
Abstract
Background:
The presence of a telomerase reverse transcriptase (TERT) promoter mutation has been suggested as a potential prognostic marker for thyroid cancer, and a synergistic association with the BRAFV600E mutation has been demonstrated. The aim of this study was to verify the role of this genetic duet in papillary thyroid cancer (PTC).
Methods:
Studies of the association of BRAFV600E and TERT promoter mutations with clinicopathologic features, recurrence, or PTC-related mortality were included from PubMed and Embase databases (inception to September 2016).
Results:
Thirteen eligible studies incorporating 4347 patients with PTC were included, and 283 (median 8.3%) of these patients had coexistent BRAFV600E and TERT promoter mutations. The coexistence of the two mutations was far more strongly associated with high-risk clinicopathologic features than either mutation alone was, including advanced TNM stage (vs. BRAFV600E : odds ratio [OR] = 4.19 [confidence interval (CI) 3.07–5.71]; vs. TERT: OR = 4.66 [CI 2.67–8.13]), extrathyroidal extension (vs. BRAFV600E : OR = 3.1 [CI 2.2–4.37]; vs. TERT: OR = 5.66 [CI 3.02–10.6]), lymph node metastasis (vs. BRAFV600E : OR = 1.59 [CI 1.16–2.17]; vs. TERT: OR = 2.03 [CI 1.22–3.38]), and distant metastasis (vs. BRAFV600E : OR = 11.76 [CI 5.63–24.58]). The coexistence of the mutations showed the highest risk of recurrence (coexistence vs. no mutations: hazard ratio [HR] = 6.60 [CI 3.82–11.40]; BRAFV600E vs. no mutations: HR = 1.31 [CI 0.49–3.46]; TERT vs. no mutations: HR = 3.38 [CI 0.85–13.35]). Moreover, PTC-related mortality was significantly higher with coexistent mutations than in the presence of BRAFV600E alone (HR = 20.07 [CI 8.37–48.09]).
Conclusions:
Coexistent BRAFV600E and TERT promoter mutations have a synergistic effect on clinical outcomes in PTC, whereas each mutation alone has a modest effect. Therefore, molecular testing of BRAFV600E and TERT promoter mutations together is useful in assessing risk stratification of PTC.
Introduction
T
Several molecular markers have been studied to identify potential prognostic markers, and an association between the BRAFV600E mutation and poor prognosis of PTC has been demonstrated (8 –10). However, owing to its high prevalence in PTC, clinical application of the BRAFV600E mutation has limitations, especially in areas where the mutation is very prevalent (11 –13). Recently, a telomerase reverse transcriptase (TERT) promoter mutation has been proposed as a strong prognostic biomarker (14), and meta-analyses have demonstrated an association between the TERT promoter mutation and aggressive clinicopathologic characteristics (15,16). In 2014, Xing et al. first demonstrated a synergistic role of BRAFV600E and TERT promoter mutations in the aggressive features and recurrence of PTC (17) and PTC-related mortality (18). Since then, the concept of the role of this genetic duet on the prognosis has drawn great attention (19) and prompted subsequent studies. Remarkably, although it was reported that the TERT promoter mutation without the presence of a BRAFV600E or RAS mutation did not increase the risk of recurrence or mortality in PTC, the risk effect of the TERT mutation was observed when BRAFV600E or RAS mutations coexisted (17,20). Additionally, as a potential mechanism of their synergistic effect on prognosis, it was proposed that BRAFV600E leads to overexpression of TERT by upregulation of the E-twenty six (ETS) transcription factor through activation of the mitogen-activated protein (MAP) kinase pathway (16). However, the mechanism of this synergy has not been elucidated. Moreover, the effect of this coexistence on clinicopathologic characteristics is inconclusive because most studies did not provide data on both the TERT promoter mutation and BRAFV600E status.
Therefore, a comprehensive meta-analysis was performed to evaluate the synergistic effect of BRAFV600E and TERT promoter mutations on clinical outcomes in PTC.
Materials and Methods
Search strategy
A literature search was conducted from PubMed and Embase from inception to September 16, 2016. Two independent investigators (S.M. and Y.S.S.) selected articles with a combination of the following important terms: “TERT,” “TERT promoter,” “telomerase reverse transcriptase promoter,” “telomerase reverse transcriptase,” “mutation,” “mutations,” “thyroid,” “neoplasms,” “cancer,” “carcinoma,” and “tumor.” The language of the literature was limited to English.
Study selection
All articles were electronically downloaded and screened for inclusion by a two-step method. First, titles and abstracts were evaluated according to predefined criteria. Articles were excluded if: (i) it they did not report any clinical information of PTC subjects (e.g., sex, age, lymph node metastasis, extrathyroidal extension, disease stage, recurrence, or mortality); (ii) there was no information on any TERT promoter or BRAFV600E mutations; (iii) the study was published as a form of an abstract, an expert opinion, a letter, a conference article, or a review. Care was taken to avoid data extraction from duplicate articles. If studies had multiple reports, the latest or most complete article was enrolled. Then, full texts of the selected, potentially relevant articles were reviewed independently by the two investigators based on the criteria listed above. Any disagreements were resolved by a third investigator (Y.J.P.).
