
Abstract
Background:
Cytologically defined indeterminate thyroid nodules are a diagnostic challenge. Surgical lobectomy remains the gold standard for definitive diagnosis. However, 70–85% of nodules are ultimately benign. The primary objective of this study was to evaluate the negative predictive value (NPV) of F18-fluorodeoxyglucose (FDG) positron emission computed tomography (PET/CT) in excluding cancer among cytologically indeterminate thyroid nodules within the authors' institution using surgical pathology as the gold-standard reference. In addition, a systematic review was performed of published prospective studies on the NPV of PET/CT in evaluating indeterminate thyroid nodules.
Methods:
A retrospective review was performed of all patients aged ≥18 years seen at the Mayo Clinic between January 1, 2000, and December 31, 2014, with cytologically defined indeterminate thyroid nodules (suspicious for Hürthle cell neoplasm or follicular neoplasm; N = 858), who had a PET/CT within one year of fine-needle aspiration (n = 80) and underwent definitive diagnostic lobectomy (n = 51). Nodules were considered PET negative if they had a standardized uptake value (SUV) <5. Additionally, a systematic review was performed of published prospective studies on the NPV of PET/CT across multiple sites.
Results:
Fifty-one patients met the eligibility criteria. The retrospective review combined with a systematic review of eight prospective studies suggests that indeterminate nodules with a negative PET (SUV <5) have a low risk of malignancy (NPV 94%). The cancer prevalence in the institution is 14% and 27% in the combined prospective studies.
Conclusions:
PET/CT represents a preoperative, non-invasive tool that when combined with sonographic features can identify indeterminate nodules at low risk for malignancy.
Introduction
W
Despite technologic advances in sonography, “early detection” of thyroid cancers among incidentally found thyroid nodules has not resulted in decreased thyroid cancer-related mortality (5). Moreover, increased rates of FNAs and high rates of “indeterminate” reports has led to more patients undergoing thyroidectomy for ultimately benign nodule(s) than for thyroid cancer (6).
Surgery, while definitive, is associated with an increased risk of complications, including vocal cord paralysis, hypothyroidism, hypoparathyroidism, bleeding/hematomas, and infection. Well-validated preoperative tests that can reliably discriminate benign from malignant indeterminate thyroid nodules across many sites are thus sorely needed.
Genetic approaches have emerged in recent years as tools for preoperatively differentiating benign from malignant indeterminate thyroid nodules, with three “rule-out” assays currently available (4). Despite the initial enthusiasm of molecular assays, the Afirma® gene expression classifier (GEC), for example, has performed poorly in the authors' center and inconsistently across other sites (7 –9). Moreover, validation studies for all three rule-out molecular assays have been performed using tumor tissues comprising cPTC and/or FV-PTC, with only a minority of cases representing FTC and/or HCC. The latter have few or no clearly identified genetic alterations, respectively. In the authors' center, only 15% of indeterminate nodules are malignant, and of these, FTC and/or HCC represent 60% of the malignancies, with only a minority (25%) being cPTC. Thus, molecular assays “trained” on tissues of up to 50% cPTC, such as the GEC, or trained on samples not enriched for FTC and/or HCC (i.e., all three rule-out assays) are likely to have poor clinical utility in centers such as the Mayo Clinic, in which indeterminate FNA results (Bethesda category 4) are limited to “true” follicular neoplasms (i.e., FA or FTC) (10).
