
Abstract
Objective:
Considering the limited data available on the natural course of euthyroidism, this study was designed to evaluate the progression in time from euthyroidism to subclinical or overt hypo- or hyperthyroidism.
Methods:
This study was conducted within the framework of the Tehran Thyroid Cohort Study, in which 5783 individuals aged 40.4 ± 0.2 years were followed for six years. The overall loss to follow-up rate was 8.3%. After applying exclusion criteria, data of 4204 euthyroid subjects remained for analysis of a six-year natural course analysis. Thyroid function tests, clinical characteristics, and metabolic characteristics were assessed at baseline and every three years.
Results:
The annual incidence rates [confidence intervals (CI)] of subclinical and overt hypothyroidism were 7.62 [CI 7.39–7.85) and 2.0 [CI 1.94–2.06] per 1000 persons, respectively. For thyroid hyperfunction, the annual incidence rates of subclinical and overt hyperthyroidism were 0.92 [0.90–0.95) and 0.68 [0.66–0.70) per 1000 persons, respectively. Euthyroid persistency was 93.24% during 6 years. Predictive factors for conversion to thyroid dysfunction were thyrotropin, free thyroxine and thyroid peroxidase antibody levels, sex, and smoking. Criteria for early diagnosis of hypothyroidism (i.e., sensitivity of 94% and specificity of 82%, p < 0.0001) were obtained based on baseline and three-year follow-ups of thyroid function tests and thyroid peroxidase antibody. Early diagnosis of hypothyroidism was significantly associated with impaired glucose tolerance (relative risk with 3.03 [CI 1.36–6.75]; p = 0.007), high cholesterol (relative risk 2.46 [CI 1.45–4.18]; p = 0.001), obesity (relative risk 2.92 [CI 1.64–5.2]; p < 0.001), and hypertension (relative risk 1.68 [CI 1.53–1.84]; p < 0.04).
Conclusion:
This study shows that after a six-year follow-up in an iodine sufficient area, 6.7% of euthyroid subjects were found to progress to thyroid dysfunction, in particular subclinical hypothyroidism.
Introduction
T
Although studies evaluating the time course of subclinical hypo- and hyperthyroidism to overt diseases are abundant (4,5), data regarding the natural course of euthyroidism in general populations are scarce. In addition, factors that play a main role in the natural history in the transition of euthyroidism to thyroid dysfunction need to be determined. The magnitude of the complications caused by abnormal thyroid function is not entirely known. The rate of progression from the euthyroid state to thyroid disease is also a key factor in potential cost implications for health care systems, including screening programs (1,2,6 –9). Additionally, early detection and treatment of subclinical thyroid dysfunction is potentially beneficial, since some studies report the occurrence of various adverse health outcomes such as osteoporosis, hyperlipidemia, hypercholesterolemia, hyperhomocysteinemia, and cardiovascular and neuropsychiatric disorders in cases with thyroid diseases, especially among the elderly (2,6 –9).
In this large cohort study, we aimed to determine the natural course of thyroid functions over a six-year period, including rates of progression to subclinical hypo- or hyperthyroidism and overt hypo- or hyperthyroidism or the persistence of euthyroidism.
Subjects and Methods
Study design
The present study was conducted within the framework of the TTS (10), a population-based cohort study performed on residents of district 13 of Tehran with the aim of evaluating the prevalence and natural course of thyroid diseases and their long-term consequences in terms of ischemic heart disease and cardiovascular and all-cause mortality in the urban, iodine-sufficient population of Tehran, the capital of Iran. Details of the study methods have been previously described (10). The TTS is being conducted within the framework of the Tehran Lipid and Glucose Study (11), in which 15,005 residents, aged ≥3 years participated. Data collection is ongoing, designed to continue for at least 20 years, with 3-year intervals. Of 10,368 subjects aged ≥20 years, 5786 subjects who had serum samples for measuring thyroid function tests at baseline and follow-up phases were selected to participate in the TTS.
The ethics committee of the Research Institute for Endocrine Sciences (RIES) of Shahid Beheshti University of Medical Sciences approved the protocol for this study. Written informed consent was obtained from all subjects.