Data extraction
The following variables were extracted by the two investigators independently based on the same rules: first author, publication year, country, number of patients by each TERT promoter and BRAFV600E mutation, number of males or females, mean age at diagnosis, the TNM stages, lymph node metastasis, extrathyroidal extension, distant metastasis, recurrence, and mortality. Disagreements were discussed with the third investigator.
Data analyses and statistical methods
The pooled odds ratios (ORs) with confidence intervals (CIs) were calculated using the Mantel–Haenszel method, and the mean difference (MD) with CIs using inverse variance according to the Cohen method. Higgins' I
2 statistic was used to test for heterogeneity. When I
2 ≤50%, the included studies were considered to have little heterogeneity, and a fixed-effects model was used. When I
2 >50%, the heterogeneity was defined, and a random-effects model was used. Subgroup and sensitivity analyses were used to determine the cause of heterogeneity. The potential for publication bias was assessed using a funnel plot analysis. To examine the strength of the outcome, we conducted a sensitivity analysis to estimate the effects of the remaining studies without the larger one's effect. All statistical analyses were calculated by the statistical program R v3.1.0 (
Results
Characteristics of eligible studies
The literature search yielded 327 potentially relevant articles, of which 195 were screened for further review. Thirteen articles were ultimately selected for meta-analysis (17,20 –31). The detailed procedure of the study selection is summarized in Figure 1. In total, 4347 patients with PTC were enrolled in this analysis. Overall, 283 (median 8.3%; range 2.8–21.6%) of these patients had coexisting BRAFV600E and TERT promoter mutations. Sample sizes of these studies ranged from 51 to 1051 patients. Because several variables contained in each article were different, the meta-analysis was conducted using the relevant variables for each study. The examined variables of the selected studies are summarized in Table 1.
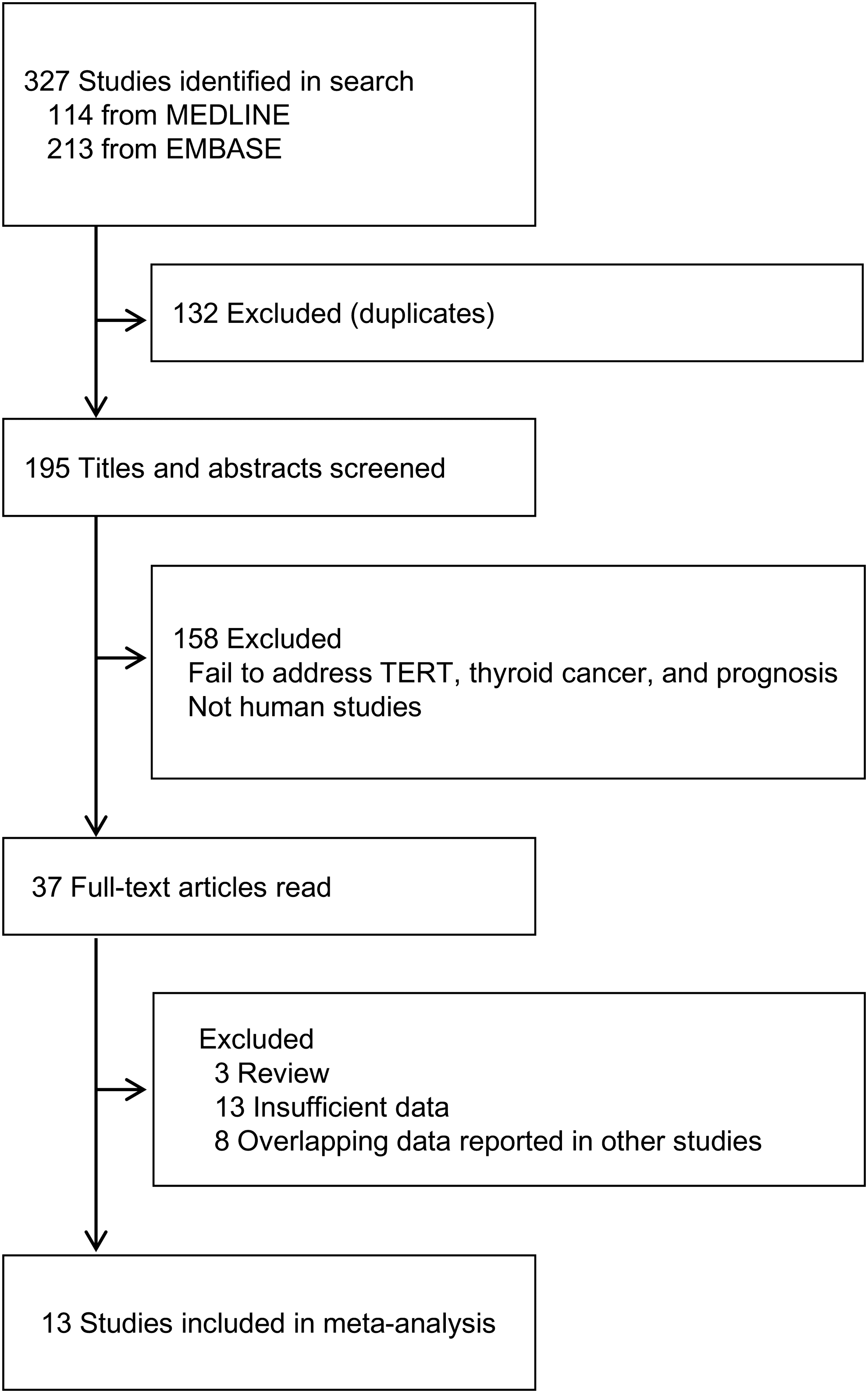
Representation of the search strategy.