Alternatively, positron emission computed tomography (PET/CT) is a sensitive and non-invasive imaging tool for identifying malignant lesions. PET/CT is widely used for staging solid tumors, guiding therapy, and detecting recurrences. Malignant transformed cells typically have increased expression of glucose transporters and higher glycolytic rates than those of surrounding normal tissue. This altered metabolism leads to an increased accumulation of the radiolabeled glucose analog F18-fluorodeoxyglucose (F18-FDG) in malignant compared with benign lesions. The efficacy of F18-FDG PET/CT in discriminating benign from malignant lesions has been well established, particularly in the evaluation of incidentally identified pulmonary nodules. Approved by Medicare for reimbursement since 1998, FDG PET/CT is routinely used in the evaluation of lung nodules >8 mm (11). Multiple studies, including within the authors' center, have shown that incidentally discovered FDG-avid thyroid nodules have a high (35%) incidence of thyroid cancer in a series from the authors' institution (12,13). Conversely, few studies have examined the negative predictive value (NPV) of a negative PET/CT in excluding thyroid cancers among cytologically defined indeterminate thyroid nodules (14 –21). A single meta-analysis of six studies, with 225 patients and using surgical pathology as the gold standard, reported that an indeterminate nodule with a negative PET, defined as a thyroid nodule without increased focal uptake above background, had an overall NPV of 96% in excluding thyroid cancer (22). Thus, PET/CT may be an alternative and less invasive tool for preoperatively discriminating benign from malignant indeterminate thyroid nodules.
The main purpose of this study was to evaluate retrospectively the NPV of FDG PET/CT in excluding cancer among cytologically defined indeterminate thyroid nodules within the authors' institution using surgical pathology as the gold-standard reference. Finally, to confirm PET/CT as a potential tool in real-time clinical practice, a systematic review was performed of published studies examining the role of PET/CT imaging prospectively in the evaluation of cytologically defined indeterminate thyroid nodules among multiple centers.
Material and Methods
A retrospective, IRB-approved chart review was performed of all adult patients (≥18 years) seen at the Mayo Clinic between January 1, 2000 and December 31, 2014 (N = 858) with cytologically defined indeterminate thyroid nodules after US-FNA (suspicious for HCN or FN) who also had an FDG PET/CT within one year of thyroid FNA (n = 80; usually FDG PET/CT was performed for other reasons) and who underwent definitive diagnostic lobectomy. Fifty-one patients met the eligibility criteria. Incidental, papillary thyroid microcarcinomas (PTM) identified postoperatively (n = 3) were excluded from the data analyses. The maximum standardized uptake value (SUVmax) that best separated benign from malignant lesions was determined by a receiver operating characteristic (ROC).
FNAs were performed under US guidance by experienced endocrinologists or radiologists using 25–27-gauge needles (four to six passes per nodule). All cytology slides were reviewed by an experienced thyroid cytopathologist.
An experienced nuclear medicine radiologist (J.D.) independently, and in a blinded manner to either sonographic and/or surgical pathology results, reviewed and quantified all FDG PET/CT scans. All FDG PET/CT scans were performed on GE Discovery PET/CT scanners. SUV is defined as a region of interest (ROI) activity (mCi/mL) divided by the administered activity per body weight (mCi/g = mCi/mL). SUVmax was measured in a ROI placed over each cytologically indeterminate nodule. The total body weight of the patient was used for the SUV calculation, rather than the lean body mass. The administered activity of F18 FDG was 15 mCi ± 10%. All studies were performed 60–70 min after the administration of the radiopharmaceutical. Images were acquired in 3D mode at 2, 3, or 4 min per bed position (depending on the patient's weight). All patients had fasted for at least 4 h, except for water. Glucose level measured prior to each study was <200 mg/dL.
Next, US images were reviewed using a risk-stratification scheme consistent with the American Thyroid Association (ATA) 2015 guidelines (4), and the sonographic patterns of all but one of the indeterminate nodules (one patient without available US imaging) were determined. Indeterminate nodules were then classified according to level of suspicion (i.e., benign, very low, low, intermediate, high).
A systematic review was performed of published articles in English between 2000 and 2015 using OVID MEDLINE, OVID MEDLINE In-Process, Embase, and PubMed databases. Keywords searched included: positron emission tomography, FDG PET, positron, indeterminate thyroid nodules, thyroid nodule, indeterminate, or words containing undetermined, atypia, suspicious, uncertain, preoperative, and presurgical. Articles selected were limited to those with reported FNA indeterminate cytology, FDG PET/CT preoperatively, and final surgical pathology available with cancer rates consistent with national estimates (∼15–30%). A total of 33 articles were identified of which eight met the inclusion criteria (see Fig. 1). Representative countries included the United States and one each from Brazil, Netherlands, France, Austria, and Spain.