Settings
In brief, 5783 persons (2377 men and 3406 women) aged ≥20 years were evaluated in the TTS, at baseline and again after three and six years respectively (10,12). The cohort profile is given in Figure 1. In each phase, detailed interviews were conducted by trained interviewers. Demographic data and information regarding smoking habits, history of radioiodine ablation and thyroid surgery, and detailed information on medication use (e.g., antithyroid, thyroxine, or any medication interfering with thyroid function) were recorded.
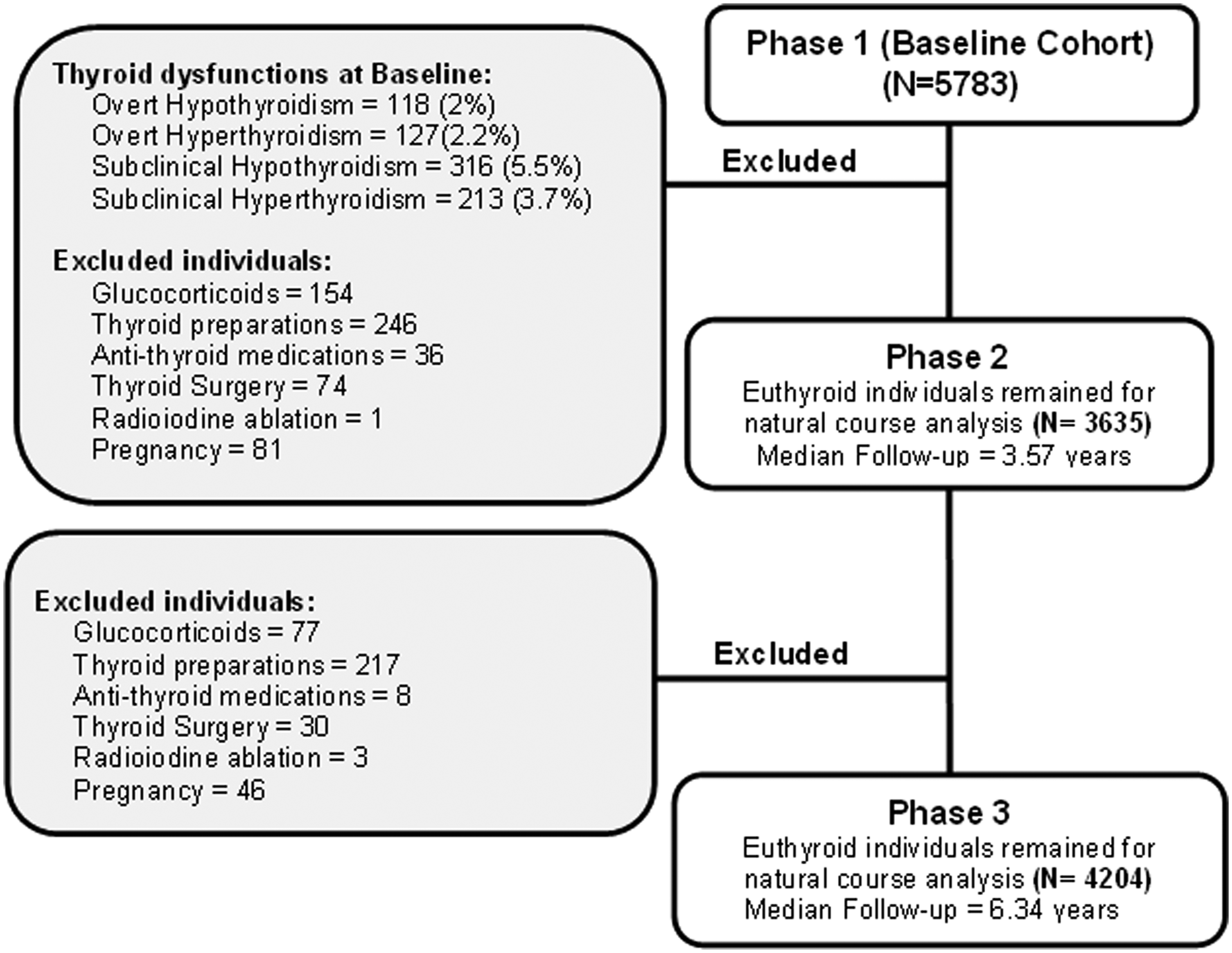
Cohort profile of the Tehran Thyroid Study. Reasons for excluded cases are given, and the total number of euthyroid individuals for natural course analysis is displayed for each phase. Overall loss to follow-up rate was 8.3% over six years of follow-up.