These studies used the same database. Data including age, sex, lymph node metastasis, extrathyroidal extension, TNM stage, and mortality were extracted from Liu et al. Distant metastasis and recurrence data were extracted from Xing et al.
Data were extracted from The Cancer Genome Atlas Data Portal.
Y, the study was evaluated; N, the study was not evaluated.
Effect of BRAFV600E mutation alone over no mutation on clinicopathologic characteristics
Presence of a BRAFV600E
mutation alone was modestly associated with age at diagnosis (MD = 1.73 [CI 0.6–2.86]), advanced TNM stage (TNM stage III–IV: OR = 1.56 [CI 1.31–1.85]), extrathyroidal extension (OR = 2.45 [CI 1.99–3.03]), and lymph node metastasis (OR = 1.52 [CI 1.12–2.05]) compared with no mutation (Supplementary Fig. S1; Supplementary Data are available online at
Effect of the TERT promoter mutation over no mutation on clinicopathologic characteristics
In comparison with the group negative for either mutation, a TERT promoter mutation alone was not significantly associated with sex, advanced TNM stage, or extrathyroidal extension, while it was moderately associated with age at diagnosis (MD = 8.86 [CI 4.00–13.72]), lymph node metastasis (OR = 1.58 [CI 1.02–2.46]). In addition, a significantly higher risk for distant metastasis was found in patients with a TERT promoter mutation alone than in those without mutations (OR = 7.28 [CI 2.85–18.58]; Supplementary Fig. S2). No significant heterogeneity was found among these studies.
Effect of the coexistence of BRAFV600E and TERT promoter mutations over no mutations on clinicopathologic characteristics