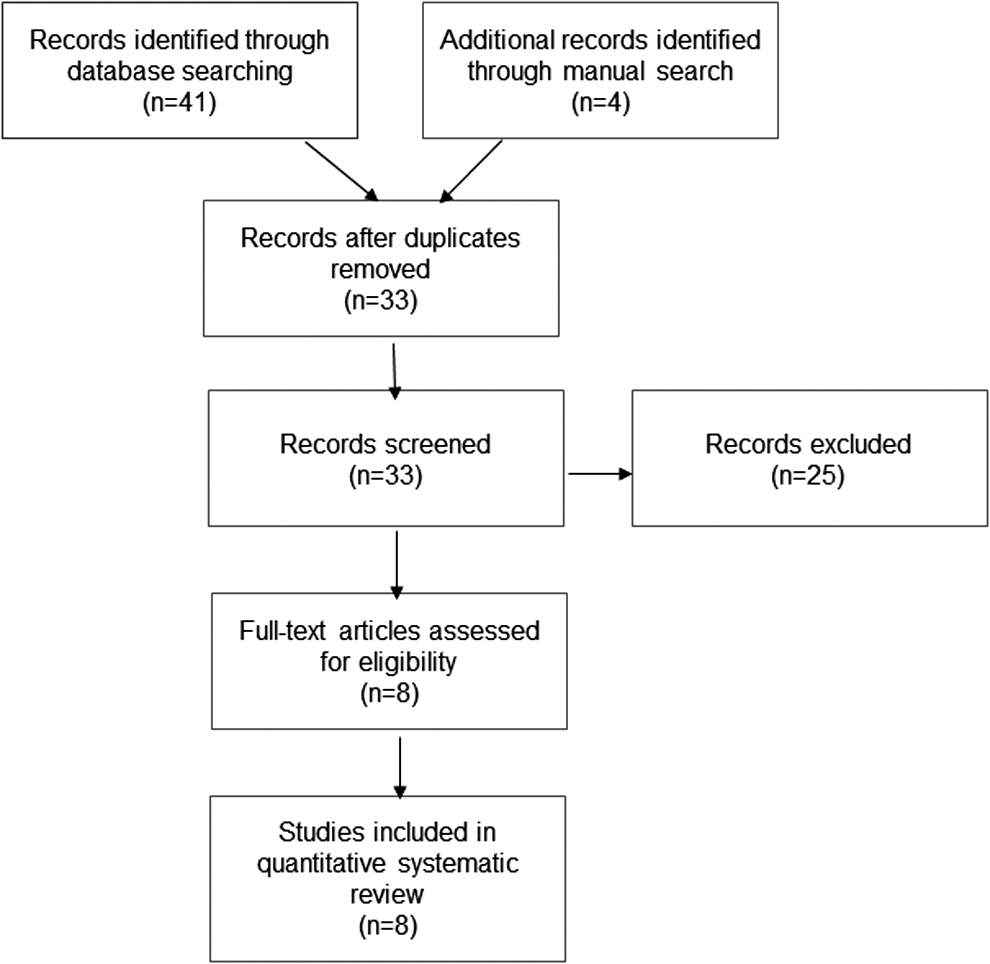
Results of literature search.
Results
FDG PET/CT
Fifty-one patients were identified with indeterminate thyroid nodules (n = 27 S-FN, n = 24 S-HCN) for whom a preoperative PET/CT and definitive surgical pathology were available. The SUVmax value that best separated benign from malignant lesions was determined by ROC analysis, and was found to be an SUV of 5. In this study, PET negative was defined as an SUV <5.