Participants
The eligibility criteria for studying the natural course of euthyroidism were defined as no history of thyroid surgery or radioiodine ablation, no history of past or current use of thyroid preparations or antithyroid medications, not being under treatment with glucocorticoids, and not being pregnant at the time of recruitment. Patients lacking any eligibility criteria were excluded from analysis at each phase. Finally, 5086 (86.6%) individuals remained for the study of whom data of 3635 and 4204 subjects remained for natural course analysis after 3 and 6 years, respectively; data for 569 individuals were available only after 6 years. Information about follow-up visits has previously been described (10).
Variables
For analysis of outcomes, individuals at baseline and years 3 and 6 were categorized into four categories according to the normal reference ranges of thyroid function tests in Iranian populations (13): (1) subclinical hypothyroidism was defined as serum thyrotropin (TSH) level >5.06 mU/L with normal free thyroxine (FT4) level; (2) overt hypothyroidism was defined as serum TSH level >5.06 mU/L and FT4 < 0.91 ng/dL; (3) subclinical hyperthyroidism was defined as serum TSH level <0.34 mU/L and normal FT4 level; and (4) overt hyperthyroidism was defined as a TSH concentration <0.34 mU/L with serum FT4 concentration >1.55 ng/dL (13).
Baseline values of demographics, anthropometrics, and metabolic profiles including fasting blood glucose, two-hours postprandial glucose, lipid profile, thyroid function tests, smoking habits, and blood pressure were investigated as predicting and/or confounding variables.
Data sources and measurements
Fasting blood samples were drawn from all participants between 7:00 and 9:00
Statistical analysis
Quantitative data are described as mean ± standard deviation for normally distributed data, based on the Kolmogorov-Smirnov test, while nonnormal variables are presented as median (interquartile range, P25–P75). Categorical data, explained by percentages, were tested by chi-squared, Fisher's exact, or Monte Carlo tests. Incidence rates of clinical hyperthyroidism, clinical hypothyroidism, and subclinical hypo- and hyperthyroidism were estimated per 1000 person-years. Also, relative risk (RR) with 95% confidence intervals have been used to describe the incidence of progression to thyroid dysfunction as compared with euthyroid persistency after three and six years of follow-up. Repeated measures multivariate analysis of variance (ANOVA) was conducted to investigate the changes of the quantitative data collected over six years of follow-up. Within-group variance of nonparametric data was assessed by Wilcoxon and Friedman tests. Between-group differences were analyzed by one-way ANOVA, Student's t-test, Kruskal-Wallis, and Mann-Whitney U tests, where indicated. RRs of outcomes linked with TSH and FT4 levels were adjusted for regression dilution bias by Rosner regression dilution ratios of the TTS (12). Receiver operating characteristic (ROC) curve analysis was also used to find the most sensitive/specific TSH/TPOAb cutoff levels for defining the natural course of thyroid function, by assuming nonparametric distributions for which the Youden index method was used, along with the corresponding sensitivity and specificity. Diagnostic odds ratios with 95% confidence intervals were calculated (positive likelihood ratio divided by negative likelihood ratio) to explain the effectiveness of diagnostic criteria, because diagnostic odds ratios are not sensitive to the low prevalence of outcomes (14). We also employed multinomial logistic regression to determine the effects of various demographic, clinical, and biochemical factors on progression to thyroid dysfunction or euthyroid persistency. Binary logistic regression was also used to determine the associations between early diagnosis of euthyroidism (based on the proposed criteria) and some metabolic outcomes. To adjust for multiple testing, the Benjamini-Hochberg method (15) was used to control the false discovery rate. All statistical analysis was carried out using the Stata statistical package program version 13 (Stata Corp.).