The coexistence of BRAFV600E and TERT promoter mutations was significantly associated with age at diagnosis (MD = 16.18 [CI 13.84–18.52]), sex (OR for male = 2.33 [CI 1.71–3.15]), advanced TNM stage (OR = 7.51 [CI 5.38–10.48]), extrathyroidal extension (OR = 8.14 [CI 5.55–11.94]), lymph node metastasis (OR = 2.94 [CI 2.12–4.09]), and distant metastasis (OR = 8.36 [CI 4.13–16.95]) compared with no mutations (Supplementary Fig. S3). No significant heterogeneity was found among these studies.
Effect of the coexistence of BRAFV600E and TERT promoter mutations over BRAFV600E mutation alone on clinicopathologic characteristics
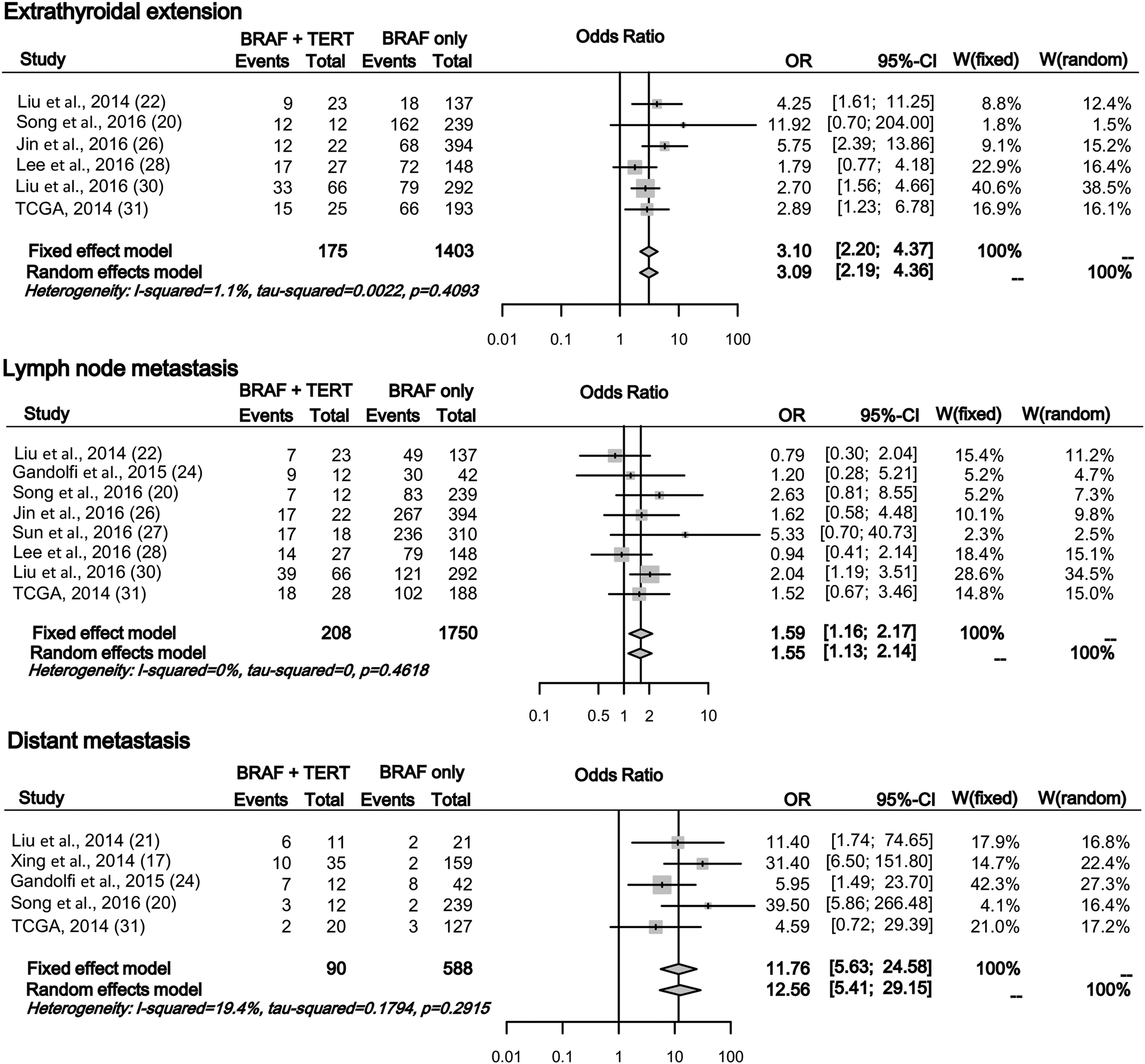
In comparison with a BRAFV600E mutation alone, the coexistence of BRAFV600E and TERT promoter mutations was significantly associated with all variables, including older age (MD = 14.50 [CI 12.24–16.75]), greater portion of male patients (OR = 1.93 [CI 1.44–2.58]), advanced TNM stage (OR = 4.19 [CI 3.07–5.71]), and higher risks of extrathyroidal extension (OR = 3.1 [CI 2.2–4.37]), lymph node metastasis (OR = 1.59 [CI 1.16–2.17]), and distant metastasis (OR = 11.76 [CI 5.63–24.58]; Fig. 2). No significant heterogeneity was found among these studies.
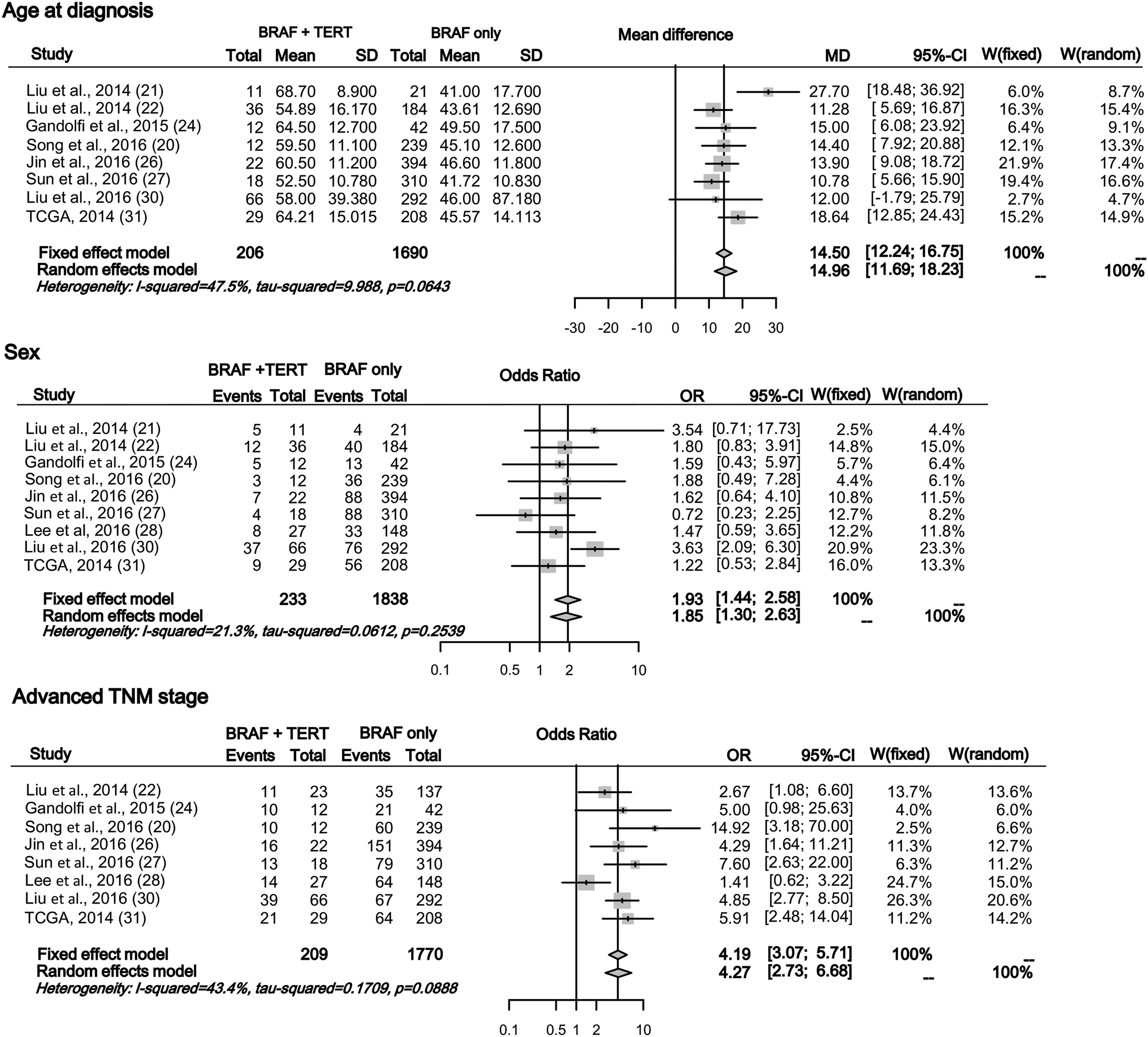
Effects of the coexistence of BRAFV600E and TERT promoter mutations over BRAFV600E mutation alone on clinicopathologic characteristics. The forest plot displays the effect size and confidence intervals (CIs) for each study and overall. TCGA, The Cancer Genome Atlas Data. Continued.