Twenty (39%) patients had SUV values <5, ranging from 2.1 to 4.9. The remaining nodules (n = 31; 61%) had SUV ≥5.0, ranging from 5.0 to 86.1. The median nodule size for both groups was 1.8 cm, with a range of 0.8–7.4 cm. Patient demographics were similar in both groups (Table 1). In patients with thyrotropin levels (TSH) performed (n = 43), there was no significant difference between patients with malignant (n = 7) versus benign (n = 36) nodules (M = 1.79 vs. 2.26; p = 0.37).
One patient did not have an US imaging/report.
SUV, standard uptake value; PET, positron emission tomography; US, ultrasound.
Of the 27 nodules identified as S-FN, 12 (44%) were classified as PET negative and 15 (56%) as PET positive (Tables 2 and 3). At final surgical pathology, one PET-negative and three PET-positive nodules were malignant (15% cancer incidence), providing a positive predictive value (PPV) and NPV of 20% and 92%, respectively. The single PET-negative, cancer-positive nodule represented a PTM for which SUV values may be underestimated due to partial volume effect. Excluding the sub-centimeter nodule, the NPV increases to 100%. Interestingly, two nodules with the highest SUVs (86.1 and 48.4) represented follicular adenomas.
CT, computed tomography; FNA, fine-needle aspiration; PPV, positive predictive value; NPV, negative predictive value; S-FN, suspicious for follicular neoplasm; S-HCN, suspicious for Hürthle cell neoplasm; PTC, papillary thyroid cancer; HCC, Hürthle cell carcinoma; FTC, follicular thyroid carcinoma.
Of the 24 nodules defined as S-HCN, 8 (33%) were classified as PET negative and 16 (67%) as PET positive. At final surgical pathology, one PET-negative and two PET-positive nodules were malignant (13% cancer incidence), with a PPV and NPV of 13% and 88%, respectively. The single PET-negative, cancer-positive nodule represented a 2.3 cm minimally invasive FTC. Altogether, excluding the sub-centimeter nodules, the overall NPV of PET-negative indeterminate thyroid nodules was 95%. As summarized in Table 5, this NPV is consistent with published prospective PET/CT studies of indeterminate thyroid nodules (14,17,18,20,21). In the authors' experience, the PPV of PET/CT in identifying thyroid carcinomas among indeterminate nodules was lower than that for PET-positive thyroid nodules in general.
US characteristics
Using a risk-stratification scheme consistent with the ATA 2015 guidelines (4), sonographic patterns of indeterminate thyroid nodules were reviewed for all but one patient (no US available), and they were further classified according to risk (Table 4). Sonographically, none were classified as a benign pattern, and three (6%) had a very low suspicion pattern; none of these was malignant. Fourteen (28%) nodules were classified as low suspicion, with one (7%) positive for malignancy, which was a minimally invasive FTC (2.3 cm). The majority (32; 64%) of nodules were classified as intermediate and high suspicion. Of 16 intermediate patterns, two were malignant, representing a HCC with capsular and vascular invasion (5.2 cm) and a PTC (1.1 cm). Of 16 high-suspicion pattern nodules, four were malignant (25%), representing two PTM (0.7 cm and 0.8 cm), one widely invasive HCC (2.8 cm), and one locally invasive FV-PTC (4.4 cm). One indeterminate nodule did not meet the criteria for a defined ATA sonographic pattern. SUVs varied greatly; nodules classified sonographically as very low risk had a range of SUVs from 2.4 to 48.4, while nodules in low-, intermediate-, and high-risk categories had maximal SUVs of 21.4, 33.2, and 86.1, respectively. Notably, the SUVmax of a malignant lesion in this study was 21.8.
One case not included, as no US image available (benign).
PET/CT negative (minimally invasive FTC).
Both PET/CT positive.
Three PET/CT positive, one PET/CT negative (microPTC).
ATA, American Thyroid Association.
Systematic review
The systematic review of published studies, using preoperative PET/CT to classify indeterminate thyroid nodules, identified eight prospective studies that included 309 patients with final histopathology as the gold-standard reference (Table 5). The Bethesda classification system was used in two of the eight studies (15,19). One study classified nodules by the World Health Organization classification for thyroid tumors (20), and the remaining five either did not mention the method and/or were completed prior to implementation of the Bethesda classification system in 2009.