Results
The prevalence of thyroid dysfunction at baseline (with no exclusion criteria) was found to be 118 (2%) and 127 (2.2%) for overt hypothyroidism and hyperthyroidism, respectively and for subclinical hypothyroidism and hyperthyroidism it was 316 (5.5%) and 213 (3.7%), respectively. A total of 5086 (86.6%) individuals aged 40.4 ± 0.2 years were euthyroid at baseline. Data of excluded individuals are shown in Figure 1. After 3 years, 3400 (93.5%) individuals remained euthyroid, of whom 3920 (93.2%) showed normal thyroid status after 6 years. For thyroid hypofunction, the annual incidence rates [with CIs] of subclinical and overt hypothyroidism were 7.62 [CI 7.39–7.85] and 2.0 [CI 1.94–2.06] per 1000 persons, respectively. A total of 81 subjects who were euthyroid at baseline became subclinically hypothyroid at after 3 years and all of them returned again to an euthyroid status again after 6 years. Regarding hyperfunctioning of the thyroid, the annual incidence rates of subclinical and overt hyperthyroidism were 0.92 [CI 0.90–0.95] and 0.68 [CI 0.66–0.70] per 1000 persons, respectively. Table 1 displays the annual incidence rates and risk for progression to thyroid dysfunction.
Euthyroid persistent group considered as reference.
Per 1000 person-years.
The incidence rates of six-year follow-up show the final outcome of individuals, so they are cumulative of incidences at three-year follow-up in cases of persistent conditions, though for cases of normalization from thyroid dysfunctions to euthyroidism, the rates are diluted.
χ2, chi-squared; CI, 95% confidence interval; RR, relative risk.
Baseline demographic, anthropometric, and laboratory characteristics for the six-year natural courses of euthyroid subjects are shown in Table 2, indicating that progression to subclinical (n = 136) and overt hypothyroidism (n = 41) was more frequently observed in females (p < 0.001). While TSH, FT4, and TPOAb levels were within the normal reference range at baseline, they differed significantly between groups of natural course (e.g., hypothyroid vs. persistently euthyroid individuals) (p < 0.001).
Quantitative data with normal distribution are shown as mean ± standard deviation, while nonnormal data are presented as median (interquartile range: P25–P75). Categorical data are reported as counts (percentages).
Smoking data had 1.3% random missing.
BMI, body mass index; FT4, free thyroxine; TPOAb, thyroperoxidase antibodies; TSH, thyrotropin.
Data regarding the most important predictors of natural course of euthyroid subjects are illustrated in Table 3. Based on the regression dilution ratios–adjusted RR of multivariate multinomial logistic regression, each mU/L increase in TSH was associated with a 9.32-fold greater risk of progression to subclinical hypothyroidism and a 5.40-fold increased risk of overt hypothyroidism, whereas other variables were controlled. Smoking was only a significant risk factor for overt hyperthyroidism.
Relative risks of outcomes linked with TSH and FT4 levels were adjusted regarding regression dilution bias by Rosner regression dilution ratios (RDR) of Tehran Thyroid Study [10] (exp(LN (RR) /RDR)).
Based on ROC analysis (Supplementary Fig. S1; Supplementary Data are available online at
Cutoff points for thyroid functions tests are extracted based in receiver operating characteristic analysis.
Adjusted (adj) RR, relative risks of outcomes linked with TSH and FT4 levels were adjusted regarding regression dilution bias by RDR of the Tehran Thyroid Study [10] (exp(LN (RR) /RDR)).
Simultaneous sensitivity = Sensitivity 1 + Sensitivity 2 − (Sensitivity 1 × Sensitivity 2); Simultaneous specificity = Specificity 1 × Specificity 2. Sensitivity 1 is related to baseline and sensitivity 2 is related to data at 3-years follow-up.
Sequential sensitivity = Sensitivity 1 × Sensitivity 2; Sequential specificity = Specificity 1 + Specificity 2 − (Specificity 1 × Specificity 2).
It is clear that the diagnostic criteria for subclinical hypothyroidism is applicable when free thyroxin levels are within normal range.
DOR, diagnostic odds ratio (positive likelihood ratio/negative likelihood ratio).