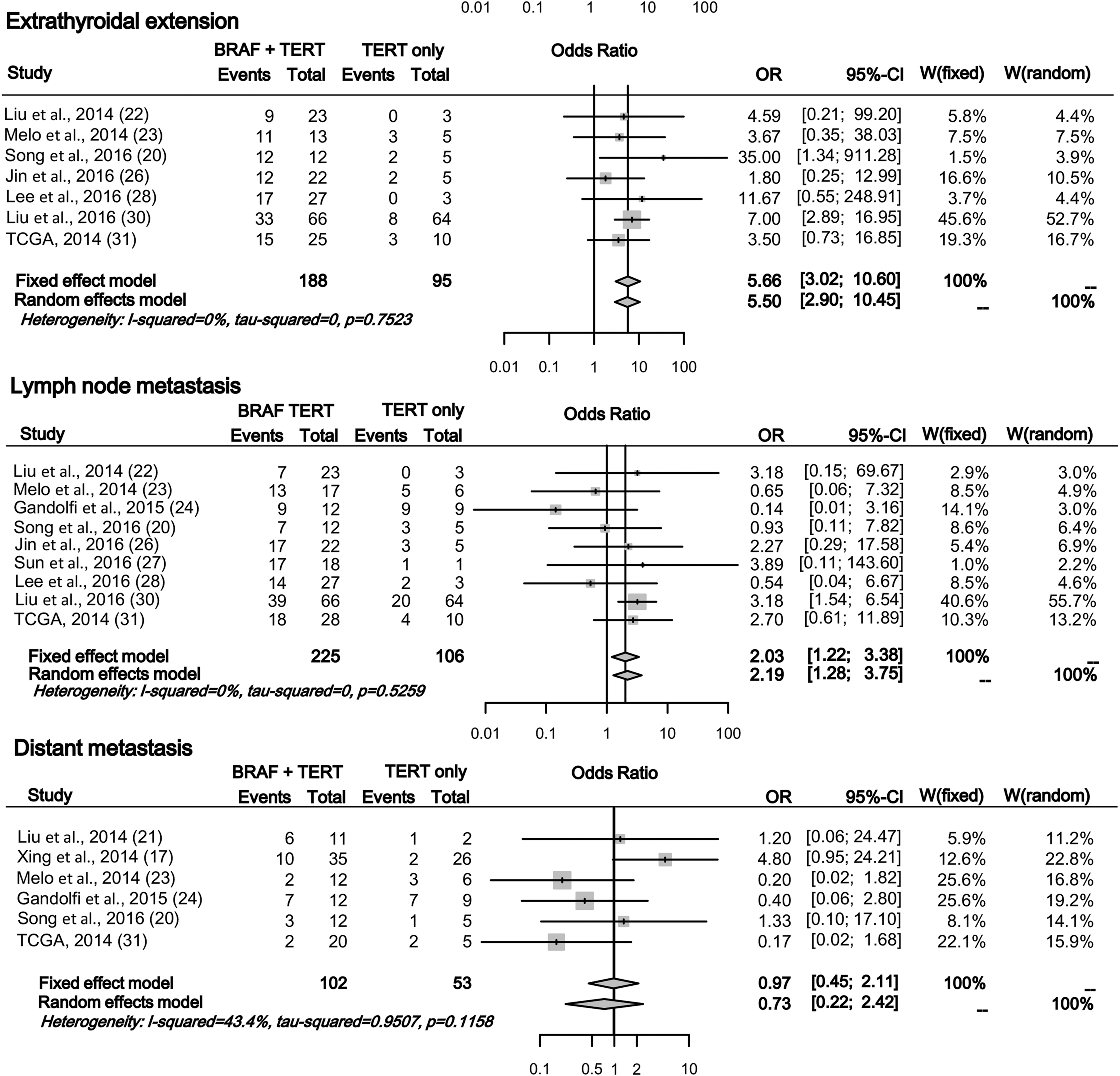
Effect of the coexistence of BRAFV600E and TERT promoter mutations over TERT promoter mutation alone on clinicopathologic characteristics
The coexistence of BRAFV600E and TERT promoter mutations was significantly associated with age at diagnosis (MD = 8.28 [CI 3.72–12.84]), sex (OR for male = 2.09 [CI 1.25–3.49]), advanced TNM stage (OR = 4.66 [CI 2.67–8.13]), extrathyroidal extension (OR = 5.66 [CI 3.02–10.6]), and lymph node metastasis (OR = 2.03 [CI 1.22–3.38]) compared with TERT promoter mutation alone. However, there was no significant difference in distant metastasis between the two groups (Fig. 3). No significant heterogeneity was found among these studies.