Of those that did have variability in the SUVs used to define PET negativity and positivity, 143 (46%) were ultimately classified as PET negative (no focal FDG uptake) with nine (6%) malignant on final pathology (five PTC, one PTM, one PTC-FV, and two tumors of unknown malignant potential [TUMP]) and an overall NPV of 94%. Four studies that included 169 patients had NPVs of 100% (14,17,20,21). Only one study reported a NPV of 57% (16). This was a pilot study limited to only 15 patients, and included an incidental 0.1 cm PTM. In a study from France by Deandreis et al. (2012), the NPV of 84% reflects nine PET-negative, indeterminate thyroid nodules that on final pathology were classified as TUMP. This histological category is not represented in the Bethesda classification scheme used in the United States. Five studies confirmed the current findings with NPVs ≥95%, which included 111 PET/CT-negative nodules, and all but one were benign on final histopathology (14,17,18,20,21). The cancer prevalence in these studies ranged from 4% to 47%.
Discussion
With the widespread use of US and US-FNA, along with the implementation of the Bethesda classification scheme for thyroid nodules, which attempted to provide a uniform approach to the classification of thyroid nodules by cytology, an increasing number of “indeterminate” nodules are being diagnosed, especially related to category III, AUS/FLUS (6). This has resulted in widely variable cancer prevalence rates between centers for indeterminate nodules making it difficult for any one test, such as molecular markers, to function equivalently in all practices. An alternative diagnostic test that relies on specific functional and/or physical properties of malignant nodules (i.e., increased glucose uptake) may represent an alternative strategy for discriminating benign from malignant nodules.
In the authors' high-volume thyroid nodule practice with around 1000 FNAs performed annually, the majority of cytopathology results are reported as benign, suspicious for malignancy, or malignant. Only 10% of FNAs are classified as S-FN/S-HCN in the authors' institution and very rarely are reported as “atypical” (10). Thus, at the authors' institution with experienced thyroid cytopathologists, most thyroid nodules are definitively classified into one of the actionable categories, with only 10% of nodules requiring additional preoperative tests and/or diagnostic lobectomies for indeterminate results. Following diagnostic lobectomy for FNAs of S-FN/S-HCN, of the 15% proven malignant, 59% represented FTC or HCC, 14% FV-PTC, and only 25% cPTC (10). This histologic pattern most likely explains why the GEC performed so poorly in the authors' center, since the latter was “trained” on around 50% cPTC and included only 23% FTC/HCC (23). Likewise, Thyroseq2 and ThyGenX plus ThyraMIR, the other two rule-out assays, may or may not perform well in this or other centers, as the NPV of these tests was validated on tumors representing ≤20% FTC/HCC (24,25).
The present data demonstrate that S-FN nodules (>1 cm) with an SUV <5 have a very low risk for malignancy (0% in this study). Similarly, S-HCN nodules with an SUV <5 also have a low risk for malignancy (12.5%). Overall, combining the data for S-FN and S-HCN, using an SUV <5 to define PET negativity for nodules >1 cm, the NPV of PET/CT was 95% in this study, meeting current clinical criteria for which surveillance could be considered. In 5% of cases, in which a PET failed to exclude a cancer, the lesion represented a benign-behaving minimally invasive FTC. Consistent with this study, a systematic review of eight prospective PET/CT studies of indeterminate thyroid nodules showed a high overall NPV of 94% in excluding underlying cancer. The false-negative PET results in these studies represented low-grade PTCs (i.e., FV-PTC, PTCs) that often behave in an indolent manner. The National Comprehensive Cancer Network (NCCN) indicates observation of indeterminate nodules is reasonable, as opposed to surgery, if the test has a NPV of ≥95% (26).
