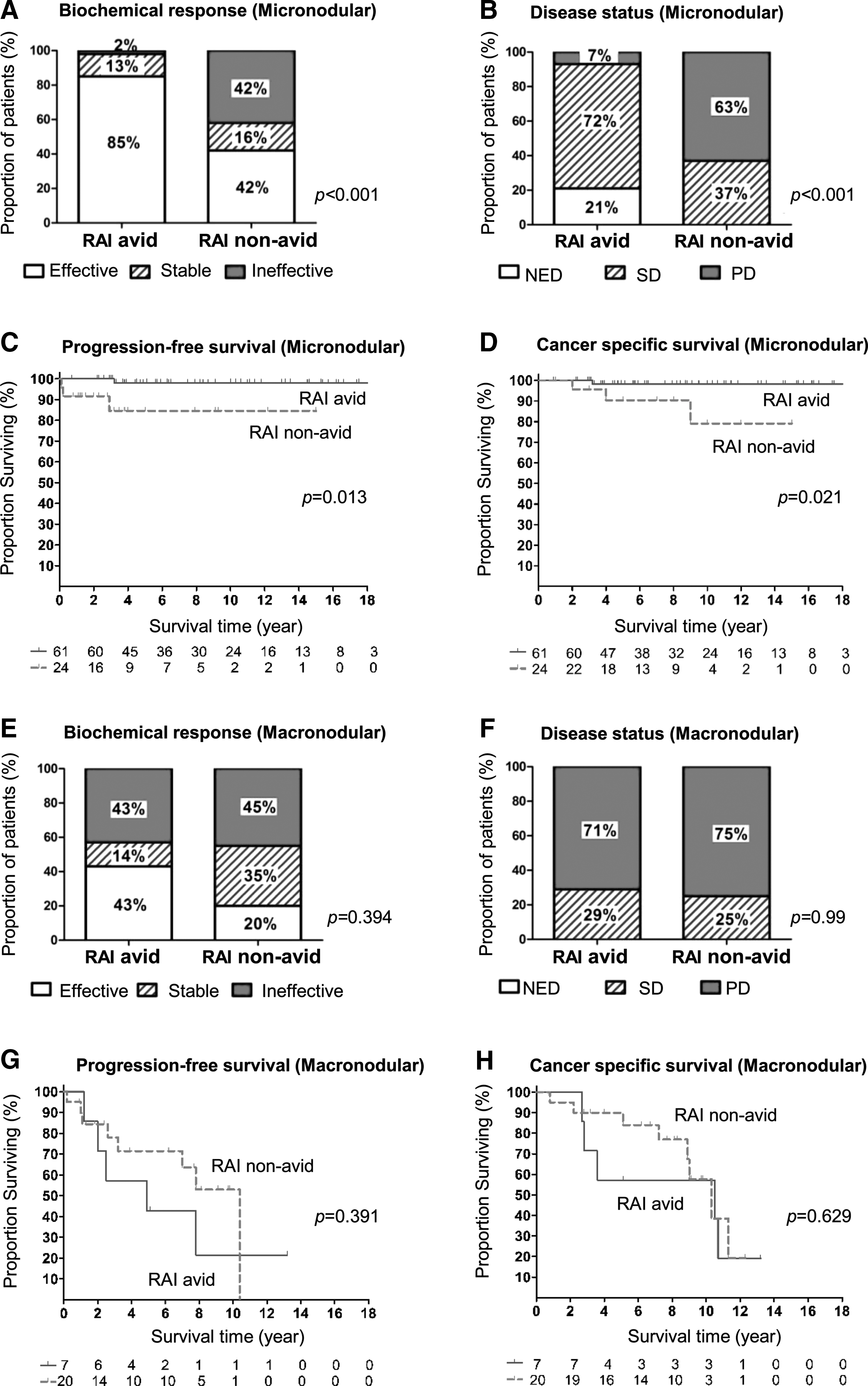
Clinical outcomes of the study patients with lung metastases in the micronodular and macronodular groups according to the RAI avidity. Biochemical response
Discussion
In the current study, patients with macronodular LM-DTC had a significantly compromised biochemical response and disease status after RAIT, irrespective of RAI avidity. Patients with macronodular LM also had a poorer PFS and CSS than those with micronodular LM. As such, the maximal size of metastatic lung lesions as measured by the initial chest CT at the diagnosis of LM is the best prognostic indicator of disease progression and survival in patients with LM. A recent study proposed that the course of LM varies from rapid progression to slow progression, as detailed above (19). However, establishing the rate of disease progression on the basis of follow-up images usually requires long follow-up periods, in most cases with LM arising from DTC. Consequently, the opportunity to treat patients with more effective targeted agent therapy could be lost (11,14). Thus, it is necessary to customize the follow-up intervals for individual patients according to the expected disease course. The results of the present study suggest that short-term chest CT follow-ups should be performed in patients with macronodular LM, and additional therapeutic options should be considered earlier rather than repeated RAIT if any disease progression is detected in such cases. If it can be demonstrated through further clinical studies, re-differentiation therapy to enhance RAI uptake may be preferentially considered in patients with macronodular LM (24,25).