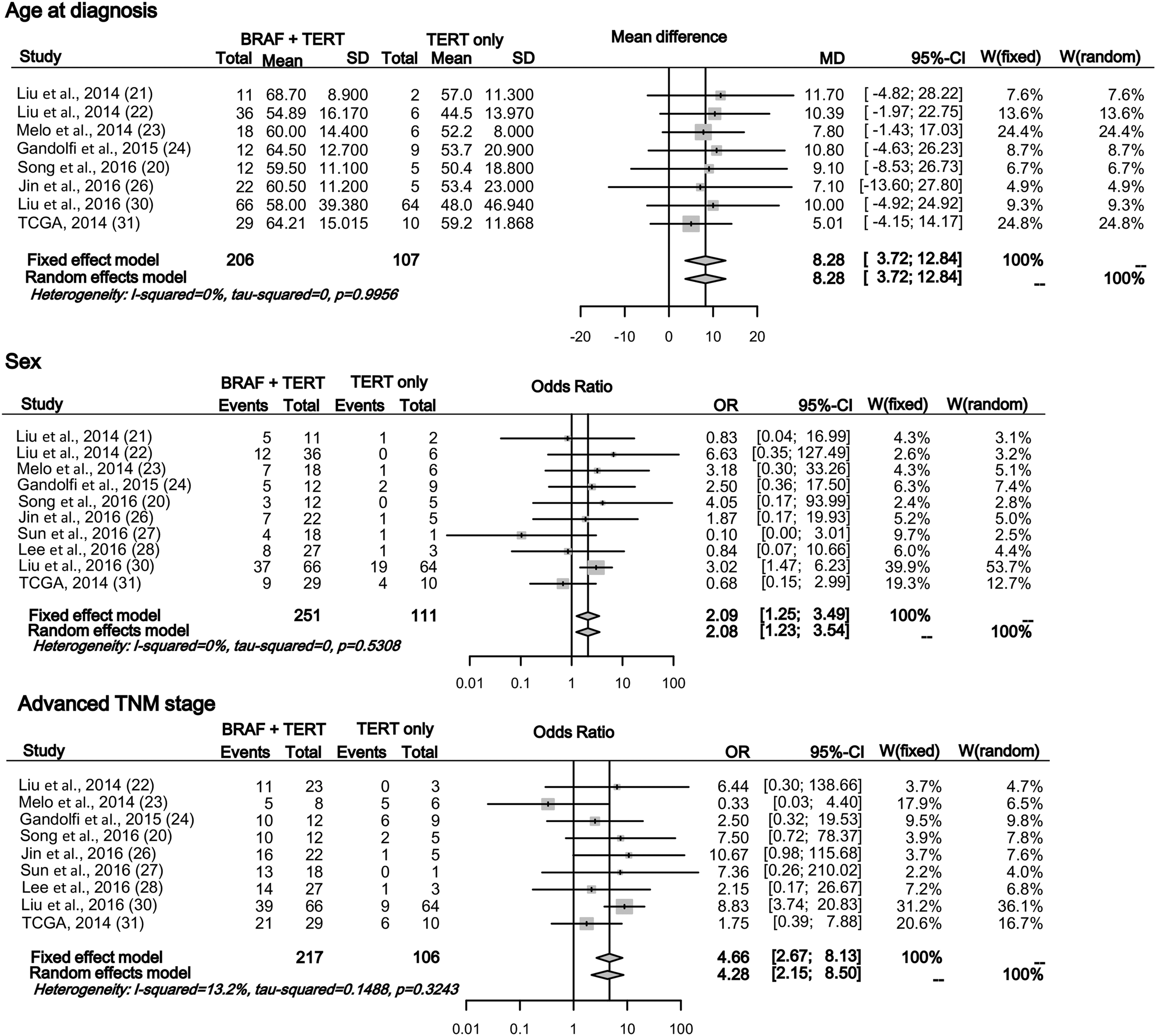
Effects of the coexistence of BRAFV600E and TERT promoter mutations over TERT promoter mutation alone on clinicopathologic characteristics. The forest plot displays the effect size and CIs for each study and overall. Continued.