Early diagnosis of subclinical hypothyroidism was also significantly associated with impaired fasting glucose (fasting blood sugar = 100–125 mg/dL; RR 1.49 [CI 1.13–1.96]; p = 0.005), high cholesterol (TC ≥240 mg/dL; RR 1.60 [CI 1.15–2.23]; p = 0.005), and obesity (body mass index >30 kg/m2; RR 1.54 [CI 1.14–2.07]; p = 0.002).
Figure 2 illustrates the longitudinal variations of TSH, FT4, and TPOAb levels (over three TTS phases) among various outcomes of euthyroid individuals. For crude values, the significant time (p < 0.001) and time × groups (p < 0.0001) interaction indicates the different natural courses of thyroid functions and TPOAb among euthyroid individuals and thyroid disorders. After adjustment for sex, smoking status, and baseline waist to hip ratio (WHR) (baseline difference of groups), TSH, and FT4 showed significant time (p < 0.05) and time × groups (p < 0.0001) interaction. However, adjusted TPOAb levels did not differ significantly across the three phases of the TTS. Adjusted TPOAb levels showed a significant group (p < 0.001) and time × groups (p < 0.0001) interaction.
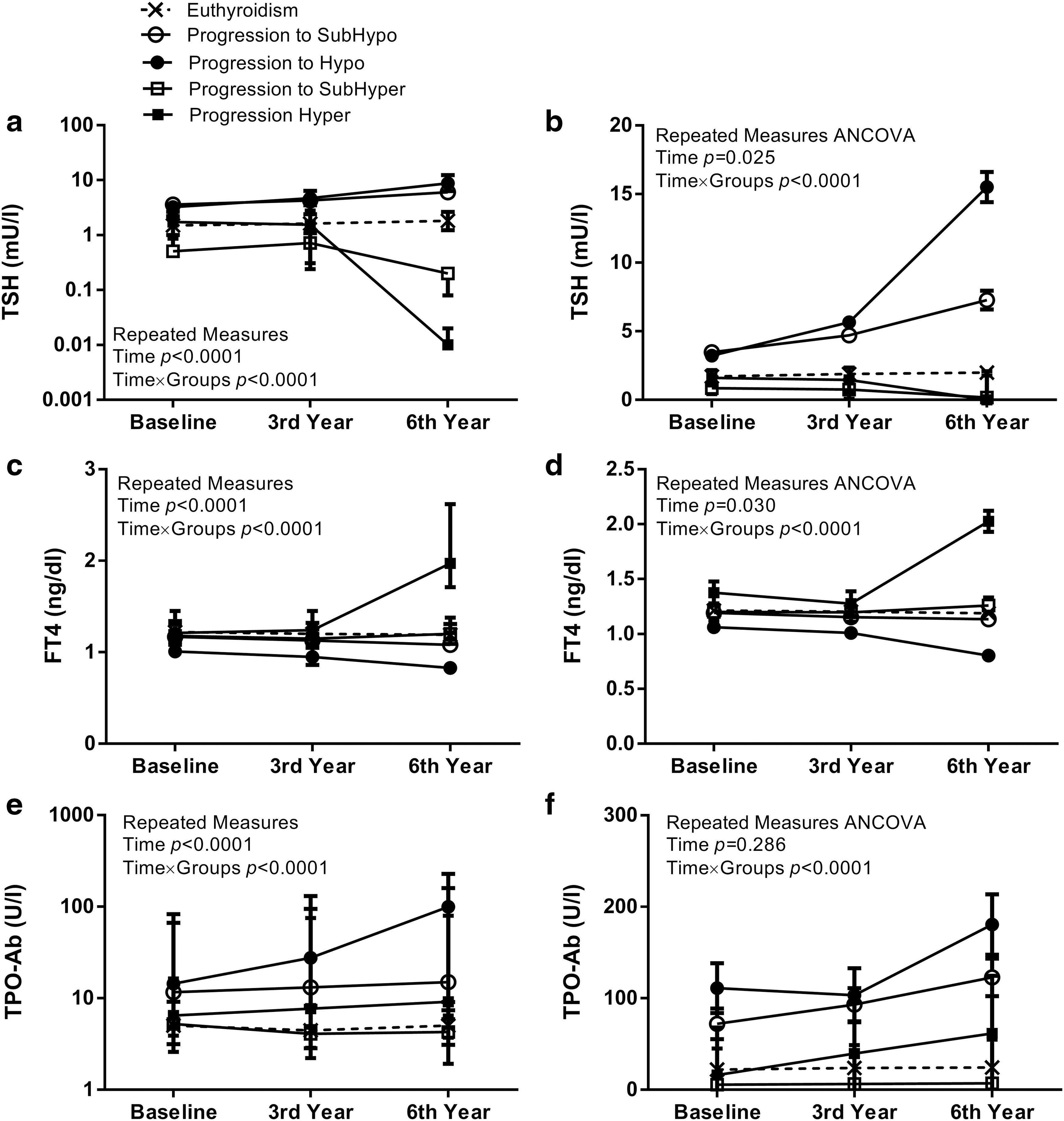
Longitudinal changes of thyrotropin (TSH) (
Discussion
The main findings of our study are as follows: (1) euthyroid persistency was as high as 93% during 6 years of follow-up; (2) conversion rates to subclinical hypothyroidism after 3 and 6 years were 4.3% and 4.6% respectively; (3) progression rates to overt hypothyroidism after 3 and 6 years were 0.6% and 1.2% respectively; (4) progression rates to subclinical and overt hyperthyroidism were approximately 0.6% and 0.4% respectively; and (5) criteria for early diagnosis of thyroid hypofunction were provided, which might be helpful in predicting the progression to subclinical and overt hypothyroidism.
The historical cohort of the Whickham Survey documented an incidence of thyroid disorders in a randomly selected sample of 2779 British adults to be 3.5/1000/year [CI 2.8–4.5] for spontaneous hypothyroidism of females and 0.6/1000/year [CI 0.3–1.2] for men (16). Moreover, the incidence of hyperthyroidism in women was reported to be 0.8 per 1000 person-years [CI 0.5–1.4] and was negligible in men (16). Both raised serum TSH and positive antithyroid antibodies were the paramount predictors of progression to hypothyroidism in the Whickham Survey and the study done by Guel et al. (16,17), results in line with our findings.