Many previous studies have shown that RAI avidity is an independent factor predicting a better prognosis (4,10,18). However, in contrast to previous reports, the current analysis found that RAI non-avid LM was significantly associated with poor clinical outcomes and survival in the micronodular group only. RAI avidity of LM is partially associated with the size of metastatic lung nodules (26). In addition, the efficacy of RAIT in patients with larger metastatic lesions is considerably low, regardless of RAI avidity (27). Therefore, the size of the largest metastatic lung lesion should be considered when determining whether to start targeted agents in patients with RAI-refractory LM.
In the present study, receiver operating characteristic curve analysis was performed to determine the optimal cutoff value of the size of the initial largest metastatic lung lesion for predicting CSS (Supplementary Fig. S3). The area under the curve was 0.857, and the most reliable cutoff value was 1.0 cm, with 76.5% sensitivity and 87.8% specificity (p < 0.001). This cutoff value of 1.0 cm was consistent with the criterion that was used for dividing the LM-DTC patients into the micronodular and macronodular groups.
Unlike previous studies, DTC patients with DM in other organs besides the lungs were excluded. This was done because metastatic disease at multiple sites is associated with a poorer prognosis than metastasis confined to the lung is (5,8,28 –31). The 10-year survival rate of LM-DTC patients ranges from 60% to 85%, whereas that of patients with bone metastasis ranges from 13% to 21% (3 –6,8,32). Survival after the diagnosis of brain metastasis from DTC is generally less than a year (33). High-activity RAIT is not a main therapeutic modality in patients with bone and/or brain metastases of DTC (20,28,30), and management of these patients should involve a multidisciplinary approach consisting of bisphosphonate, radiotherapy, metastasectomy, and RAIT (21,30,34,35). Therefore, the results of the current study are very important for evaluating the relative significance of prognostic factors for predicting clinical outcomes and survival in patients with metastatic DTC confined to the lung.
Biochemical responses, which were defined as dynamic changes in the serum levels of sTg or TgAb, showed a high agreement with disease status defined as structural disease progression. In fact, 80% (28/35) of the study patients whose sTg levels increased ≥25% showed structural disease progression. This result supports previous findings that changes in the serum levels of sTg are a prognostic indicator for assessing the efficacy of RAIT for DTC patients with LM in the absence of TgAb interference (18,36). In a previous study, it was demonstrated that sustained positive TgAb levels or increasing TgAb concentrations could be evidence of recurrent or persistent disease and may be prognostic indicators of poor outcome in patients with undetectable Tg values (37). This finding was supported by the fact that all patients with positive TgAb and those in whom TgAb levels increased by ≥50% showed structural disease progression. In the present study, dynamic changes in the serum levels of sTg or TgAb were particularly valuable when patients with DM in other organs besides the lungs were excluded.
In this study, the definition of NED considered both absence of radiological evidence of disease and biochemical evidence of an undetectable serum sTg levels. This definition is quite strict, and only 15% patients with micronodular LM achieved NED after RAIT. It appears that a smaller proportion of patients benefited from RAIT compared with previous studies (3,9). However, this finding was mainly derived from the difference in the definitions used in the studies. Previous studies included patients with detectable but low serum sTg after treatment for the definition of NED because those low sTg levels have little prognostic relevance and they may normalize with time (10,38).
The current study has several limitations. First, it was affected by the limitations inherent to studies with a retrospective design. In addition, only patients from a single tertiary referral center were enrolled, and a relatively limited number of study subjects were included. Nonetheless, this is an important study for evaluating clinical outcomes by assessing the changes in the serum levels of sTg and TgAb as well as PFS and CSS of DTC patients with metastasis in the lung only, according to the maximal size of the metastatic lesions. The results highlight the relevance of stratifying the mortality risk of DTC patients with LM according to the initial size of lung lesions.
In conclusion, the initial largest diameter of metastatic lesions in the lung is the most important prognostic factor for predicting poor clinical outcomes and poor survival in patients with metastatic DTC confined to the lung. RAI avidity was not an independent prognostic factor predicting PFS and CSS in multivariate analyses in patients with macronodular LM. RAI avidity was a significant prognostic factor associated with longer PFS and CSS only in the micronodular group. The efficacy of repeated high-dose RAIT to improve survival of patients with macronodular lung metastases should be evaluated in future studies. The findings suggest that short-term chest CT follow-up should be performed, and other therapeutic options such as TKIs should be considered earlier if any disease progression is detected in patients with macronodular LM, rather than repeating RAIT, even if the metastatic lesions are RAI avid.
Footnotes
Acknowledgments
This study was supported by a National Research Foundation (NRF) of Korea Research Grant (NRF-2015R1D1A1A09057966). A part of this study was presented as a poster at the Endocrine Society's 98th annual meeting in Boston, MA.
Author Disclosure Statement
The authors have nothing to disclose.