Risk effects of the long-term outcomes of BRAFV600E mutation, TERT promoter mutation, or their coexistence
In comparison with the group negative for either mutation, the highest risk of recurrence of PTC was found in patients with a coexisting BRAFV600E and TERT promoter mutation after adjustment for age and sex (coexistence vs. no mutations: hazard ratio [HR] = 6.60 [CI 3.82–11.40]; BRAFV600E alone vs. no mutations: HR = 1.31 [CI 0.49–3.46]; TERT alone vs. no mutations: HR = 3.38 [CI 0.85–13.35]; Fig. 4). However, the effects of the coexistence of two mutations over either mutation alone on recurrence could not be analyzed because of limited data. In the analyses for PTC-related mortality risk, TCGA data (31) were excluded because they have all-cause mortality, and two studies (20,30) were included. The HR of the TERT promoter mutation alone group could not be derived, since only one study (30) had the events of death in that group. However, it was found that the coexistence of BRAFV600E and TERT promoter mutations had a significantly higher PTC-related mortality than no mutations or BRAFV600E alone did (coexistence vs. no mutations: HR = 9.38 [CI2.81–31.29]; BRAFV600E alone vs. no mutations: HR = 1.05 [CI 0.29–3.76]; coexistence vs. BRAFV600E alone: HR = 20.07 [CI 8.37–48.09]; Fig. 5). Moreover, to confirm the synergistic effect of the genetic duet on mortality, the ORs were further analyzed for mortality using five studies with PTC-related mortality rate (20,23,25,29,30). The coexistence of the two mutations was more strongly associated with high-risk mortality than either mutation alone, demonstrating a synergistic role of BRAFV600E and TERT promoter mutations (coexistence vs. BRAFV600E : OR = 17.46 [CI 8.20–37.18]; vs. TERT: OR = 2.81 [CI 1.17–6.76}; Supplementary Fig. S4).
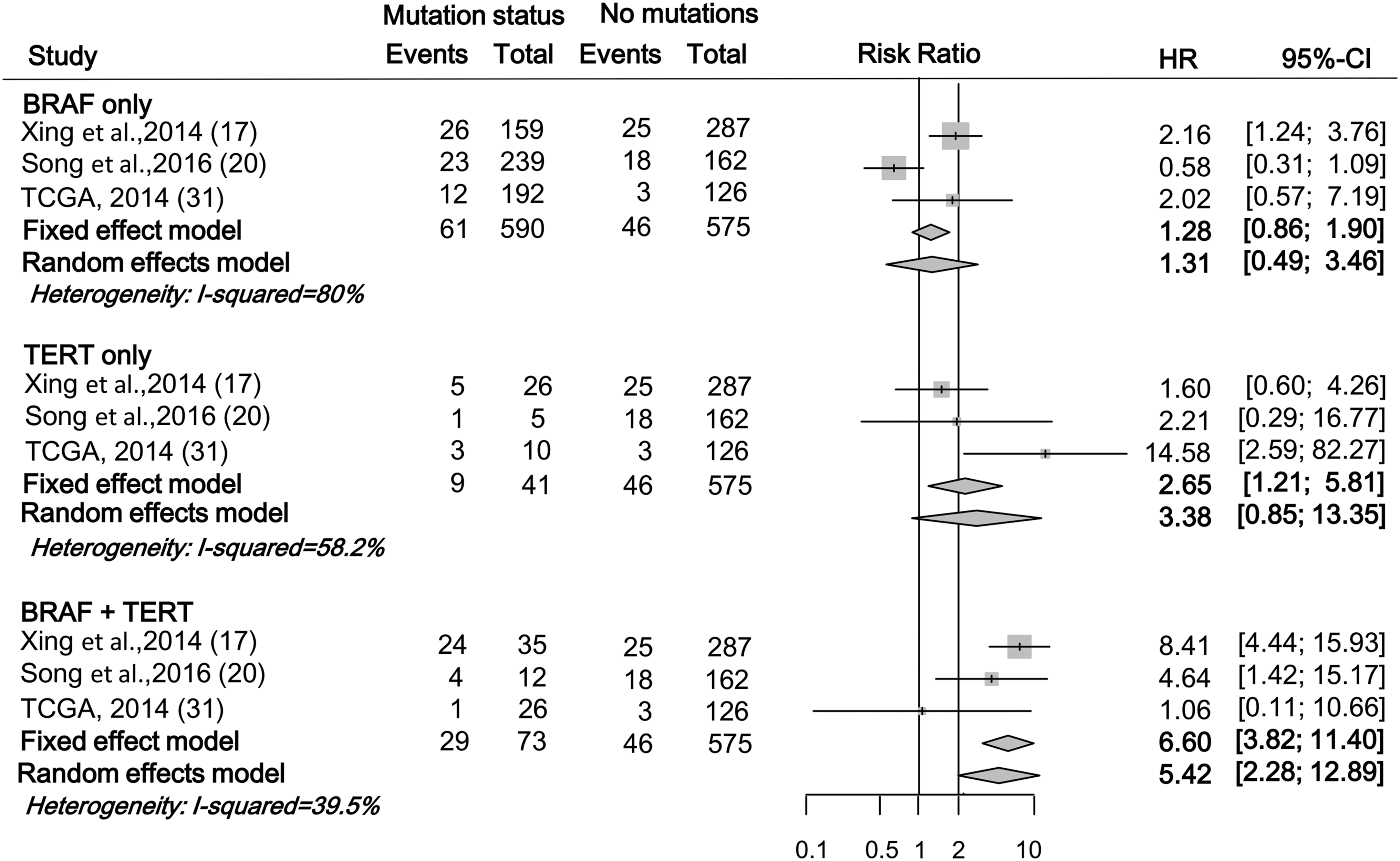
Forest plot showing individual and pooled hazard ratios of the recurrence of papillary thyroid carcinoma (PTC) in BRAFV600E or TERT promoter mutation or their coexistence in comparison to no mutations with the adjustment for age at diagnosis and sex.