In addition, in the Colorado Thyroid Diseases Prevalence study, 88.3% of the total population was euthyroid, with men being more frequently euthyroid than women, revealing a prevalence similar to that of our study (86.6%), and consistent with findings in iodine-replete populations (1). The natural history of euthyroidism most probably depends on the presence of underlying autoimmunity, TSH levels (even in normal range), age, and sex; however, long-term prospective data on euthyroid individuals are rare, making it difficult to determine their definitive course (1,2,16). The results of the Amsterdam autoimmune thyroid disorders (AITD) cohort study showed that overt hypothyroidism and hyperthyroidism developed in 4.8% and 1.7% of female individuals, respectively during a 5-year follow-up of those prone to the disorders; however, the occurrence of hypothyroidism was reported only in females with family history of autoimmune thyroid diseases in this study (18). Another nested case-control study conducted within the framework of the Amsterdam AITD cohort study revealed that higher TSH and lower FT4 are predicting factors for conversion from euthyroidism to autoimmune hypothyroidism (19), results in agreement with those of the TTS.
The incidence of subclinical hypothyroidism in 3057 U.S. euthyroid individuals (≥65 years of age) has been reported to be 2.7% (84 of 3057) over a 2-year period (20). The prevalence of subclinical hypothyroidism has been reported to be 3–12% (16,21), and 1–6% for subclinical hyperthyroidism (1,2,22), findings in line with those of our study.
Studying the natural course of euthyroid individuals progressing to thyroid over-activity in large populations is crucial; to our knowledge there is no prospective data documenting this in large cohorts; the majority of studies evaluating the spontaneous changes in subclinical hyperthyroid patients report that progression to overt hyperthyroidism is rare (5,22,23). The retrospective cohort of the Thyroid Epidemiology, Audit, and Research Study showed an annual incidence of 30–40 per 100,000 population (with a median follow-up of 4.3 years) (23), an incidence different from that of our study (92 per 100,000 population during median follow-up of 6.34 years), and that of the Whickham Survey (101.9 per 100,000) (16).