The PPV in this study was low (13%), suggesting focal, intense FDG uptake in a cytologically defined indeterminate thyroid nodule is non-specific and a poor biomarker for malignancy, unlike PET positivity of unselected thyroid nodules. This may reflect differences in malignancy patterns of indeterminate versus overall thyroid nodules, the latter of which most commonly reflect cPTC. The majority of S-HCN (67%) in this study, with a referral bias, were FDG avid, and may reflect a high level of metabolic activity. A prospective study of HCN and PET/CT is needed to understand the cost efficacy of PET/CT for such nodules. Given their potential propensity for FDG avidity, PET/CT may, however, be useful in the staging of high-risk, widely angioinvasive HCC, which most commonly lack radioiodine uptake but whose metastatic foci may retain FDG avidity. Several published series of HCC patients showed improved disease detection compared with anatomic or radioiodine imaging (27,28).
The present data suggest that indeterminate thyroid nodules classified as high suspicion by US (n = 16) have a 25% risk of malignancy (n = 4), of which one was PET negative, measuring 0.7 cm. The risk of malignancy based on the proposed US pattern for high-suspicion nodules by the ATA guidelines is lower than predicted (4). The data suggest that follicular lesions have distinct sonographic patterns compared with most PTCs, and thus sonography alone is less able to discriminate benign from malignant nodules. Intermediate pattern nodules (n = 16) had a 12.5% risk of cancer, similar to the ATA guideline categories, and none (0%) of the proven malignancies was PET negative. Nodules with either benign, very low, or low suspicion by sonography have a very low risk of malignancy, and the majority were non-FDG avid. Combining PET/CT with US for sonographically defined intermediate or high-suspicion nodules may enable surveillance for those with a negative PET (SUV <5).
A major limitation of this study is its retrospective nature, which resulted in a referral bias and enrichment of PET-positive indeterminate thyroid nodules. This may have led to an underestimation in the number of PET-negative indeterminate nodules, which in turn may underestimate the proportion of patients who may be able to avoid diagnostic lobectomy in the authors' practice. Indeed, data from the independent prospective studies of 309 patients from eight different centers support these findings, indicating a low rate of cancer among PET-negative indeterminate thyroid nodules (NPV 94%) (14 –21). Moreover, the overall rate of PET/CT-negative nodules was 46% in these studies, suggesting that a significant proportion of patients may indeed be able to avoid diagnostic lobectomy based on PET/CT results. Another limitation of this study is that almost all patients had an FDG PET/CT done for evaluation of various malignancies, creating a selection bias of patients with indeterminate nodules. The presence of FDG-avid lesions elsewhere in the body may have resulted in reduced FDG uptake and SUV values for thyroid nodules (29) (less tracer would be available for uptake in the nodule if there was a large volume of intensely avid malignancy). The present study includes images from early PET/CT scanners (2000) to more advanced current-generation scanners (improved resolution, time of flight imaging). However, the data remain consistent with published, prospective PET/CT studies, as noted above.
In summary, the present findings, in combination with the systematic review of eight prospective studies, suggest that indeterminate nodules with a SUV <5 have a very low risk of malignancy (NPV 94%). PET/CT represents a non-invasive and widely available tool for risk stratifying indeterminate nodules and a tool that can easily be validated within individual centers. PET/CT, though itself not inexpensive, has a proven overall cost efficacy (30) by potentially reducing the number of diagnostic lobectomies by around 45%. Moreover, PET/CT is not limited by sample preparation and storage techniques as for molecular assays. Finally, to the best of the authors' knowledge, this is the first study to show, for cytologically indeterminate thyroid nodules, that the ATA 2015 guidelines sonographic patterns (4), in combination with PET/CT, can identify nodules at low risk for malignancy for which surveillance may be considered.
In a time of overdiagnosis without a reduction in thyroid cancer mortality rates (5), as well as a paradigm shift toward observation of confirmed PTM (31,32), these data suggest indeterminate thyroid nodules that are PET negative have low risk for clinically significant thyroid cancers and for which surveillance may be most appropriate.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.