Forest plot showing individual and pooled hazard ratios of PTC-related mortality in BRAFV600E mutation or the coexistence of BRAFV600E and TERT promoter mutations.
Discussion
To the best of the authors' knowledge, this study is the first meta-analysis investigating an association between the coexistence of BRAFV600E and TERT promoter mutations versus each mutation alone and the associated prognostic factors. The synergistic effects of coexisting BRAFV600E and TERT promoter mutations on poor clinical outcomes have been controversial because some studies did not show similar synergistic effects (23,24,32). However, this pooled analysis clearly demonstrates that the coexistence of BRAFV600E and TERT promoter mutations are far more strongly associated with poor clinicopathologic features and long-term outcomes than either BRAFV600E or TERT promoter mutation alone are in PTC. Especially considering the recent increase in studies that proposed the TERT promoter mutation as a significant prognostic molecular marker in PTC, the limited effect of the TERT promoter mutation alone was an unexpected finding. Most of these studies, however, presented the TERT promoter mutation without discriminating between the TERT promoter mutation alone compared to coexistence with a BRAFV600E mutation.
A positive association of TERT promoter mutations with BRAFV600E has been reported in previous studies, including a recently published meta-analysis (16). Likewise, in the present study, a TERT promoter mutation was found in 11.4% of patients with BRAFV600E (median 12.9%; range 4.8–34.4%) versus 6.3% of those without BRAFV600E (median 5.4%; range 0.9–14.3%; OR = 2.46 [CI 1.93–3.14]; I 2 = 0%; Supplementary Fig. S5). Considering the existence of such a high association of TERT promoter mutations with BRAFV600E and the limited effect of the TERT promoter mutation alone in this study, it is possible that the results of previous studies on the prognostic effects of the TERT promoter mutation in PTC reflect at least in some part the effects of the BRAFV600E mutation, as well as the true prognostic impact of the TERT promoter mutation. In addition, although data were limited, several studies also reported a positive relationship between TERT promoter and RAS mutations in thyroid cancer (20,23,32). Therefore, reevaluation of the effect of each mutation alone is needed for the risk stratification of thyroid cancer.
Recently, there have been several studies on the clinical meaning of the coexistence of the TERT promoter and BRAFV600E or RAS mutations, reporting that the coexistence of the two mutations was associated with more aggressive clinical outcomes than either mutation alone (13,17). Xing et al. reported that the coexistence of two mutations was far more strongly associated with high-risk factors, recurrence of PTC, or disease-specific mortality compared with groups with no mutations, a BRAFV600E mutation alone, or a TERT promoter mutation alone. BRAFV600E and TERT promoter mutations alone each had a modest effect (17,30). This meta-analysis fully confirms the findings of their study. Recently, similar results were also demonstrated, except for the negative prognostic role of the TERT promoter mutation alone, possibly because of the low frequency of the mutation in the study (20).
The mechanism of the synergistic effects of the two mutations on prognosis can be explained at the molecular level. The BRAFV600E -activated MAP kinase pathway upregulates ETS transcription factors. The upregulation of ETS transcriptional factors leads to increased expression of TERT by binding to the binding site in the TERT promoter created by the C228T or C250T mutation. Overexpression of TERT increases tumor development and malignant transformation in thyroid cancer (16). However, the mechanism of this synergism has not yet been fully established. Moreover, owing to the low prevalence of TERT promoter mutations and limited studies containing data with TERT promoter and BRAFV600E mutations, the clinical effect of the TERT promoter mutation, BRAFV600E mutation, and their coexistence was initially uncertain. Detailed studies were required to prove their individual or synergistic effects on prognosis. In this context, the present study demonstrates a significant synergistic effect of the coexisting mutations on aggressive clinicopathologic outcomes of PTC.
There are several limitations in this study. First, the small number of studies and their small sample sizes led to insufficient statistical power, which affects the stability of the results. Second, because of the lack of data, it was not possible to conduct a subgroup meta-analysis based on other factors, such as subtype of PTC. Therefore, considering these limitations, larger well-designed studies are necessary to prove the synergistic role of TERT promoter and BRAFV600E mutations in the diagnosis and prognosis of PTC patients.
In conclusion, the coexistence of BRAFV600E and TERT promoter mutations has a synergistic effect on the clinicopathologic characteristics of PTC, including advanced TNM stage, extrathyroidal invasion, lymph node metastasis, and distant metastasis. Importantly, according to the available evidence, the coexistence of BRAFV600E and TERT promoter mutations are significantly associated with recurrence and PTC-related mortality as well. Therefore, molecular testing of BRAFV600E and TERT promoter mutations together may be useful in assisting with risk stratification of PTC in clinical settings.
Footnotes
Acknowledgments
This research was supported by Research Grant Number CB-2011-03-01 of the Korean Foundation for Cancer Research, and by the Seoul National University Hospital (grant 30-2015-0190).
Author Disclosure Statement
The authors declare no conflict of interest.