Overall, determining euthyroidism or progression to thyroid dysfunction mostly depends on our definitions for TSH normal values. In the present study, the cutoff value for abnormal TSH was >5.06 mU/mL, which is the upper normal limit of TSH values in the TTS (13). Huber et al. considered a TSH level of <6 mU/L as a predictor of lower likelihood of progression to thyroid hypofunction (24). Walsh et al. showed that the risk of hypothyroidism is very low in males with a baseline TSH ≤2.5 mU/L and increases progressively across higher categories of TSH. The use of TSH limits of 2.5 and 4.0 mU/L, in the presence of thyroid antibodies provides a clinically useful estimate of the long-term risk of hypothyroidism and Walsh et al. concluded that female sex and baseline TSH were the strongest risk factors for the occurrence of hypothyroidism at follow-up (25). One prospective study reveals that only a limited number of the cohort of patients with subclinical hypothyroidism develop overt hypothyroidism over time and the majority remain in the subclinical state after 10 years (24). Hence, it is reasonable to assume that this stability in thyroid function tests is present among euthyroid subjects over long periods of time. Moreover, in the case of high serum TSH with normal FT4 levels, spontaneous normalization of TSH has been observed (26,27). A study by Rosário et al. showed that most patients with subclinical hypothyroidism and a TSH ≤10 mU/L did not progress to overt hypothyroidism and after 3 years of follow-up, spontaneous normalization of TSH levels was observed in 20% of the study population (26). However, some may say that subclinical hypothyroidism might be an independent risk factor for cardiovascular and metabolic events, requiring therapeutic intervention regardless of spontaneous normalization or persistence. The significantly higher risk of these adverse events among our patients with early hypothyroidism might support this hypothesis. Interventional studies need to assess whether therapeutic interventions are necessary for patients with early diagnosis of hypothyroidism and subclinical hypothyroidism.
There is evidence supporting our results demonstrating that TPOAb are a risk factor for progression to thyroid hypofunction (16,24,27). In the Whickham study, subjects with subclinical hypothyroidism and TPOAb negative status had at least a 2–3% annual risk of conversion to overt hypothyroidism, a rate that almost doubled (4–5%) if TPOAb were present (16). Some studies reveal that euthyroid individuals with positive TPOAb levels have at least a 2% annual rate of progression to subclinical or overt hypothyroidism, whereas antibody negative euthyroid subjects have lower rates compared with the studies mentioned above (16,17).
Our study does have some limitations. First, although a detailed history was obtained at the time of the baseline examination, drug history was self-reported. Second, the study has a follow-up period of six years, which is not that long. Moreover, this study is underpowered to investigate subclinical (n = 23) and overt (n = 17) hyperthyroidism, for which much larger numbers are needed. The study also has several strengths. First, free serum T4 was measured, so that thyroid status is more credible than if total T4 concentrations were available. Second, to our knowledge, this study is one of the few studies aiming to determine the natural course of thyroid function in a euthyroid population and third, the study has a prospective nature with follow ups every three years. We should note that, these data are of no direct clinical relevance and merely provide insight into the natural course of euthyroid thyroid function.
In conclusion, our data clearly demonstrate that over 93% of euthyroid subjects remained euthyroid over six years of follow-up and that the factors predicting progression to thyroid dysfunction are baseline TSH, FT4, TPOAb levels, sex, and smoking.
Footnotes
Acknowledgments
We would like to express our gratitude the laboratory personnel of the RIES for their assistance and to acknowledge Ms. Niloofar Shiva for critical editing of English grammar and syntax of the manuscript. This study was supported by financial grants from the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
A.A. and F.Z. contributed to conception and design of trial, collection and assembly of data, interpretation of data, manuscript writing, and final approval of manuscript. M.B. and S.G. conducted the statistical analyses. M.B. and Z.G. wrote the primary draft of manuscript. L.M. and M.T. contributed to collection and assembly of data and manuscript writing. All authors contributed to and have approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.